


From NY Times: How Big Business Got Brazil Hooked on Junk Food

Excerpt from article:
Across the world, more people are now obese than underweight. At the same time, scientists say, the growing availability of high-calorie, nutrient-poor foods is generating a new type of malnutrition, one in which a growing number of people are both overweight and undernourished…
For a growing number of nutritionists, the obesity epidemic is inextricably linked to the sales of packaged foods, which grew 25 percent worldwide from 2011 to 2016, compared with 10 percent in the United States, according to Euromonitor, a market research firm. An even starker shift took place with carbonated soft drinks; sales in Latin America have doubled since 2000, overtaking sales in North America in 2013, the World Health Organization reported…
In many ways, Brazil is a microcosm of how growing incomes and government policies have led to longer, better lives and largely eradicated hunger. But now the country faces a stark new nutrition challenge: over the last decade, the country’s obesity rate has nearly doubled to 20 percent, and the portion of people who are overweight has nearly tripled to 58 percent. Each year, 300,000 people are diagnosed with Type II diabetes, a condition with strong links to obesity.
From Healio Gastro: AGA releases guidelines on therapeutic drug monitoring in IBD
Key points from Healio Gastro for Adult Patients with IBD:
Reference: JD Feuerstein et al. Gastroenterol 2017; 153: 827-34. Technical review: NV Casteele et al. Gastroenterol 2017; 153: 835-57.
My take: Therapeutic monitoring has become widespread and is quite helpful. My impression is that most pediatric gastroenterologists have adopted both proactive and reactive monitoring.
Related blog posts:

Looking towards the top of John Rock Hike, near Brevard, NC
Bloomberg news: Don’t Yelp Your Doctor. Study Finds Ratings Are All Wrong.
Here’s an excerpt:
If you’re looking for the best doctor, online ratings are unlikely to be much help.
That’s the determination of researchers at Cedars-Sinai Medical Center in Los Angeles, who compared reviews of 78 of the medical center’s specialists on five popular ratings sites with a set of internal quality measures and found there was essentially no correlation…
Brennan Spiegel, a gastroenterologist and co-author of the study, said that may be the right way to think about reviews — as gauges of things the patient can observe.
“It may be that these ratings are a good measure of the front-office service or the interpersonal style of the physician,” said Spiegel, a professor and director of health services research at Cedars-Sinai. “We’re not saying that there’s no value to these online ratings — we’re saying don’t confuse those ratings in any way, shape or form with the actual technical skill.”
The study, published online on Friday in the Journal of the American Medical Informatics Association, compared measures developed by Cedars-Sinai with users’ ratings on five sites: Healthgrades, Yelp, Vitals, RateMDs and UCompareHealthCare. The internal performance metrics include reviews from doctors’ colleagues and administrators, how often patients are readmitted and how long they remain in the hospital, and adherence to practice guidelines.
My take: I’ve been told that the key to patient care are the 3 A’s: availability, affability, and ability. Online evaluations likely can help assess the first two A’s; in addition, these sites allow for constructive criticisms but they need to evolve to include other measures of physician performance. Nevertheless, ignoring online evaluations (eg. digital reputation) would be a mistake for physicians –they are here to stay.
Related blog posts:

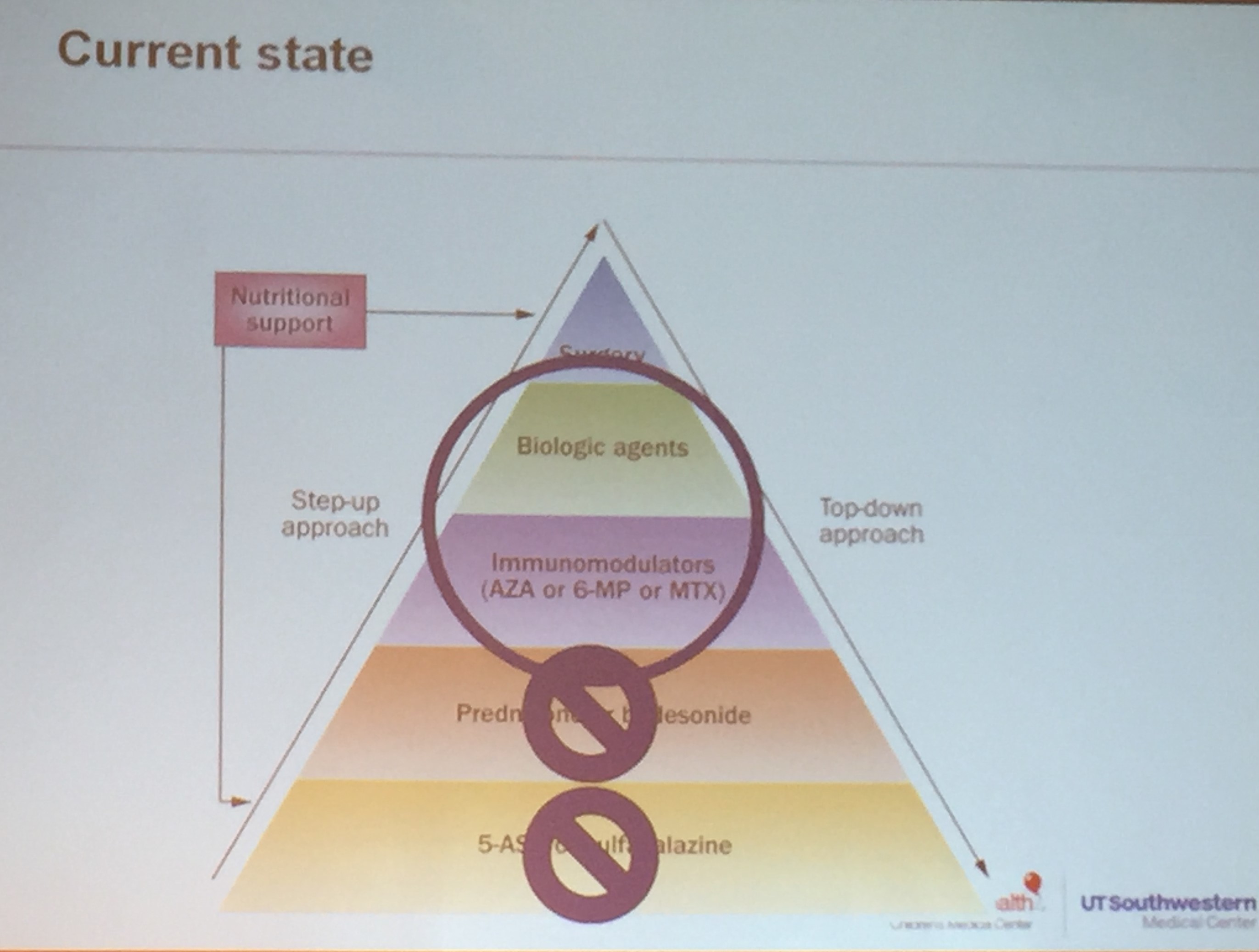
Our local CCFA chapter provided a useful physician CME meeting. The following are my notes. My notes may include some errors in transcription and errors of omission.
