A good Sunday read: Full text: Mammalian enteral ventilation ameliorates respiratory failure (R Okabe et al. Med (2021), https://doi.org/10.1016/j.medj.2021.04.004) -thanks to a friend for forwarding the study.
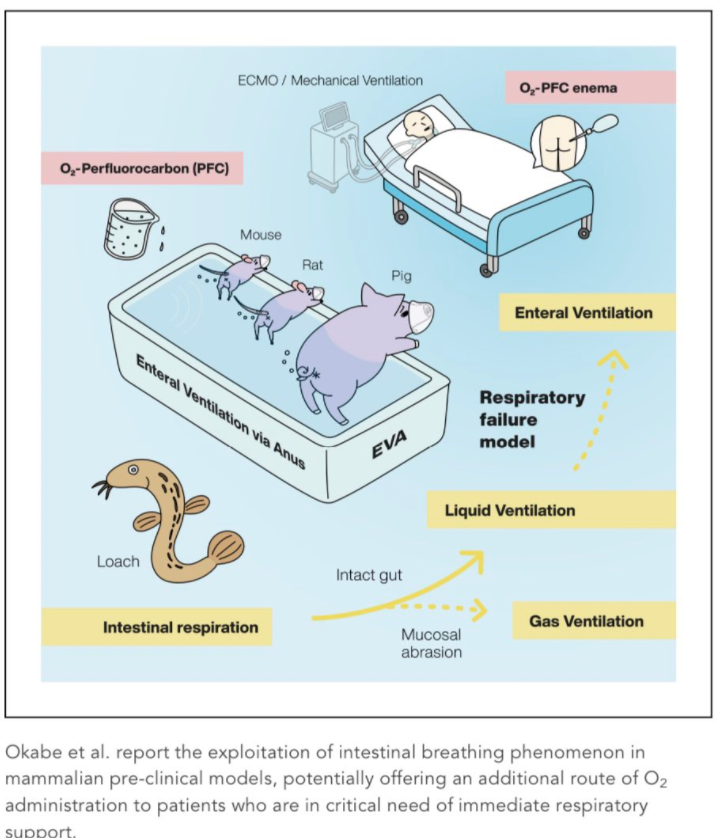
Background: Several aquatic organisms such as loaches have evolved unique intestinal breathing mechanisms to survive under extensive hypoxia. Scientists hope that the approach could one day be used to treat people with low oxygen, without risking the lung damage that can be caused by mechanical ventilators. To date, it is highly controversial whether such capability can be adapted in mammalian species as another site for gas exchange. This study reports the advent of the intestinal breathing phenomenon in mammalians by exploiting EVA (enteral ventilation via anus).
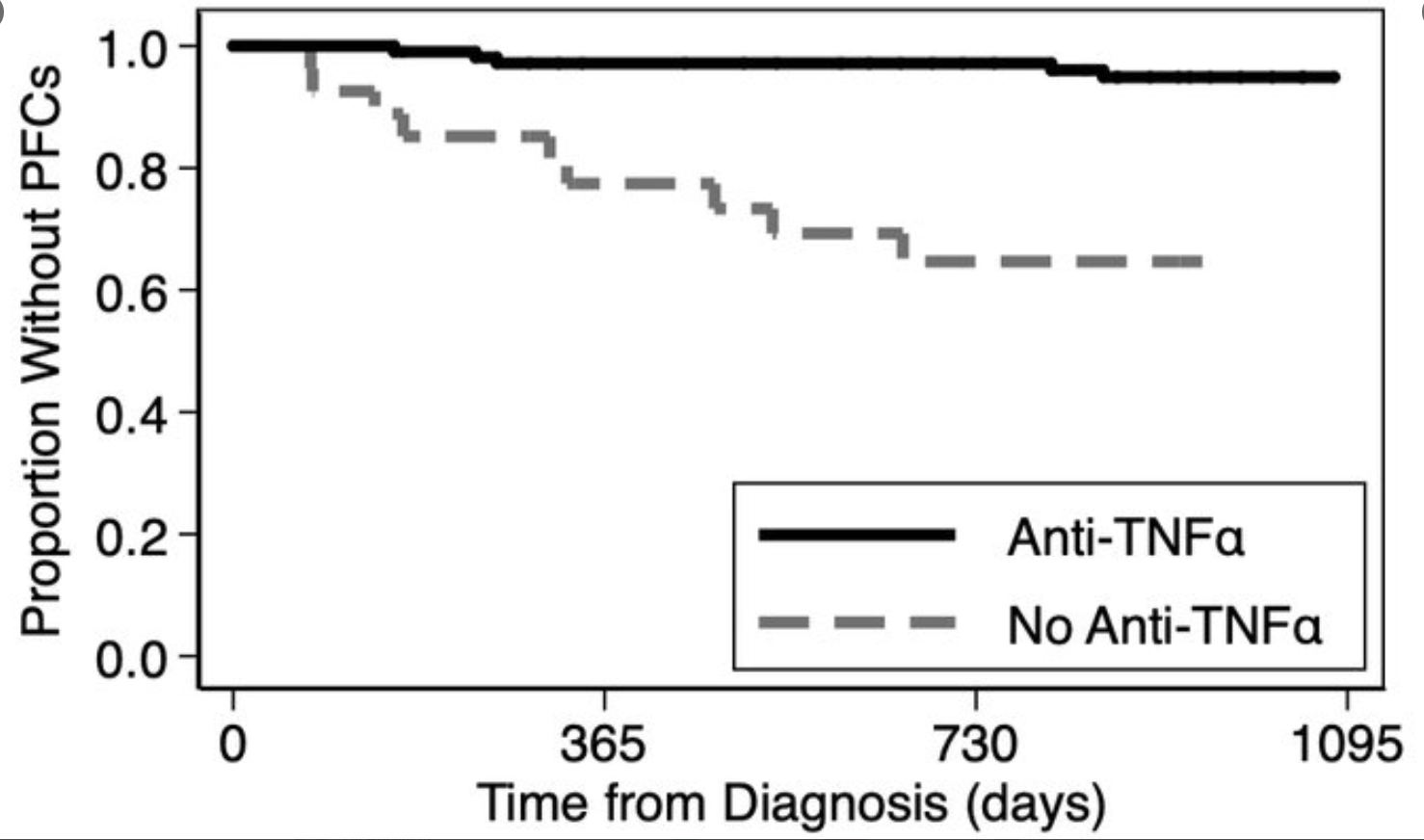
This study showed that administration of oxygen-rich perfluorochemical liquid via the rectum could “increase oxygenation in several mammals including pigs. The level of arterial oxygenation, if scaled for human application, is likely sufficient to alleviate patients with severe respiratory failure. The administration of 200–400 mL PFD to pigs weighing 10–20 kg improved PaO2 by 13 mm Hg (from 57.2 ± 13.5 to 70.8 ± 6.22 mm Hg) and SaO2 by 7% (from 84% to 91%).”
NY Times review of this study: Breathing Through the Rectum Saves Oxygen-Starved Mice and Pigs
My take: It is good that this study was not published on April 1st! Perhaps, if this advances, this will be more work for our aerodigestive team.
.