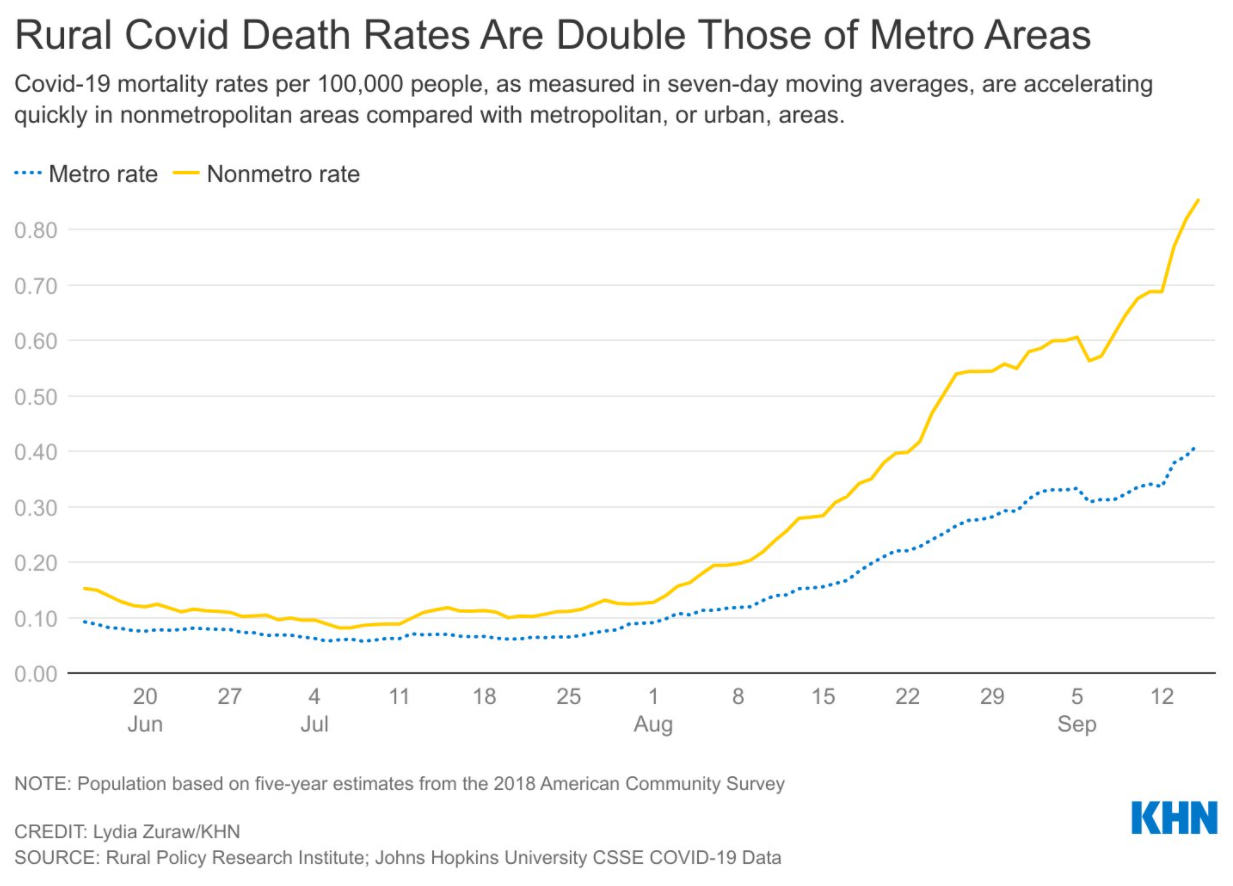

From NBC News: Covid is killing rural Americans at twice the rate of people in urban areas




From NBC News: Covid is killing rural Americans at twice the rate of people in urban areas
I want to recognize Dr. Bess Schoen. Bess is a colleague at Emory. I met her when I was a 4th year medical student. Since we work at different hospitals, I do not see her often but greatly respect her and her work.
From one of my colleagues, Tanya Hofmekler:
This month, we are celebrating Dr. Bess Schoen’s retirement and her long career in academic medicine. She will be greatly missed. Dr. Schoen has always modeled the best characteristics of a well-rounded academic physician. On top of those, she is smart, an excellent teacher and is an overall wonderful person. She has trained and impacted many residents and fellows that have passed through Emory. Her trainees walk away with practical medical knowledge and an example of compassionate care. As one of her trainees, I find myself from time to time asking: “What would Dr. Schoen do?”