Ashish Patel -Updates in Pediatric Inflammatory Bowel Disease Treatments
Key points:



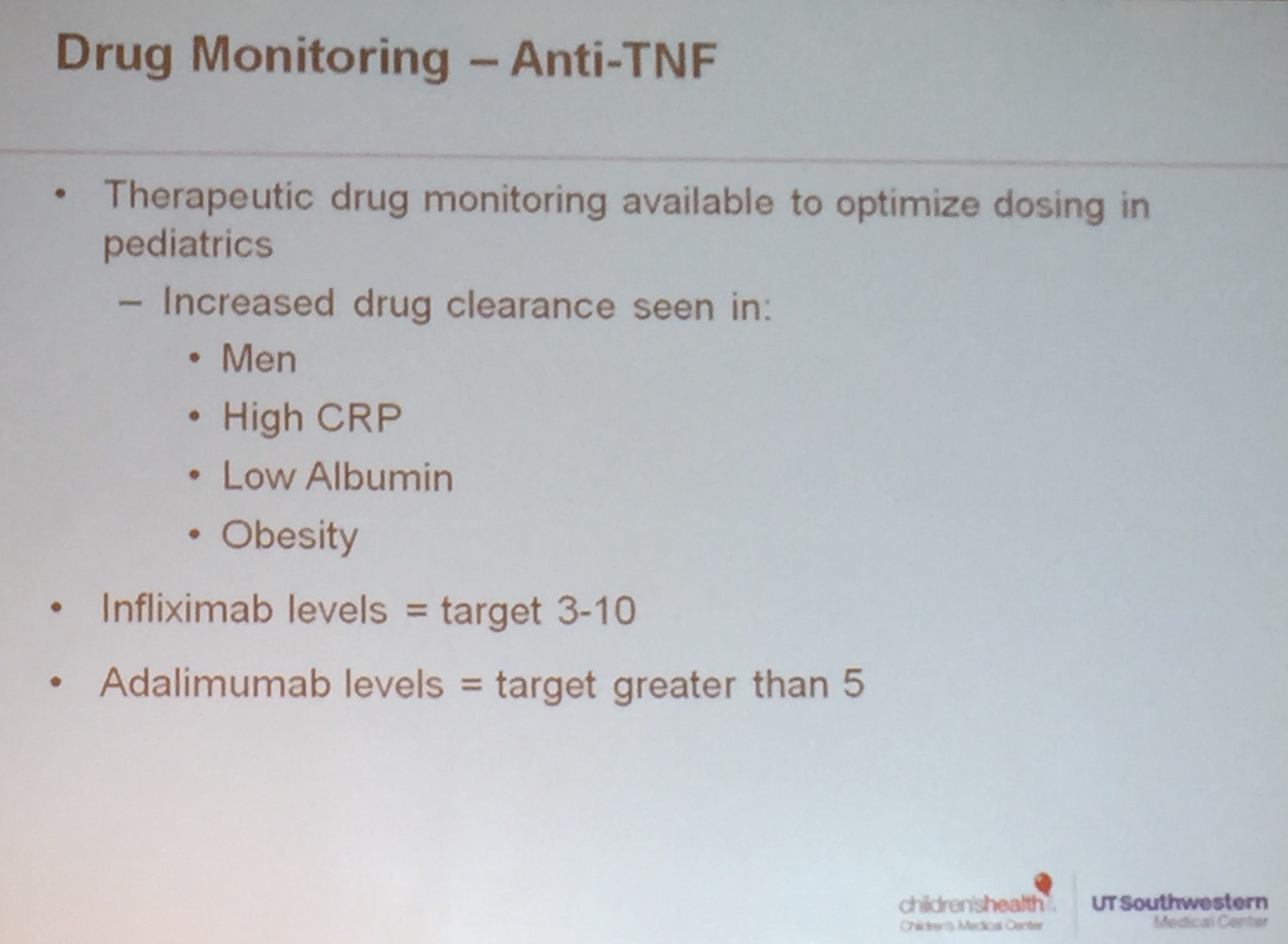


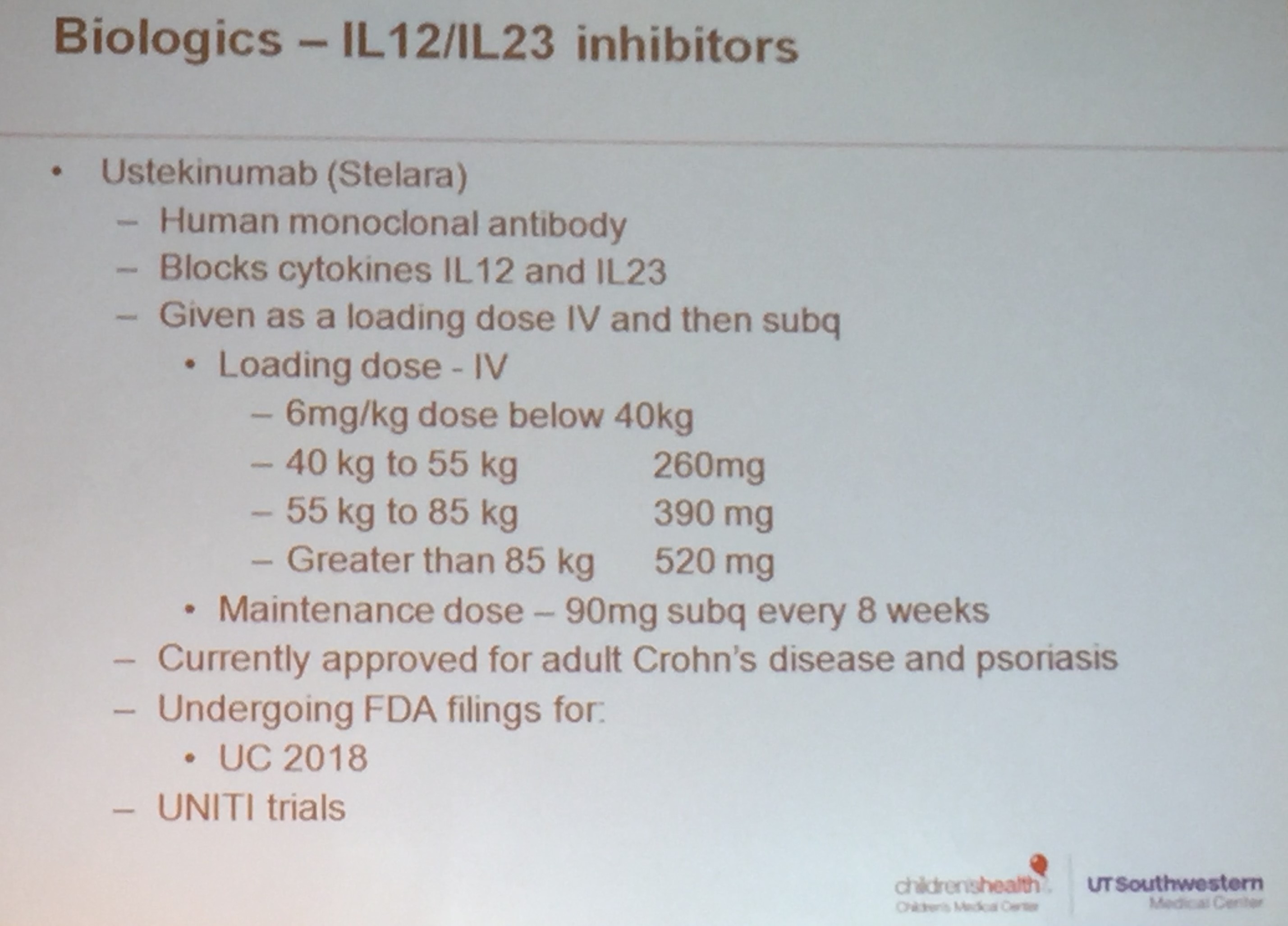



Disclaimer: These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) and changes in diet should be confirmed by prescribing physician. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
A recent retrospective study (GT Wahbeh et al. JPGN 2017; 65: 289-92) examined seven patients who were receiving a modified specific carbohydrate diet (SCD). While this is a small stud,y there are several lessons in this report and the thoughtful editorial (pg 266-67): “Alas, Who and What Can We Trust? Patients, Parents, Surrogate Markers of the Specific Carbohydrate Diet” by Stan Cohen (one of my partners).
The participants in the study had a median age of 11 yrs and received their mSCD for a median duration of 26 months. Key finding: despite lack of symptoms, all subjects had ongoing active disease on endoscopy; the majority had normal biomarkers: CRP, albumin, and hematocrit and only mildly elevated calprotectin (median 201, range 65-312).
Dr. Cohen notes the following lessons from this study:
My take: The modified SCD appears to be only partly effective and how this impacts the long-term outcomes for patients is not clear.
Related article: A McCombie. JPGN 2017; 65: 311-13. Summer camp for IBD. This study of 36 participants: “most reported that camp improved their confidence (86%), acceptance (83%), and overall quality of life (75%). 72% endorsed meeting their fellow campers as the most beneficial experience. My take: Camp helps ease social isolation associated with a diagnosis of pediatric IBD.
Related blog posts:

A recent study (J Sieczkowska-Golub et al. JPGN 2017; 65: 285-88) reports on 36 pediatric patients who received CT-P13, an infliximab biosimilar. Key findings:
The authors concluded that the induction was effective and similar to the reference infliximab.
In the accompanying editorial, Dr. de Ridder and Dr. Winter make some crucial observations:
My take: We still have a lot to learn. Until more studies are available, switching stable patients could increase risk of losing response.
Related blog posts:

Eiffel Tower
Obeticholic acid was approved last year as a treatment for primary biliary cholangitis (PBC). Now (9/21/17), the FDA warns of 19 deaths associated with Obeticholic Acid, particularly when the medication has been used at higher than recommended dosing.
Link: FDA Warning on Obeticholic Acid
An excerpt:
Nineteen cases of death were identified, of which eight provided information about the patient’s cause of death. The cause of death was reported to be worsening of PBC disease in seven cases, with cardiovascular disease cited in the other case. Seven of these eight cases described patients with moderate to severe decreased liver function who received Ocaliva 5 mg daily, instead of a dose no greater than 10 mg twice weekly as recommended in the label prescribing information for patients with this extent of decreased liver function.

NEJM: The Graham-Cassidy Plan -The Most Harmful ACA-Repeal Bill Yet
An excerpt:
The Graham–Cassidy bill would begin by repealing the individual and employer mandates retroactive to 2016. The Congressional Budget Office (CBO) previously estimated that repeal of the individual and employer mandates would immediately increase the number of uninsured Americans by 15 million or more and increase individual market insurance premiums by 20%…
The Graham–Cassidy formula would shift money from states that expanded Medicaid coverage under the ACA or increased take-up among previously eligible groups to those that did not. It would also shift money from high-cost to low-cost areas…
the bill would permit states to waive the ACA requirements that insurance sold in the individual market cover essential health benefits and that insurers not vary premiums on the basis of health status, thereby restoring the ability of insurers to engage in “medical underwriting” and effectively deny coverage or limit services on the basis of preexisting health condition..
All told, we estimate that under Graham–Cassidy, an additional 21 million people would be without insurance coverage in 2020 and later years, and this figure may be conservative..
It replaces effective coverage programs with a block grant that is inadequate in the aggregate and blind to variations in local costs, shifting considerable risk onto states. It would slash the program that provides health insurance coverage for the poor.

More from our recent CCFA Conference. My notes may include some errors in transcription and errors of omission.
