Briefly noted: GR D’Haens, C Jobin. Gastroenterol 2019; 157: 624-36. This review sums up the emerging evidence for use of fecal microbial transplantation for conditions besides recurrent Clostridium difficile infection.
Table 2 succinctly provides list of disease, types of study/evidence, and potential effect.
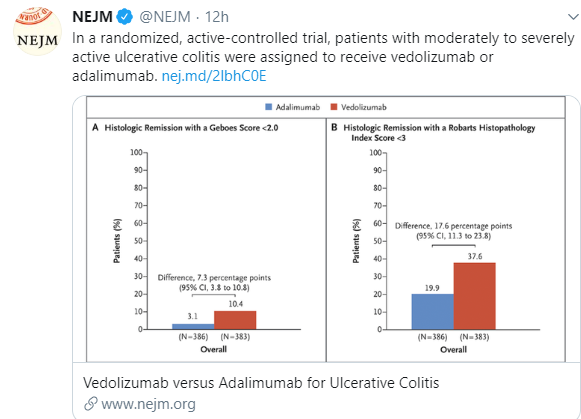
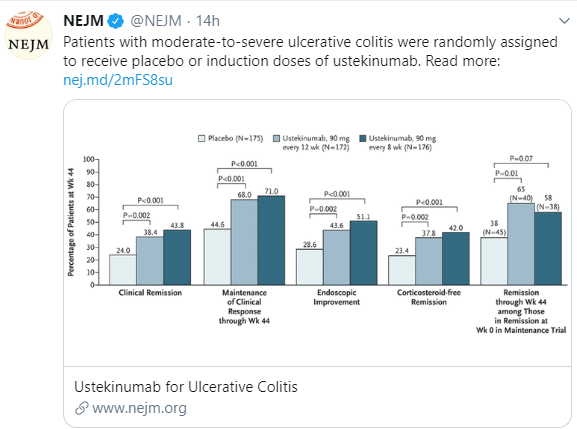
- Among gastrointestinal diseases, the authors note that there is an “overall positive” effect for ulcerative colitis, “suggestive” benefits for IBS, GVHD, post-antibiotic diarrhea, constipation, and hepatic encephalopathy. No effect has been evident with Crohn’s disease or pouchitis.
- Among nongastrointestinal diseases, the authors note a “suggestive” benefit in autism and metabolic syndrome and “unknown” effect with psoriasis and multiple sclerosis.
My take: The review indicates a need for more studies and the need to define which factors in fecal material mediate the therapeutic effects.
Related article: OC Aroniadis. Lancet Gastroenterology and Hepatology; 2019. https://doi.org/10.1016/S2468-1253(19)30198-0. In this double-blind, randomized, placebo-controlled crossover trial in patients aged 18–65 years with moderate-to-severe IBS-D with 48 patients, FMT (capsule study) was safe, but did not induce symptom relief at 12 weeks compared with placebo.
Related blog posts:
- “Intestinal Microbiota Transplant” -better terminology for FMT
- Experimental Use of FMT for Ulcerative Colitis
- FDA Warning for FMT
- Consensus Guidelines on FMT
- Clostridium difficile/Fecal Microbiota Transplantation Video
- OpenBiome -Nation’s 1st Human Stool Bank