Dr. Schoen has also dedicated herself to improve the care of pediatric patients with Inflammatory Bowel Disease through her leadership of Improve Care Now at Emory. This year, she will be honored by the Crohn’s and Colitis Foundation of America for her commitment and passion.

J Liu. Inflamm Bowel Dis 2021; 27: 1548-1549. Disparity in the Care of Black Inflammatory Bowel Disease Patients
This first-hand account of the challenges of IBD care for black patients comes from the first IBD specialist recruited to Grady Hospital (Atlanta) which has a predominantly Black patient population.
Key points:
My take: Inflammatory bowel disease is definitely a disease that affects Black people; it is often more severe and requires careful treatment.

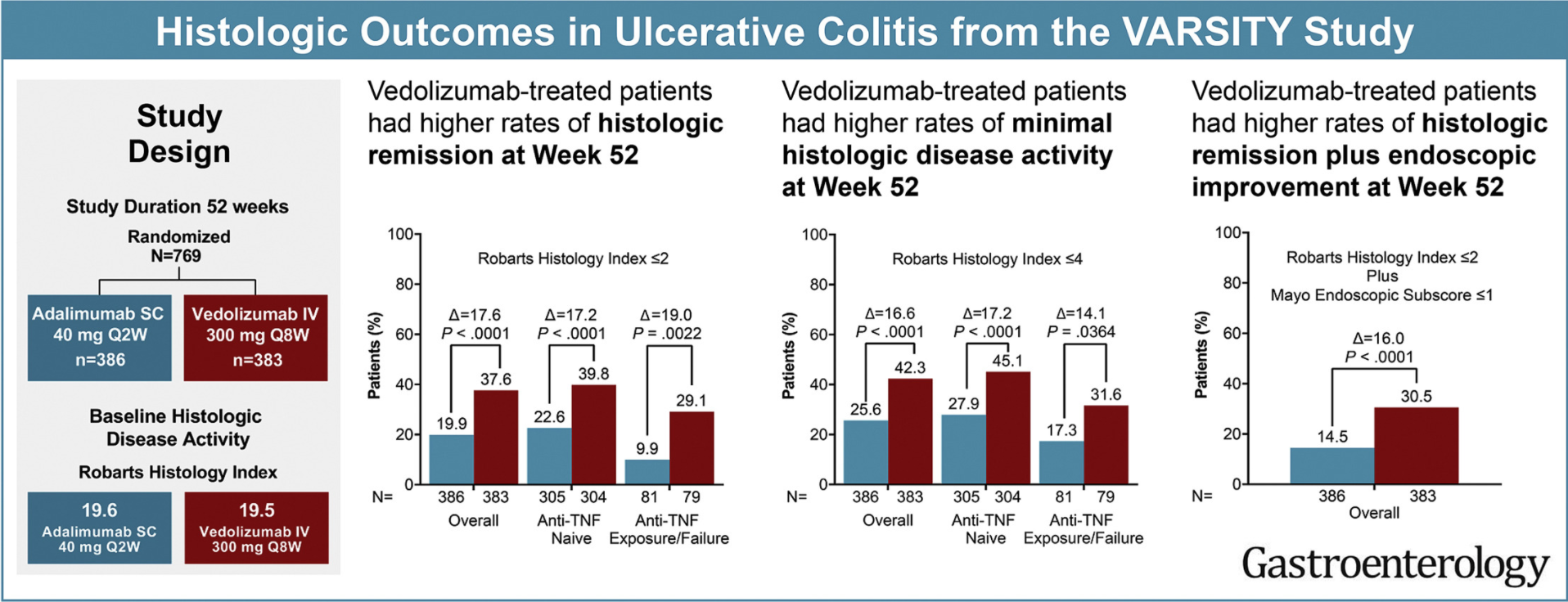
L Peyrin-Biroulet et al. Gastroenterol 2021; Open Access DOI:https://doi.org/10.1053/j.gastro.2021.06.015. Histologic Outcomes With Vedolizumab Versus Adalimumab in Ulcerative Colitis: Results From An Efficacy and Safety Study of Vedolizumab Intravenous Compared to Adalimumab Subcutaneous in Participants With Ulcerative Colitis (VARSITY)
In total, 769 patients received vedolizumab (n = 383) or adalimumab (n = 386). Geboes Index and Robarts Histopathology Index (RHI) scores were used to assess prespecified histologic exploratory end points of histologic remission (Geboes <2 or RHI ≤2) and minimal histologic disease activity (Geboes ≤3.1 or RHI ≤4) at weeks 14 and 52.
