ES Dellon et al. Clin Gastroenterol Hepatol 2022; https://doi.org/10.1016/j.cgh.2022.02.013 (Ahead of print) Open Access: Fluticasone Propionate Orally Disintegrating Tablet (APT-1011) for Eosinophilic Esophagitis: Randomized Controlled Trial
Methods: In this randomized, double-blind, placebo-controlled, dose-finding, phase 2b trial, 106 adults with EoE received 1 of 4 APT-1011 (fluticasone propionate oral disintegrating tablet) doses or placebo for a 12-week induction period and 40 weeks of maintenance.
Key findings:
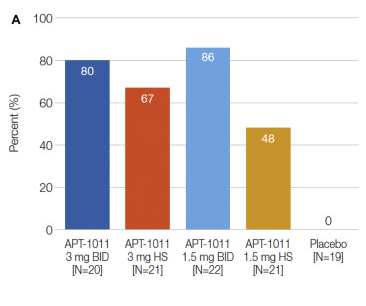
- Histologic response (≤6 eosinophils per high-power field at Week 12) rates were 0% for placebo, 80% for APT-1011 3 mg twice daily (BID), 67% for 3 mg at bedtime (HS), 86% for 1.5 mg BID, 48% for 1.5 mg HS (P < .001 for all groups vs placebo).
- There was also improvement in treatment group in dysphagia and EoE Endoscopic Reference Score (EREFS); the EREFS improved from 4.5 to 2.3 for 3 mg BID, 5.3 to 2.1 for 3 mg HS, 4.6 to 1.7 for 1.5 mg BID, 5.3 to 2.9 for 1.5 mg HS vs 5.2 to 4.5 for placebo. See Figure 2 for 52 week trend in EREFS.
- Candidiasis: For the 3-mg BID group, oral and esophageal candidiasis was 40% in Part 1 and 32% in Part 2, 18% and 16% for 1.5 mg BID, and 5% and 7% for 3 mg HS (same subject)
- Low morning cortisol noted 3 times in part 1 and 5 times in part 2. “All cortisol test abnormalities resolved upon retesting, with no dose adjustment or interruption of treatment.” Adrenal suppression is expected to be low because “FP undergoes extensive first-pass metabolism to inactive metabolites, with bioavailability demonstrated as <1%”
My take: A fluticasone ODT would represent a big improvement compared to current situation of asking families to either spray a pulmonary inhaler down their throat or to create a budesonide slurry using either honey or splenda. How much would this cost?
Related blog posts:
- Surprising Findings in Prospective Budesonide-Eosinophilic Esophagitis Study
- Higher Doses of Topical Steroids for Eosinophilic … – gutsandgrowth
- Genetic Basis of EoE
- Expecting Change in EoE Treatment
- 4-14-4 Rule: More Biopsies Recommended for EoE
- 2020 Eosinophilic Guidelines (AGA)
- Eosinophilic Esophagitis -FAQs
- What Happens When Topical Steroids Are Stopped in EoE?
- How Genetics Influence Response to PPIs in Eosinophilic Esophagitis