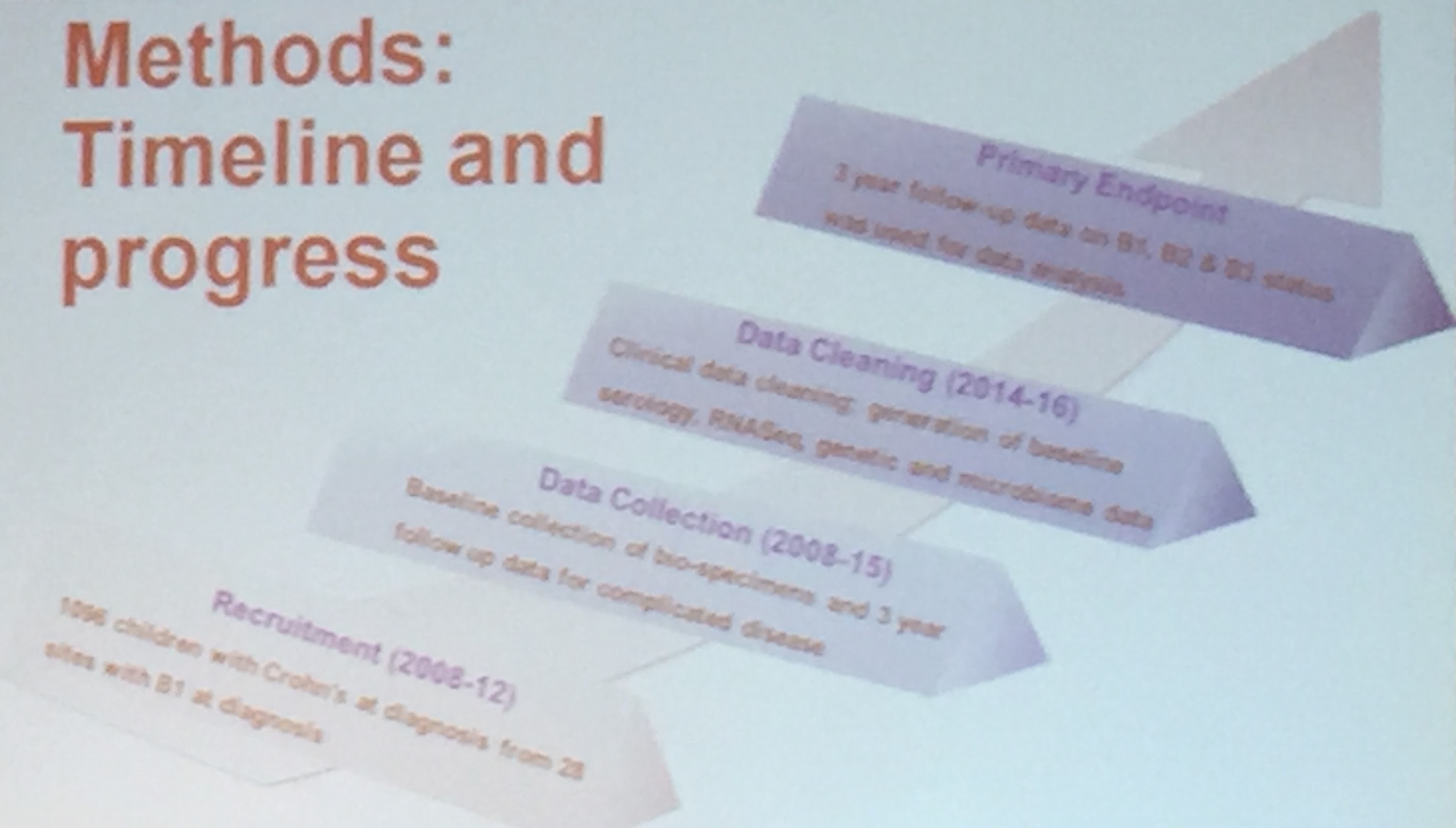
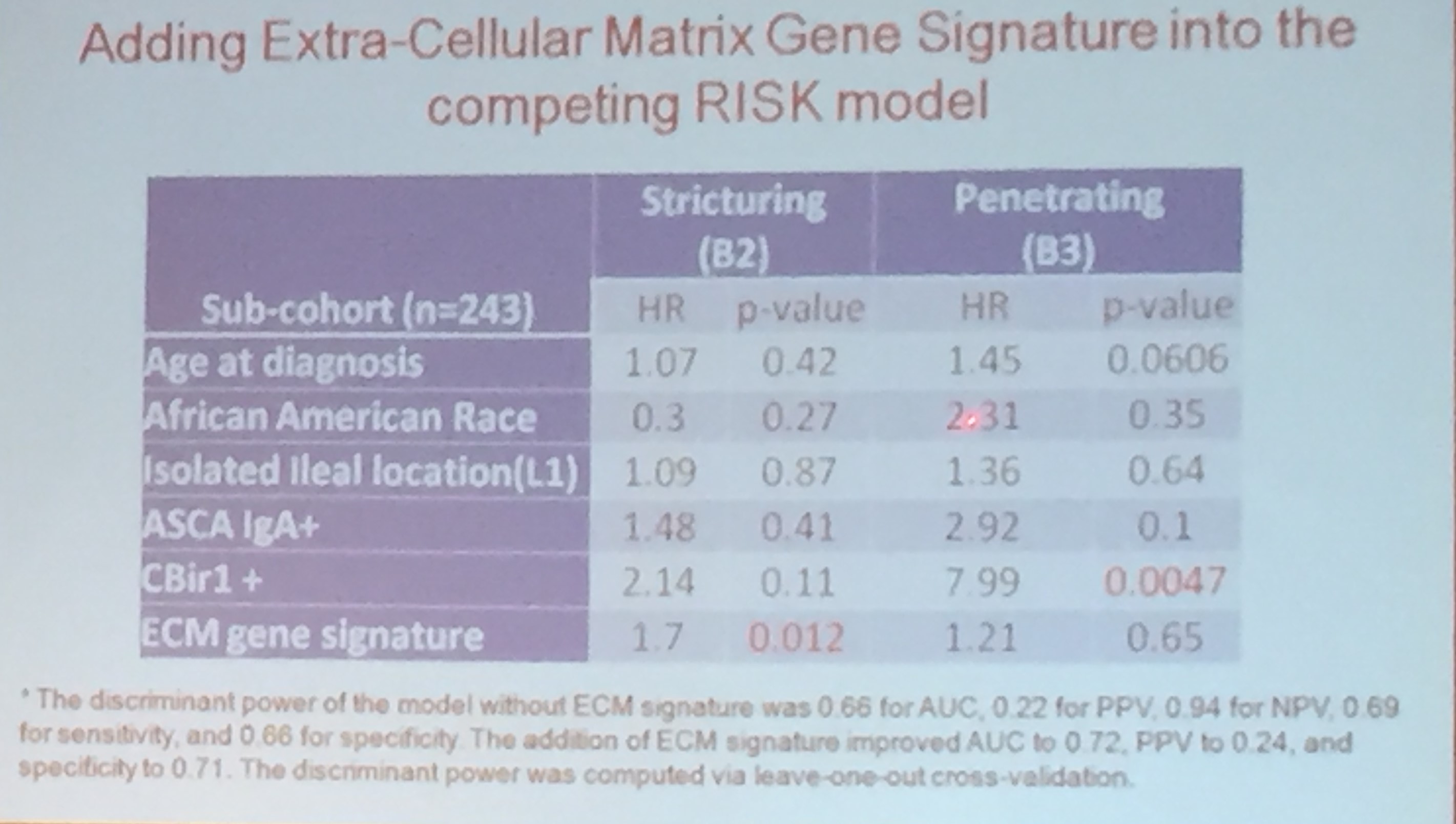
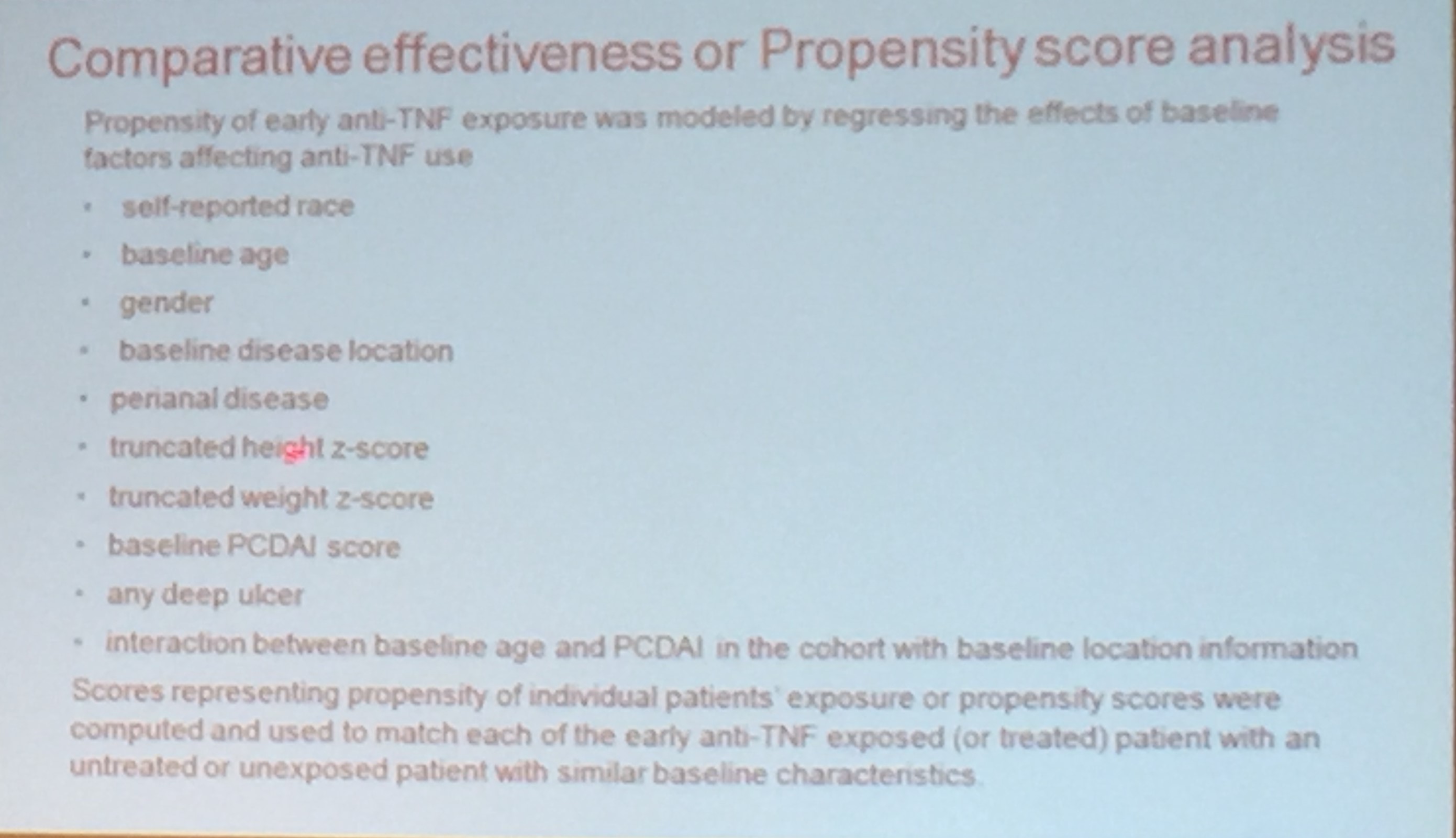
Subra Kugasthasan -RISK Updates
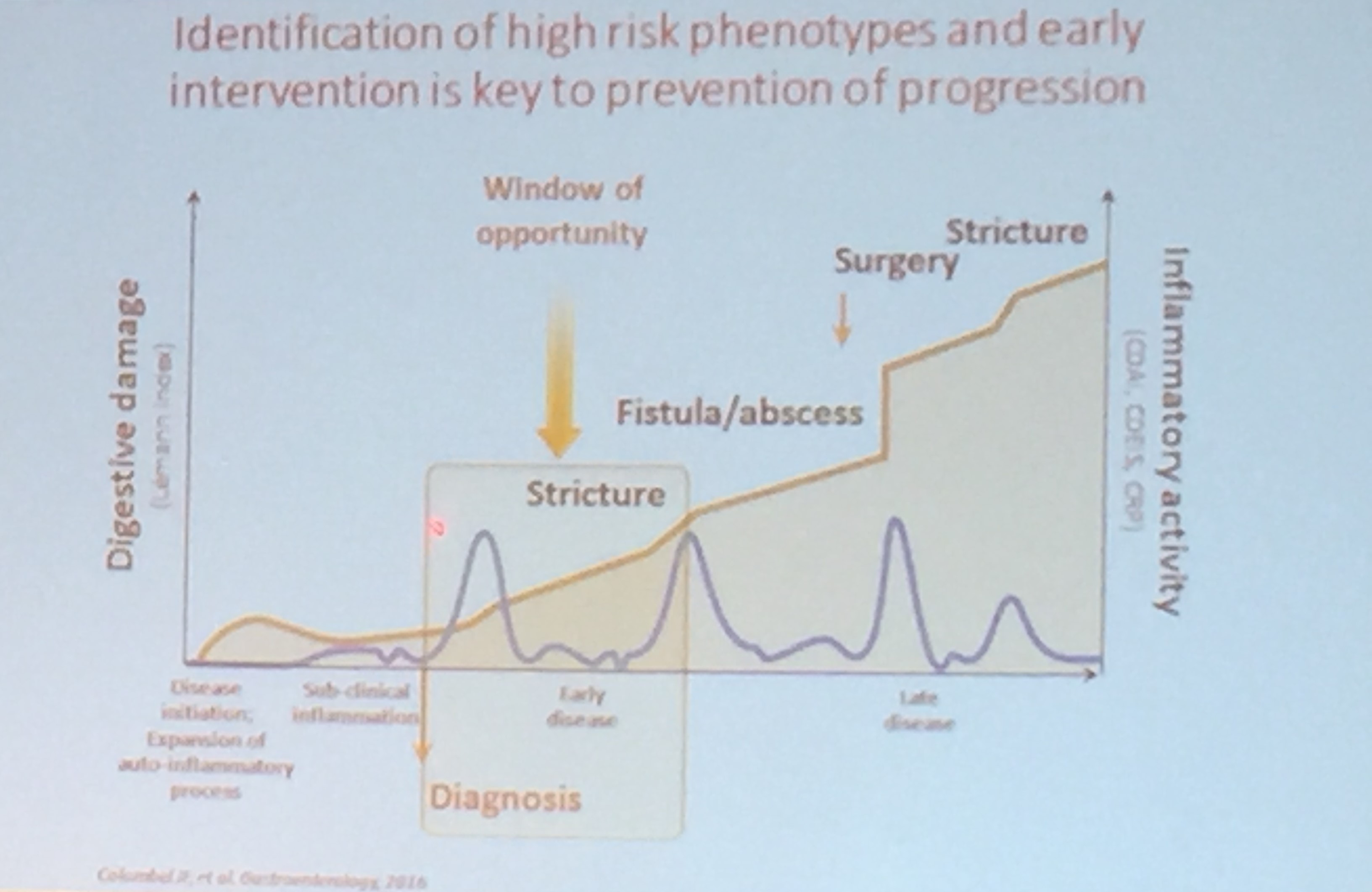
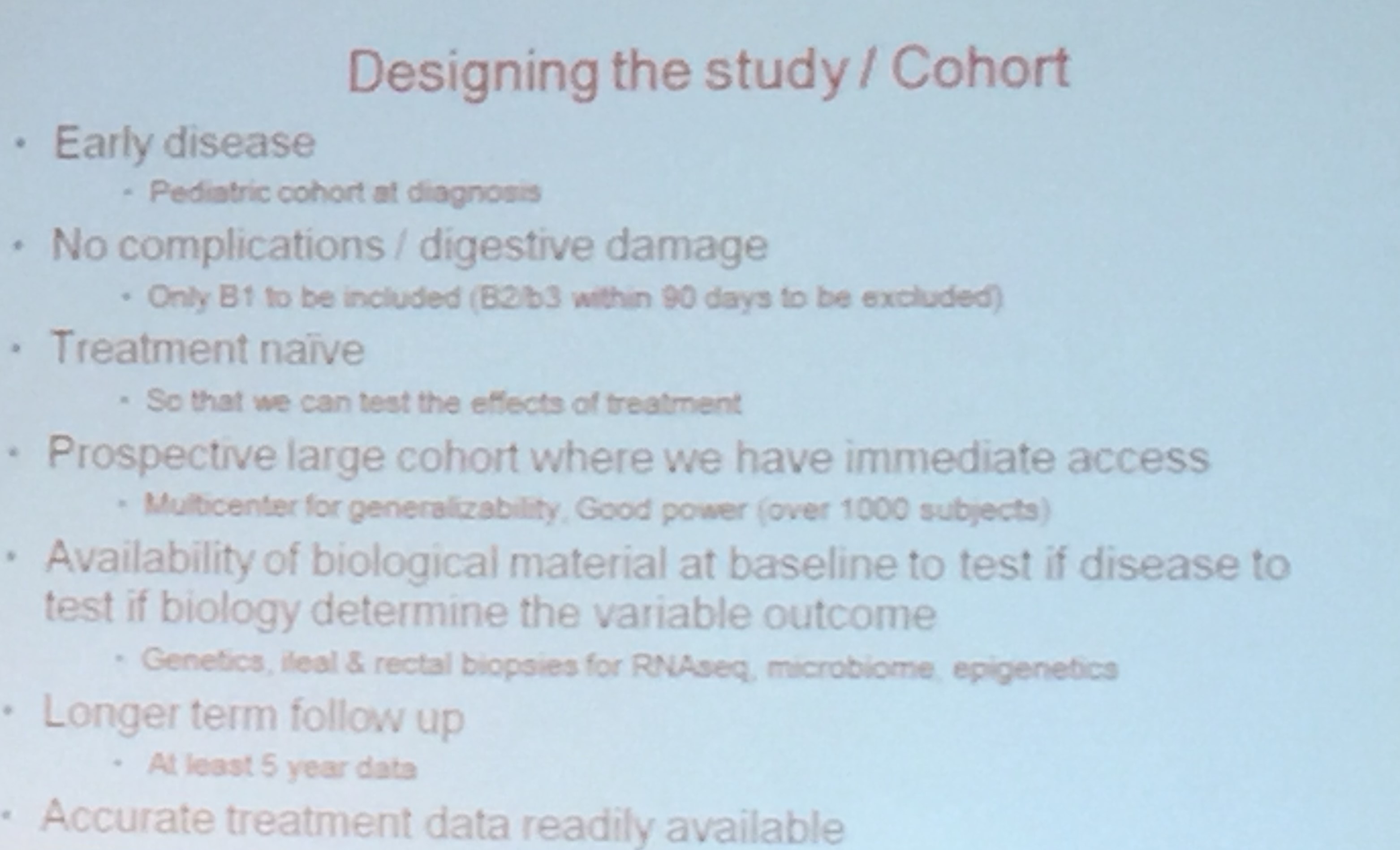
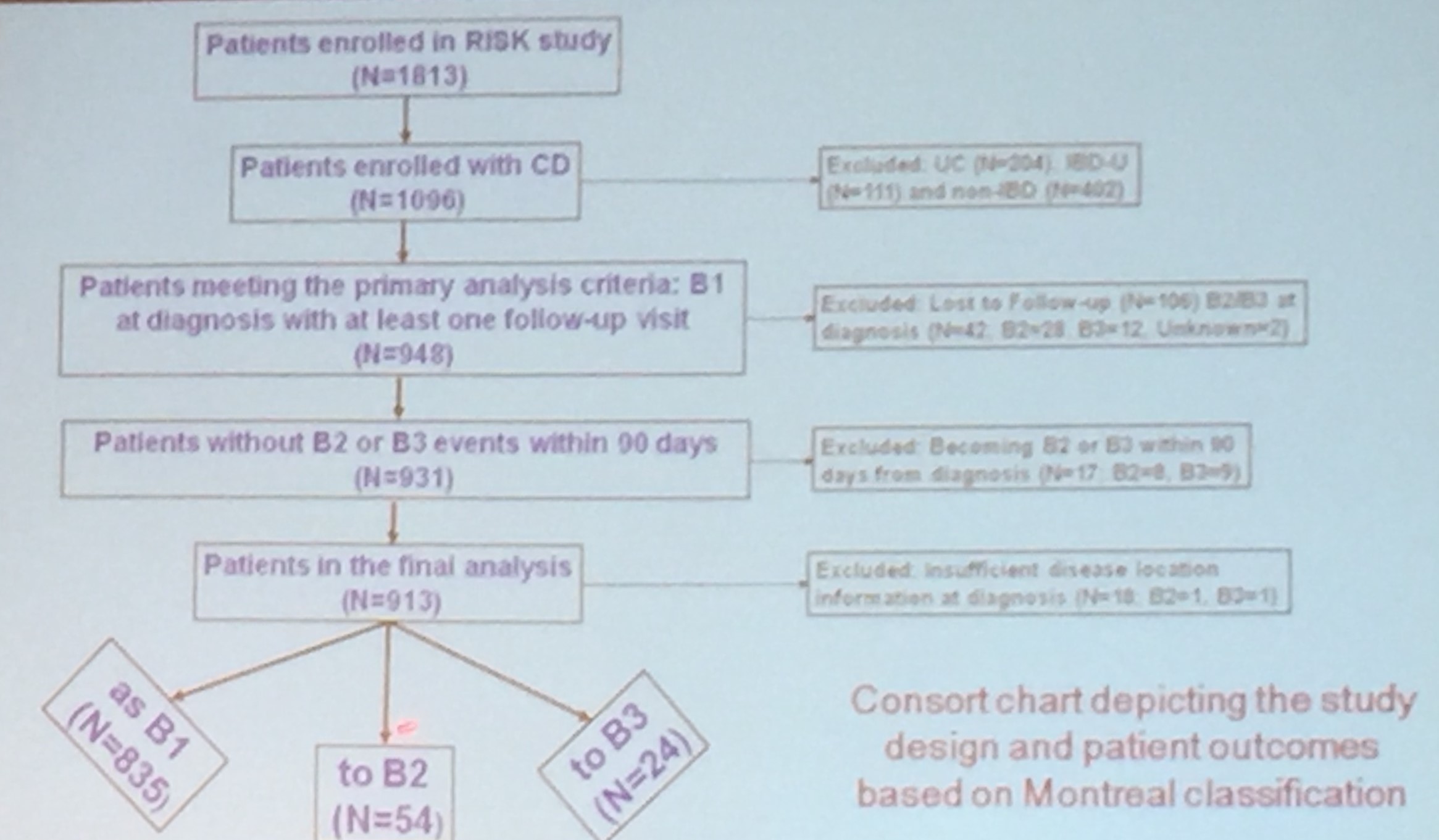
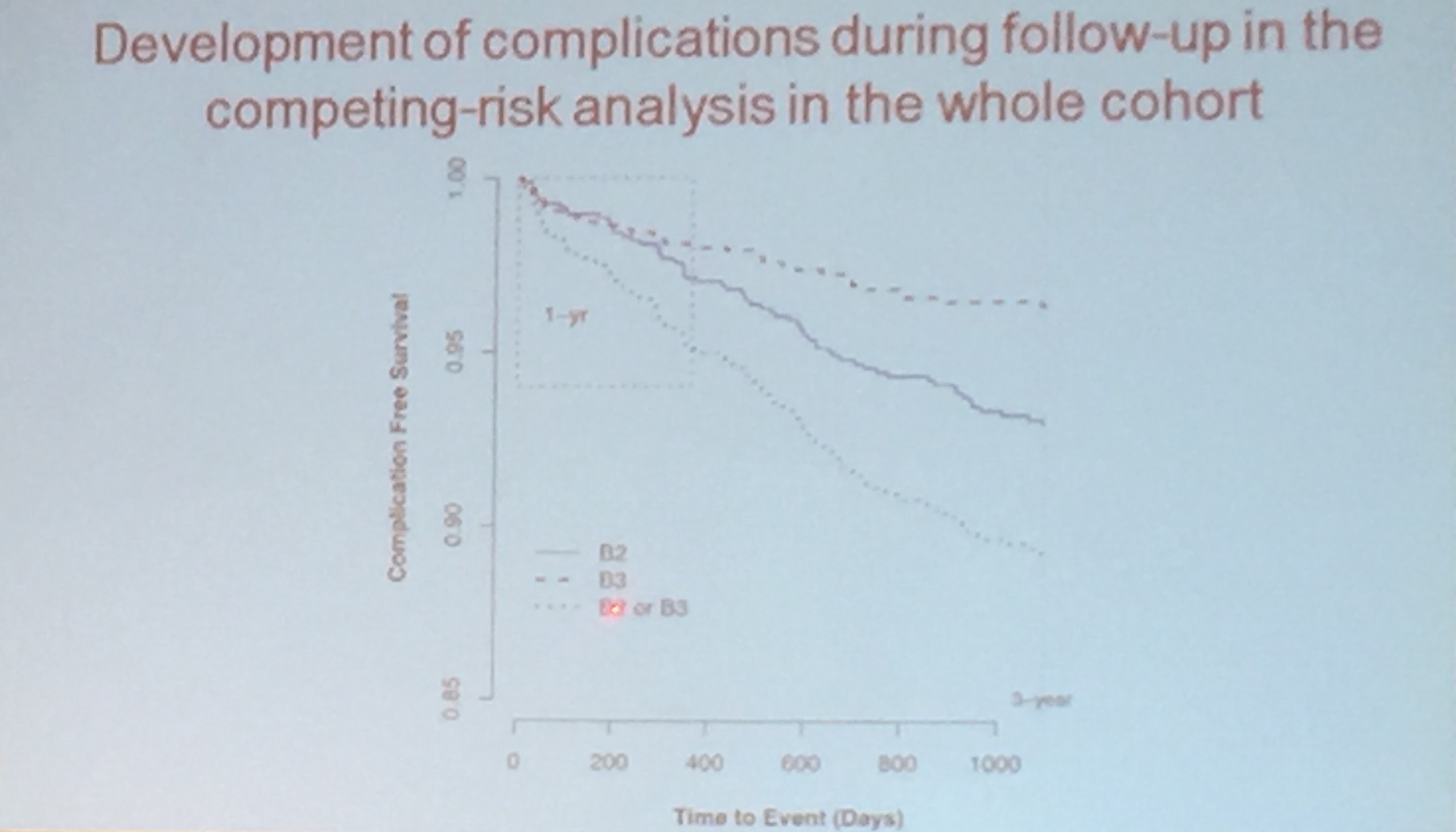