Key findings:
Vedolizumab induced greater histologic remission than adalimumab:
My take: This study shows that histologic outcomes with vedolizumab, similar to clinical outcomes, were better than with adalimumab. Some of this difference could be due to the trail design which did not allow optimization of adalimumab dosing.
Related posts:
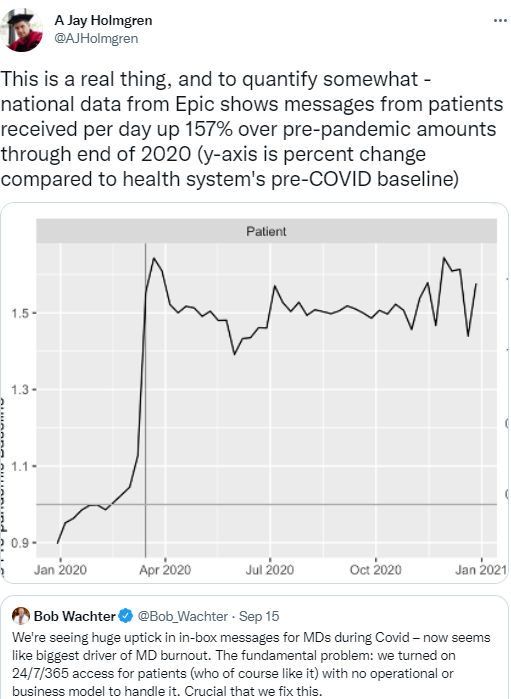
The Verge: Digital messages from patients to doctors spiked during the pandemic (Link from Bryan Vartabedian 33mail)
An excerpt:
Doctors say they’re overwhelmed by the volume of digital messages they receive from patients during the pandemic, and new data backs up their experience. The number of messages increased by over 150 percent at the start of the COVID-19 pandemic, and the levels stayed high over the course of 2020, according to an early look at data from the electronic health record company Epic.
My take: I generally prefer receiving patient information (outside the office) from my nurse rather than directly from patients. Patient messages can contribute to the feeling that you are never done with work. I do like the idea that these portals allow families to let us know if patients have trouble reaching our office.
Related blog posts:
At a recent pharmacy committee meeting, we discussed the potential use of enteral naloxone for ICU patients with opioid-induced constipation.
Background:
Potential alternatives:
Administration:
My take: Enteral naloxone (IV solution) may be helpful for opioid-induced constipation but caution is needed to assure it is administered enterally and at proper dose.
Some of the research studies:
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.

About 10 days ago, I was in Washington D.C. The image below is from my trip.
NPR: More Than 600,000 White Flags On The National Mall Honor Lives Lost To COVID (9/17/21)
An excerpt:
For more than two weeks starting this week, more than 600,000 white flags will fill the National Mall — symbolizing the lives lost to COVID-19 in the United States.
Each of the flags, displayed across the 20 acres of grass, will hold a written personalized message from loved ones honoring their memory.
The art installation, titled In America: Remember, was created by Suzanne Brennan Firstenberg, the Washington, D.C

S-M Wang et al. The American Journal of Gastroenterology: September 2021 – Volume 116 – Issue 9 – p 1844-1852. Open Access: Population Attributable Risks of Subtypes of Esophageal and Gastric Cancers in the United States
This study examined population risks for esophageal squamous cell carcinoma (ESCC), esophageal adenocarcinoma (EAC), gastric cardia adenocarcinoma (GCA), and gastric noncardia adenocarcinoma (GNCA).
“We prospectively examined the associations for risk factors and these cancers in 490,605 people in the National Institutes of Health-the American Association of Retired Persons Diet and Health cohort Diet and Health Study cohort from 1995 to 2011.”
