Related blog posts:





Diagnosis of constipation is primarily based on history and physical exam –not abdominal xray (AXR). In a recent quality improvement study (G Moriel et al. J Pediatr 2020; 225: 109-116. Reducing Abdominal Radiographs to Diagnose Constipation in the Pediatric Emergency Department), ED physicians were trying to improve adherence to evidence-based guidelines for diagnosis of constipation in otherwise healthy children. In this article, the authors note evidence “has shown abdominal radiographs to be unreliable in establishing an association between clinical symptoms of constipation and fecal load on abdominal radiographs.”
As part of the study, the researchers provided two 20-minute presentations to the pediatric emergency department providers and sent emails to them and to resident housestaff. The email for ED provider’s included the provider’s baseline abdominal radiograph frequency. After study was initiated, a followup email was sent with similar information with key information on the project along with individualized data.
Key findings:
One interesting piece of data was showing that this intervention resulted in a sustained reduction for 12 months after the intervention observation period, which mitigates the potential influence of the Hawthorne effect.
My take: In my view, the keys to this intervention was providing individualized metrics as well as having leadership in establishing this project. The individualized metrics help physicians recognize when they are outliers and to motivate them to address this.
Related posts:

A recent study (SE Tarbell et al J Pediatr 2020 225: 109-108. Children with Functional Nausea—Comorbidities outside the Gastrointestinal Tract) highlights the frequent comorbidities in children with functional nausea. The authors have combined prospective and retrospective elements with specific questionnaires and review of the electronic medical records.
Key points:
Overall, this article makes some useful points about the high rate of comorbidities with functional nausea but I disagree with some of the other discussion points.
The authors claim that “negative tests can reassure families of the absence of a more serious underlying condition.” This assertion has been disputed in other studies. In one study (A Rolfe et al. JAMA Intern Med. 2013;173(6):407-416 Full text: Reassurance After Diagnostic Testing With a Low Pretest Probability of Serious Disease), the authors conclude that ‘diagnostic tests for symptoms with a low risk of serious illness do little to reassure patients, decrease their anxiety, or resolve their symptoms, although the tests may reduce further primary care visits.’
The authors also have a permissive attitude regarding AXRs saying “a radiograph may validate a diagnosis of constipation.” Yet the preponderance of evidence indicates that AXRs are not needed or recommended for the diagnosis of constipation. The juxtaposition of this statement on page 107 of this issue with the next article on page 109 which details a quality improvement process of reducing abdominal radiographs to diagnose constipation in the ED is interesting. The ED physicians in the next article are trying to adhere to evidence-based guidelines; in this article, the authors correctly note that evidence “has shown abdominal radiographs to be unreliable in establishing an association between clinical symptoms of constipation and fecal load on abdominal radiographs.”
My take: Tarbell et al show that in patients with functional nausea, nausea is the tip of the symptom iceberg. Generally, radiographic and endoscopic diagnostic studies have very low yield and should be discouraged.
Related posts:


A recent study (AG Feldman et al. J Pediatr 2020; 225: 252-258. Subacute Liver Failure Following Gene Replacement Therapy for Spinal Muscular Atrophy Type 1) describes two children who developed subacute liver failure after treatment with onasemnogene (AVXS-101). This gene therapy was approved by the FDA in 2019 and more than 335 children have been treated. Both children presented about 3-8 weeks after their AVXS-101 infusion (despite steroid therapy), at 6 months of age and 20 months of age respectively, with ALT values above 1600 and INR of at least 1.5 (despite Vitamin K). Both had liver biospies and then were treated with methylprednisolone, starting at 20 mg/kg/day.
Key points:
My take: This new therapy’s risks are substantial; however, the benefits from treatment can be life-altering as well.
Related blog post: Understanding the New Therapies for Spinal Muscular Atrophy