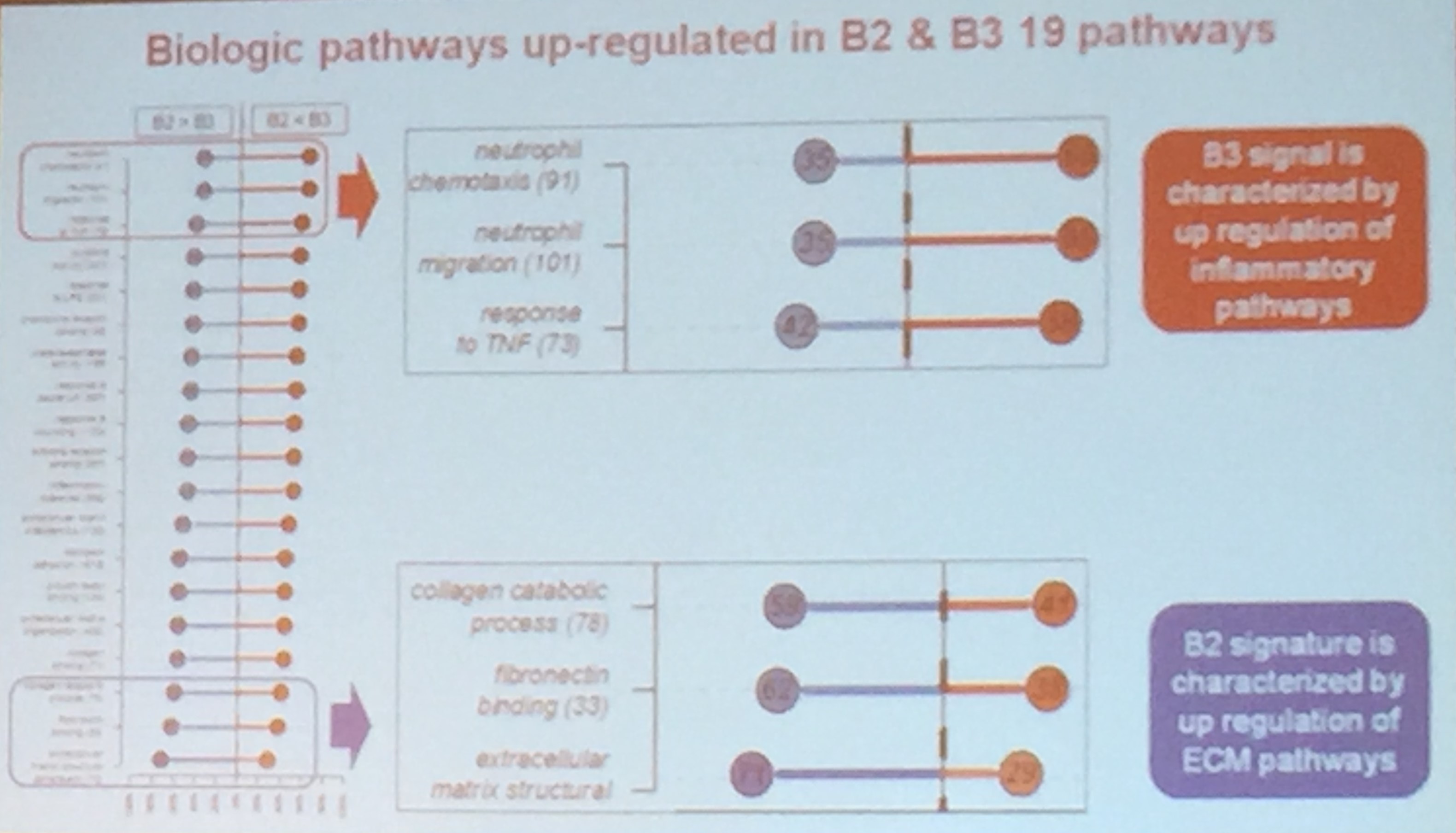
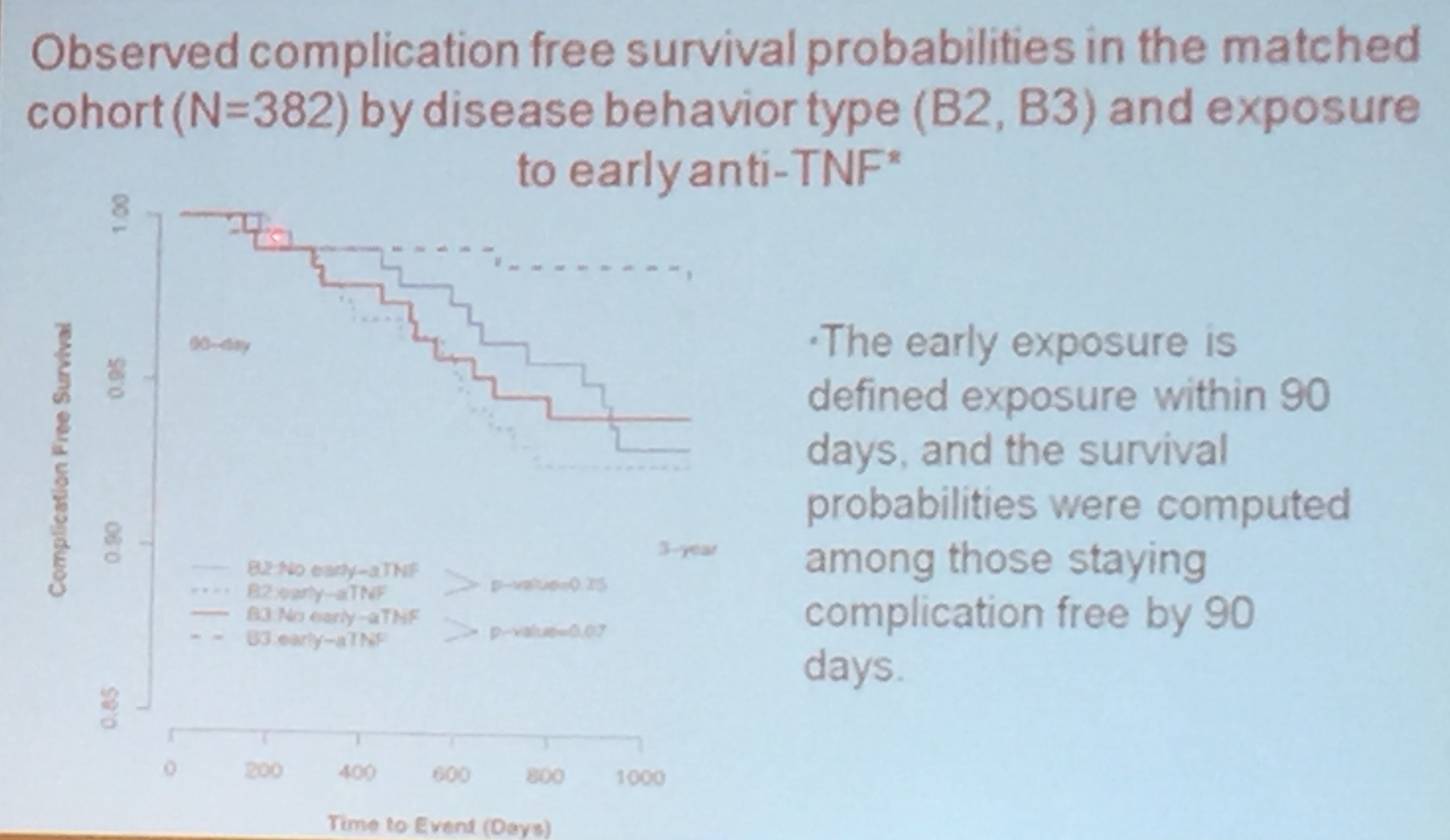
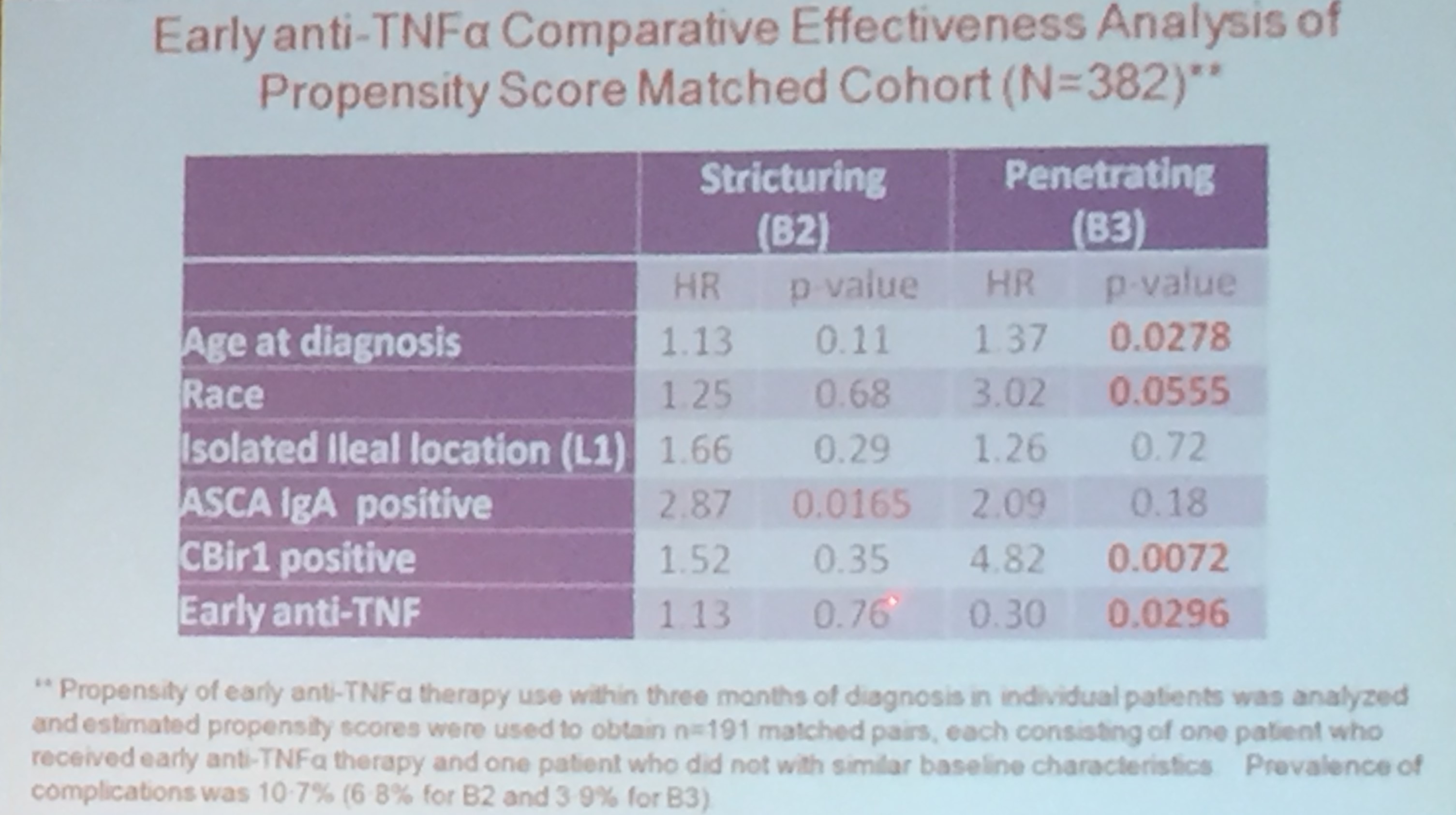
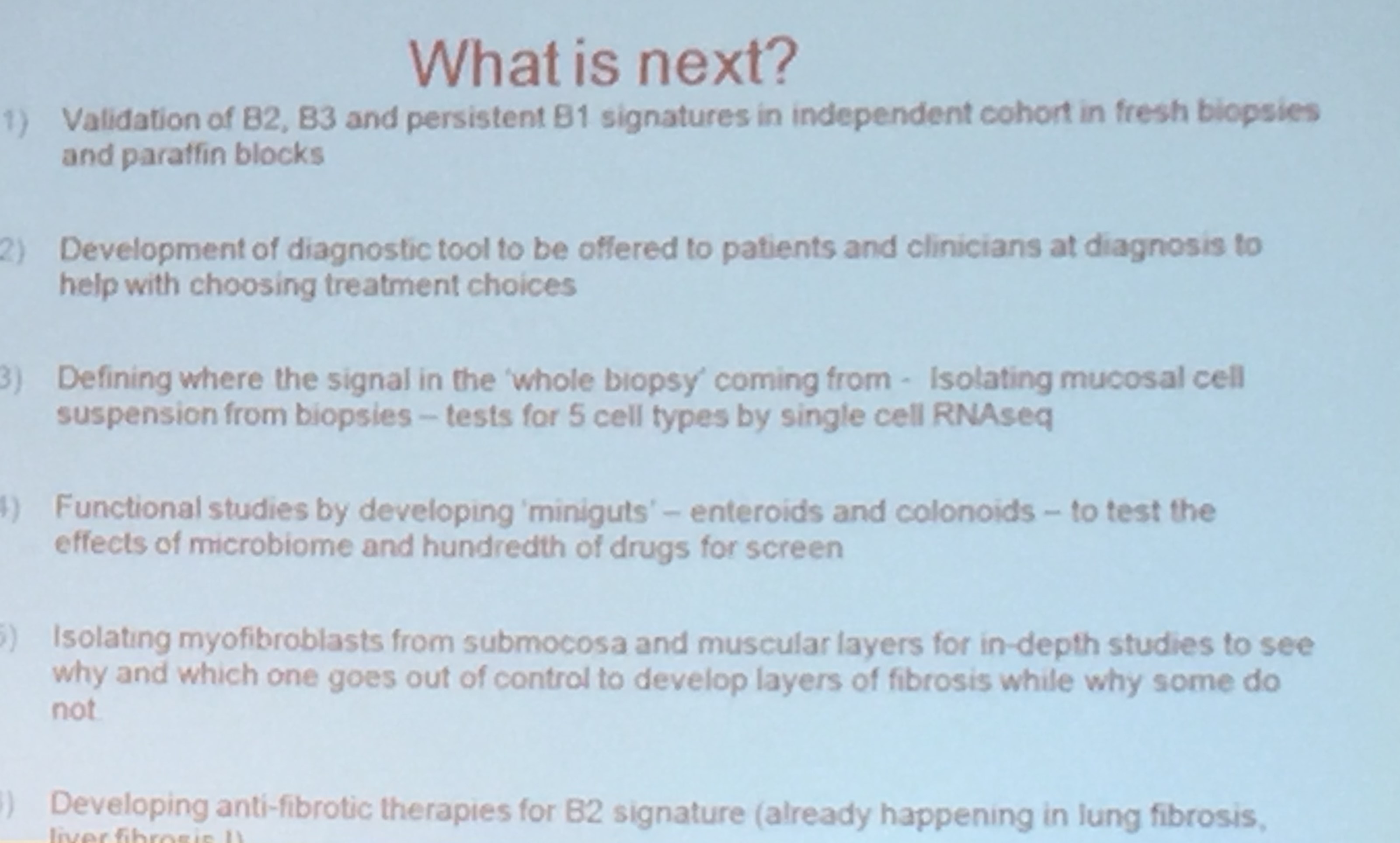
Dr. Kugasthasan’s lecture was excellent. He reviewed the typical clinical course of Crohn’s disease; in most patients, it has a remitting and relapsing course. The goal of the CCFA-sponsored RISK study was to determine how early approaches to treatment affect long-term outcomes. There is likely a window of opportunity to more favorably affect natural history of the disease. In addition, the goal is to determine whether there are predictive markers of severe disease course. This prospective study analyzed 913 patients. In this cohort, 835 remained with B1 (inflammatory) phenotype and 90 developed either B2 (stricturing) phenotype or B3 (penetrating) phenotype.
RISK Study Abstract: Prediction of complicated disease course for children newly diagnosed with Crohn’s disease: a multicentre inception cohort study (S Kugathasan et al. Lancet 2017; 389: 17108. DOI: http://dx.doi.org/10.1016/S0140-6736(17)30317-3)
Key findings:

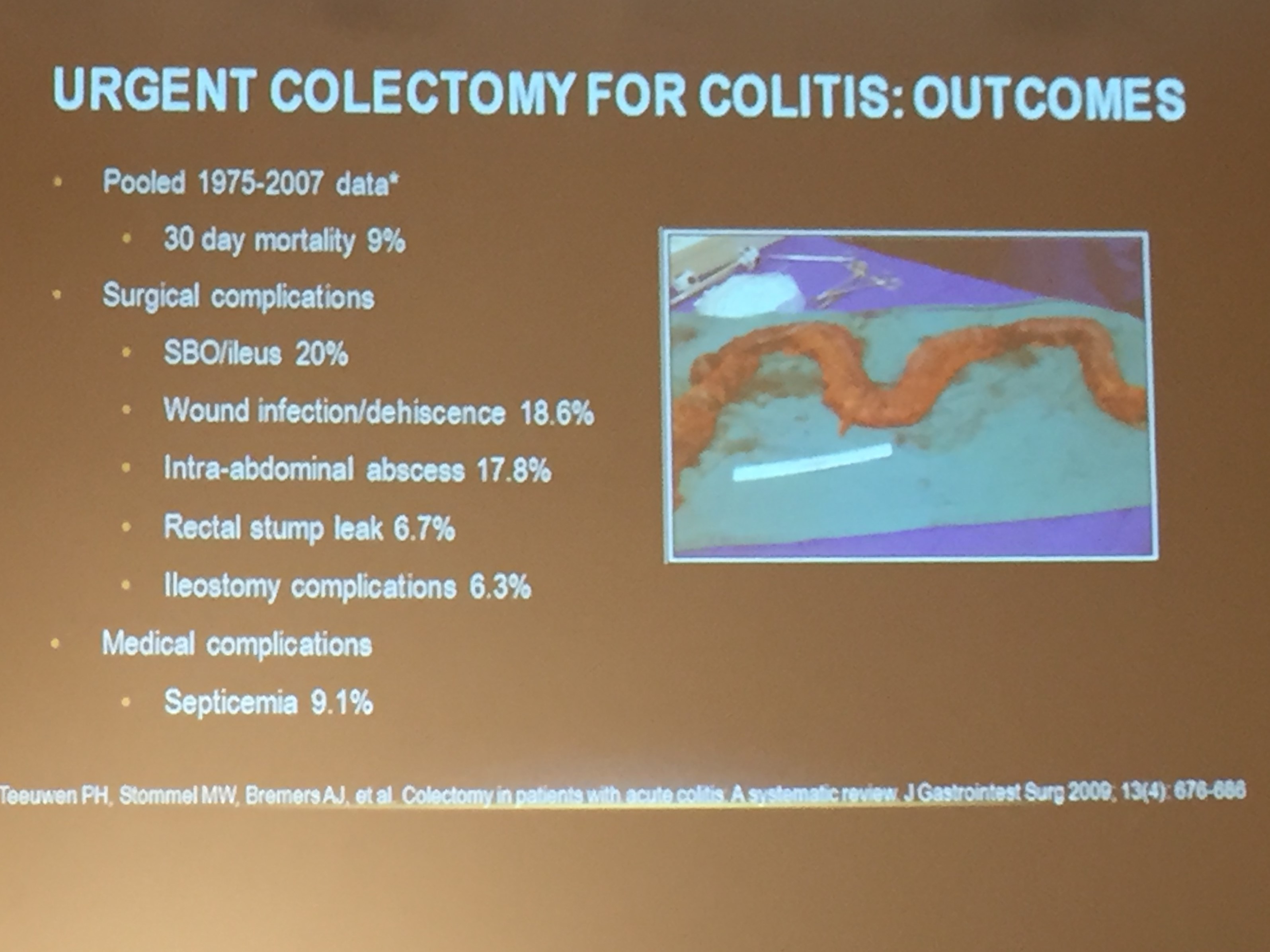
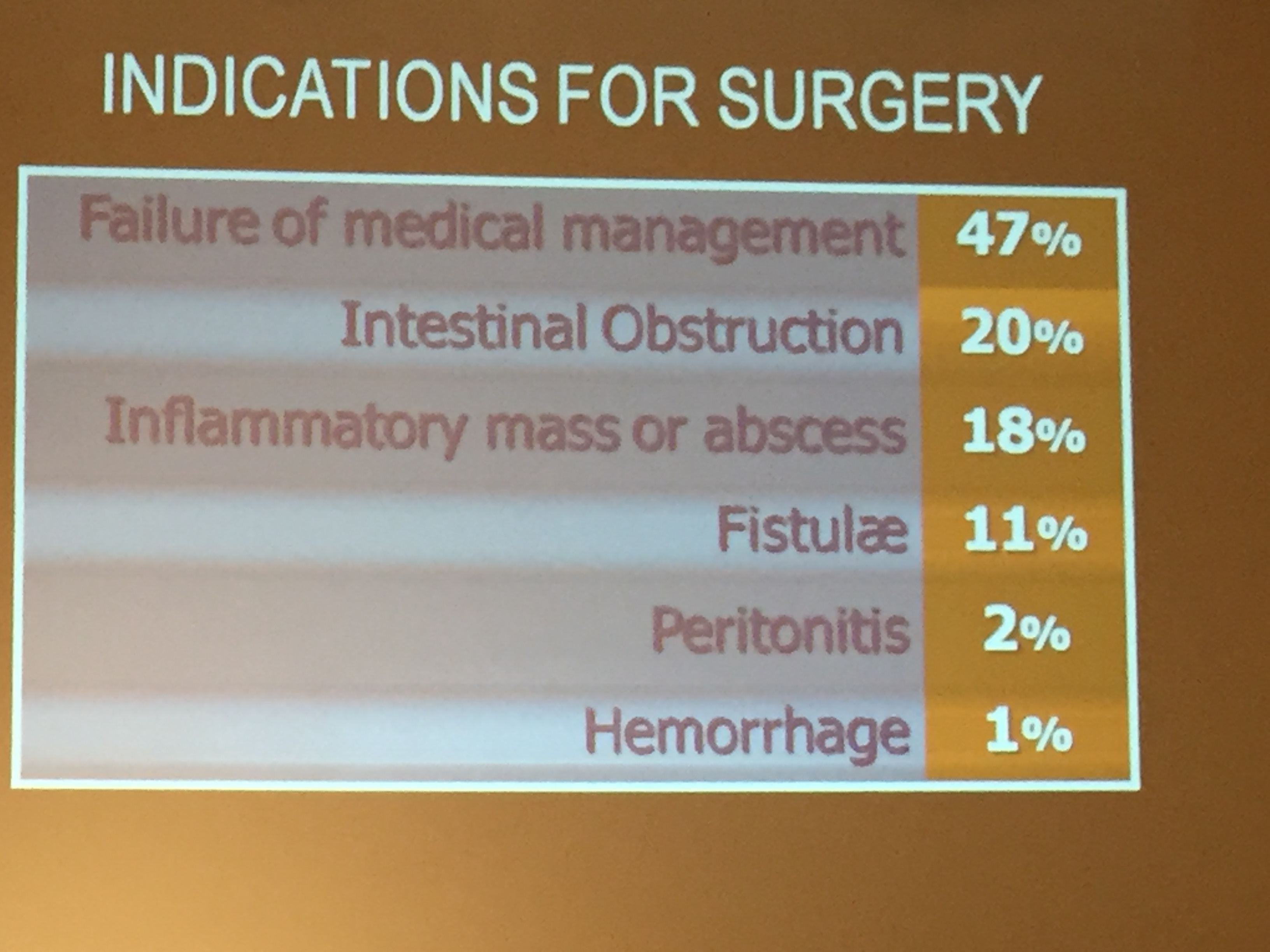
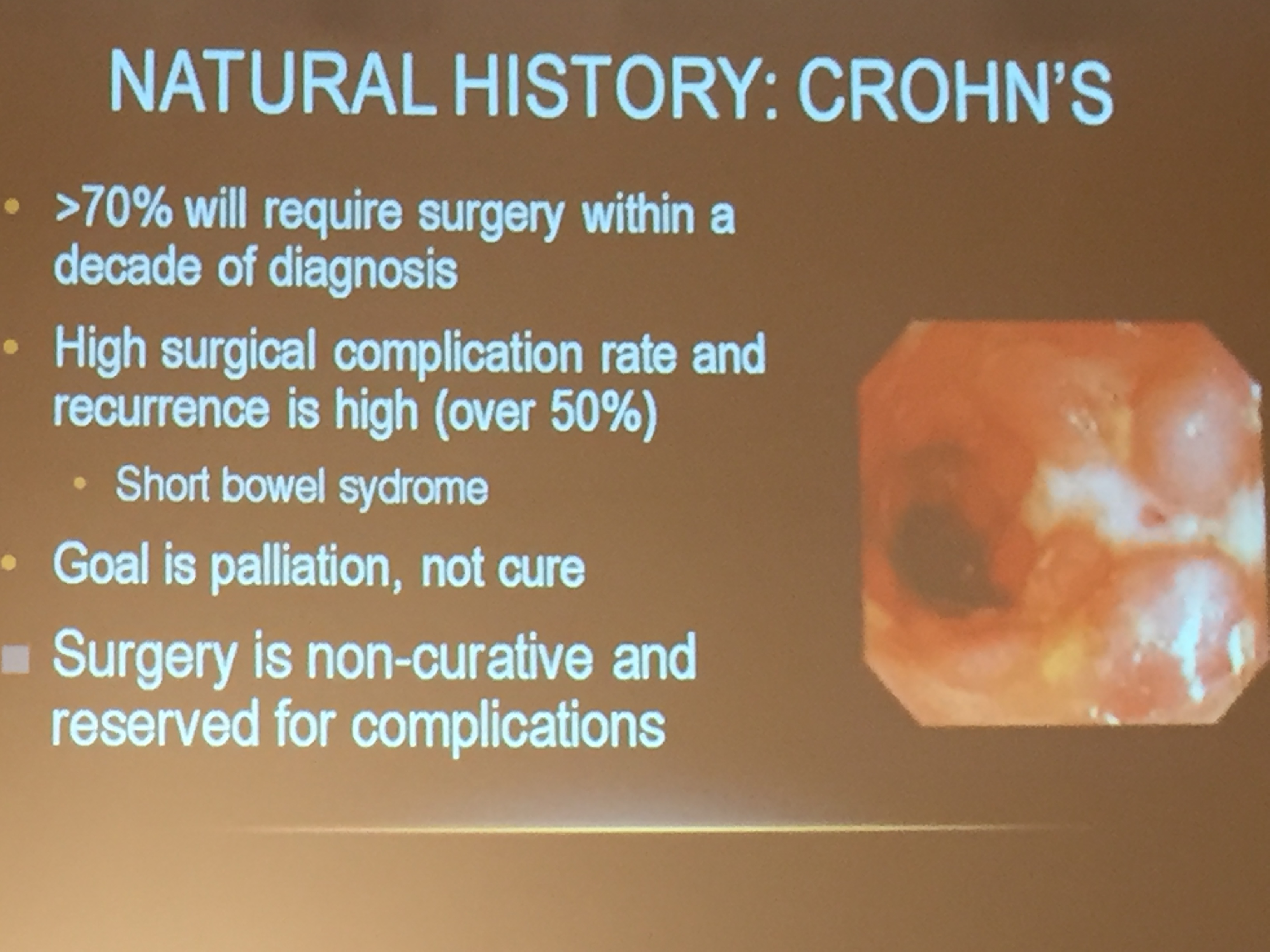
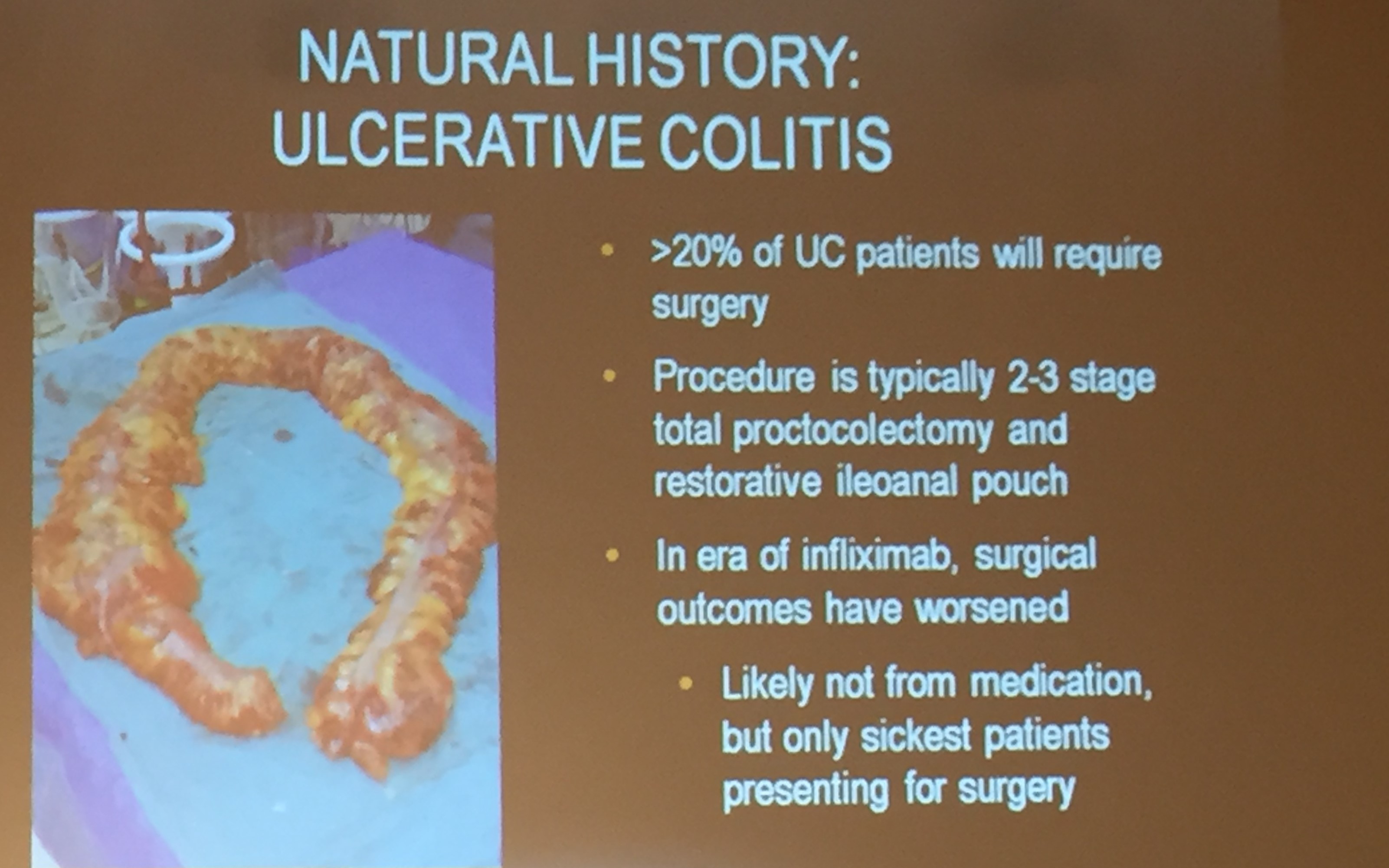
Jahnavi Srinivasan -Multi-Disciplinary Approach to IBD A Surgical Perspective
Disclaimer: These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) and changes in diet should be confirmed by prescribing physician. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