Key findings:

My take: Tobacco, Obesity and Alcohol are associated with increased risk for a large proportion of esophageal and gastric cancers in the United States
Related article: VK Rustgi et al. Gastroenterol 2021; 161: 171-184. Open Access: Bariatric Surgery Reduces Cancer Risk in Adults With Nonalcoholic Fatty Liver Disease and Severe Obesity
Key findings:
Link: Improving Morale (53 seconds)

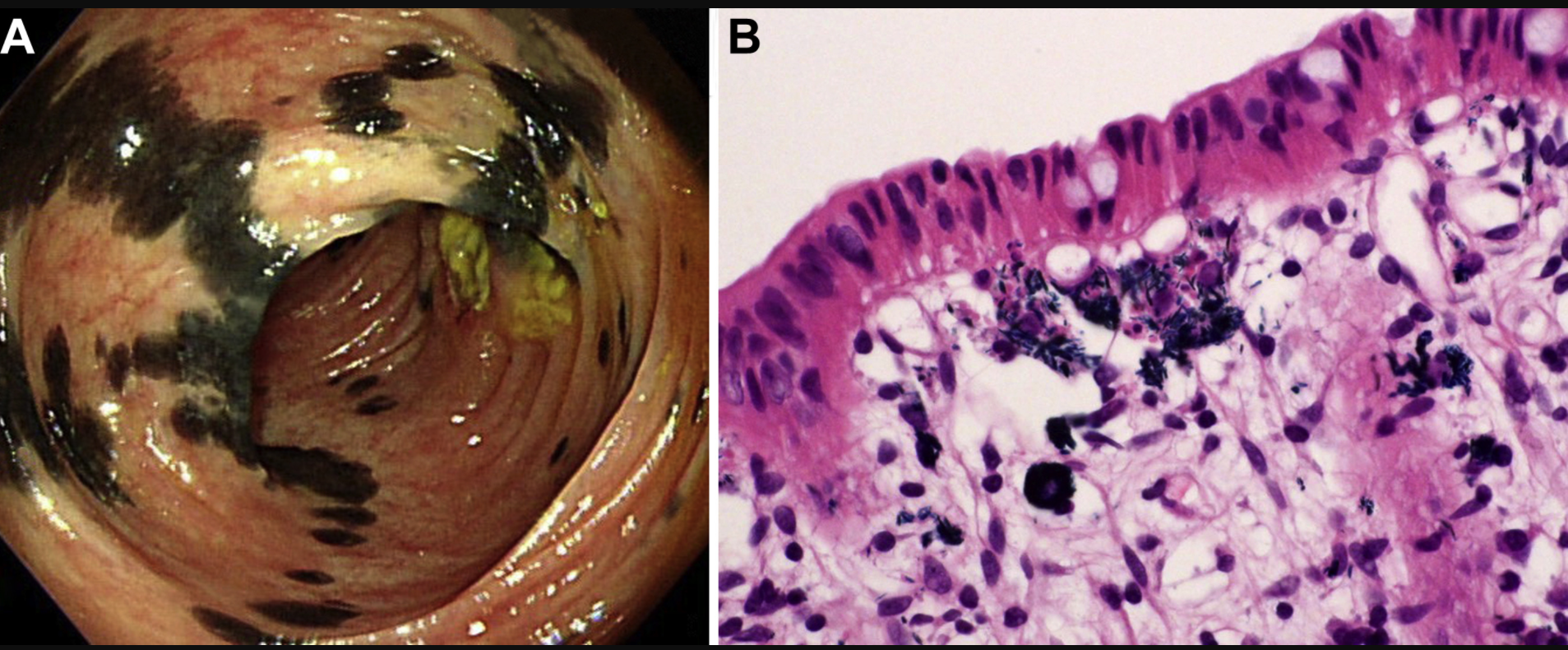
The image below is from a 57 yo woman with Crohn’s disease who was taking a supplement, indigo naturalis (Qing-Dai). “Higher magnification disclosed bluish, needle-like crystals in the cytoplasm of these histiocytes. In light of the presence of pigment-laden histiocytes, we called the lesions indigo naturalis-related pseudomelanosis. Unlike melanosis coli, which typically shows continuous homogeneous brown or black discoloration of colon mucosa (snake-skin appearance or starry sky appearance), indigo naturalis-related pseudomelanosis exhibits a haphazard distribution of black discoloration reminiscent of the skin markings of Holstein Friesian cattle…It remains to be seen whether deposition of indigo naturalis has any long-term adverse effect, although histologically the mucosa with indigo deposition was not accompanied by significant inflammatory activity.”