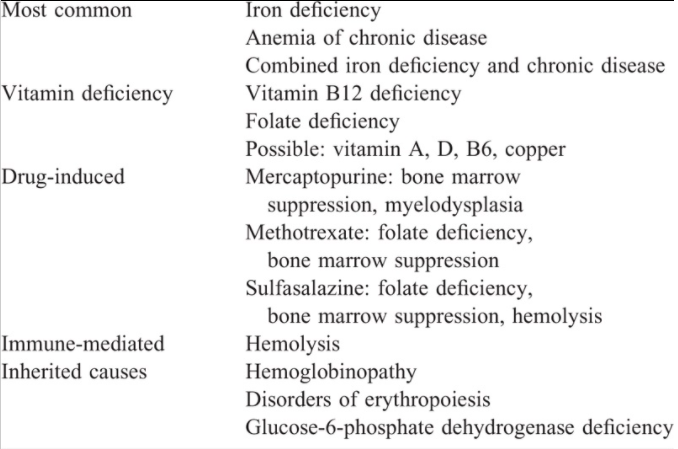
A Goyal et al. JPGN 2020; 71: 563-582 Full text (free). Anemia in Children With Inflammatory Bowel Disease: A Position Paper by the IBD Committee of the North American Society of Pediatric Gastroenterology, Hepatology and Nutrition.
Main Types of Anemia in Inflammatory Bowel Disease:
Table 4:
Recommended Testing
Treatment of Anemia
My take: This is a useful resource for a very common problem.
Related blog posts:
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition
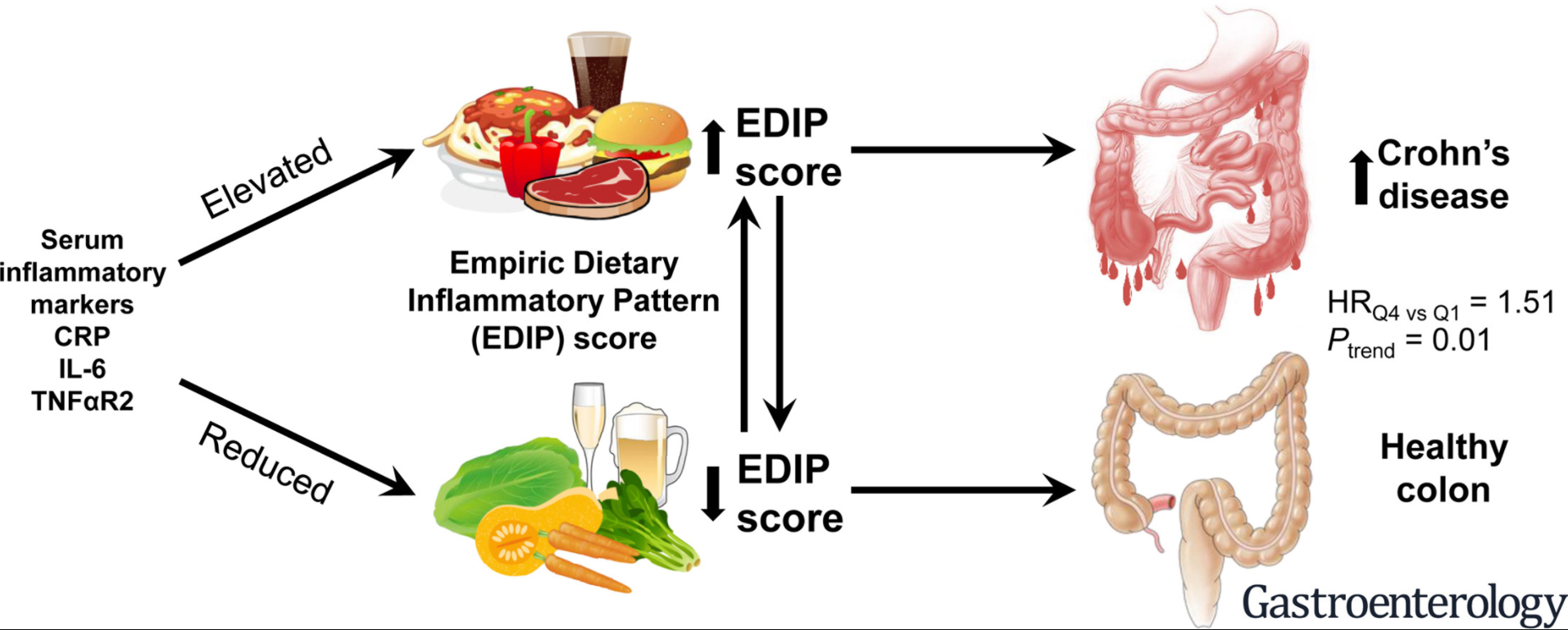
C-H Lo et al. Gastroenterol 2020; 159: 873-883. Full Text Link Dietary Inflammatory Potential and Risk of Crohn’s Disease and Ulcerative Colitis
The authors used Empirical dietary inflammatory pattern (EDIP) scores which were calculated based on the weighted sums of 18 food groups obtained via food frequency questionnaires. n=166,903 women and 41,931 men
Key findings:
Discussion points:
Related blog posts:
A recent retrospective study (TJ Laborda et al. JPGN 2020; 71: 459-464 Vedolizumab Therapy in Children With Primary Sclerosing Cholangitis: Data From the Pediatric Primary Sclerosing Cholangitis Consortium) indicates that vedolizumab (VDZ) is unlikely to be helpful for primary sclerosing cholangits (PSC).
VDZ was initiated at median age of 16 years [IQR 15–18], 69% were male, 65% had large duct involvement, 19% had (Metavir F3/F4) fibrosis and 59% had ulcerative colitis.
Key findings:
In the discussion, the authors note that their findings are in agreement with three retrospective studies in adults which have shown that VDZ is not effective for PSC in patients with IBD.
My take: This study indicates that VDZ is not likely to help with PSC, though 62% of IBD patients had improvement in their GI disease.

K Cheng et al. JPGN 2020; 71: 452-458. Cholangitis in Patients With Biliary Atresia Receiving Hepatoportoenterostomy: A National Database Study
This study, which relied on data from a pediatric database (PHIS) with 48 pediatric centers, identified 1112 subjects with biliary atresia (2004-2013).
Key findings:
My take: Cholangitis is a common problem following hepatoportoenterostomy. Earlier diagnosis of biliary atresia provides the best opportunity for improving long-term outcomes.
Related blog posts:
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.