Link: P-H Le et al. Gastroenterol 2021; 161: e10-e11. Colonic Bluish–Black Patches in a 57-Year-Old Woman with Crohn’s Disease
C Madre et al. JPGN 2021; 73: 333-337. A European Survey on Digestive Perianastomotic Ulcerations, a Rare Crohn-like Disorder Occurring in Children and Young Adults
This survey study with 51 children described the etiology and treatment of perianastomic ulcerations (PAU).
Key findings:
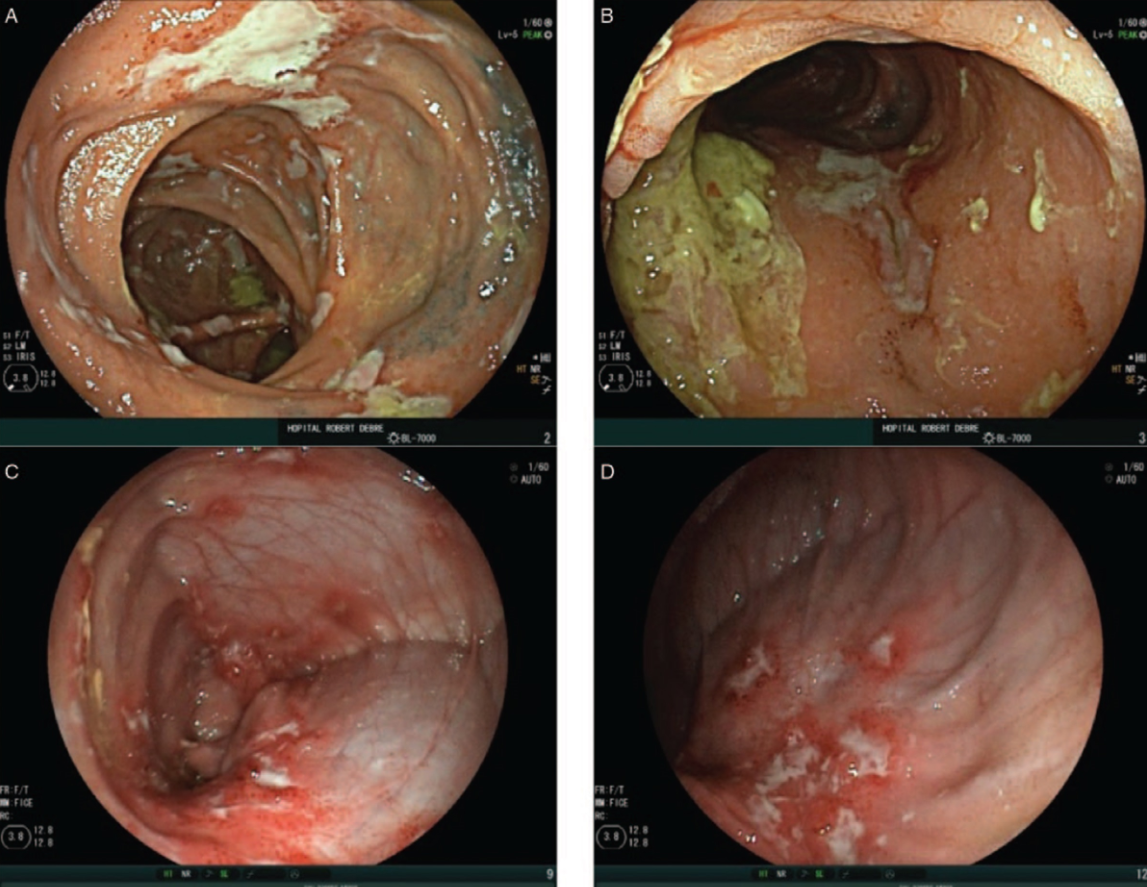
Related article: H Barraclough et al. JPGN 2021; 73: 329-332. Anastomotic Ulcers: A Tertiary Centre Experience of Endoscopic Management Techniques This study summarized a tertiary care center experience with 9 patients (2 with IBD). Frequent treatment included aminosalicylates, and endoscopic treatments (APC, endoclips).
Related blog posts:
