
Related blog posts:

Related blog posts:
Barack Obama, in a perspective article (BH Obama. NEJM January 6, 2017; DOI: 10.1056/NEJMp1616577), explains the hazards of “repeal and delay.”
Here’s a link to the full text: Repealing the ACA without a Replacement — The Risks to American Health Care
Here’s an excerpt:
Put simply, all our gains are at stake if Congress takes up repealing the health law without an alternative that covers more Americans, improves quality, and makes health care more affordable. That move takes away the opportunity to build on what works and fix what does not. It adds uncertainty to lives of patients, the work of their doctors, and the hospitals and health systems that care for them. And it jeopardizes the improvements in health care that millions of Americans now enjoy.
Congress can take a responsible, bipartisan approach to improving the health care system. This was how we overhauled Medicare’s flawed physician payment system less than 2 years ago. I will applaud legislation that improves Americans’ care, but Republicans should identify improvements and explain their plan from the start — they owe the American people nothing less.
Health care reform isn’t about a nameless, faceless “system.” It’s about the millions of lives at stake — from the cancer survivor who can now take a new job without fear of losing his insurance, to the young person who can stay on her parents’ insurance after college, to the countless Americans who now live healthier lives thanks to the law’s protections. Policymakers should therefore abide by the physician’s oath: “first, do no harm.”
A related article from the LA Times indicates that Aetna misled the public with regard to its reasons for pulling out of several exchanges: Link:U.S. judge finds that Aetna misled the public about its reasons for quitting Obamacare
An excerpt:
The judge’s conclusions about Aetna’s real reasons for pulling out of Obamacare — as opposed to the rationalization the company made in public — are crucial for the debate over the fate of the Affordable Care Act. That’s because the company’s withdrawal has been exploited by Republicans to justify repealing the act. Just last week, House Speaker Paul Ryan (R-Wisc.) cited Aetna’s action on the “Charlie Rose” show, saying that it proved how shaky the exchanges were. ..
Bates found that this rationalization was largely untrue. In fact, he noted, Aetna pulled out of some states and counties that were actually profitable to make a point in its lawsuit defense — and then misled the public about its motivations.
Related blog posts:

During one of our recent group clinical meetings, one of my partners (Edith Pilzer, MD) presented an update on cystic fibrosis.
Here is a link to her slides:Link: cf-presentation
Here are a few of my notes:
There has been a great improvement in survival of cystic fibrosis patients.. From the Cystic Fibrosis Foundation:
cftr2org —website provide information on specific genotypes, including whether genotype is associated with pancreatic insufficiency
From the website:
Pancreatic enzyme replacement therapy (PERT) (see slides)
Cystic Fibrosis Related Diabetes (CFRD)
Distal Intestinal Obstruction Syndrome (DIOS)
My take: Great update. Edith has been taking care of children with cystic fibrosis for more than 30 years and has witnessed/participated in the improvement in the survival of these patients.
Related blog posts:
Disclaimer: These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.

Puerto Rico
A recent study on a new monoclonal antibody to prevent Clostridium difficile infection is available from the NEJM. Here’s the link: Preventing Clostridium difficile Infection Recurrence
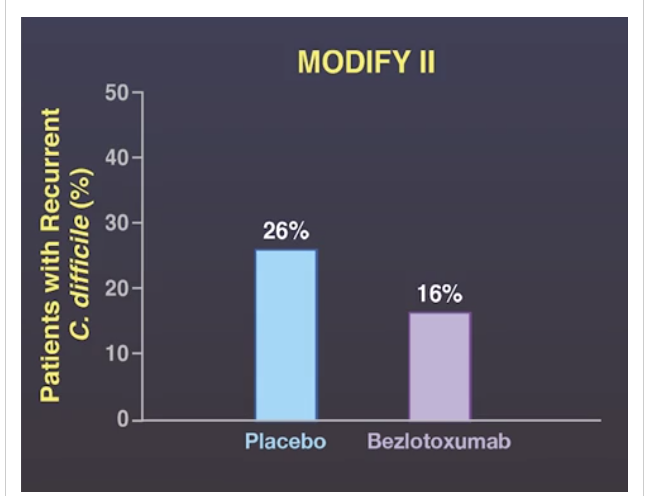

My take: In Modify I and Modify II, Bezlotoxumab reduced the rate of Clostridium difficile recurrence in elderly patients (median age 66 years). In a high risk patients, the likely hefty cost of this medication may be warranted.
These studies were likely pivotal in receiving FDA approval: FDA Approves Merck’s ZINPLAVA™ (bezlotoxumab) to Reduce Recurrence of Clostridium difficile Infection
This is a really good educational video (< 8min) -now on YouTube: Constipation in Children: Understanding and Treating This Common Problem (Thanks to John Pohl’s twitter feed for this resource)
Related blog posts:
A recent study (ALT Ma et al. J Pediatr 2016; 179: 216-8) reaches a conclusion that questions the cost-effectiveness of pretreatment TPMT activity in pediatric patients. In my opinion, this retrospective study is ridiculous. Here’s why:
The authors examined thiopurine transmethyltransferase (TPMT level) in 228 children before starting a thiopurine. They found the following:
I agree with their conclusion that routine blood tests are needed following institution of thiopurines, I think stating that “from an economic point of view –the cost for testing TPMT enzyme activity was high without major clinical benefit” cannot be made with such a small study. Deficient TPMT activity occurs in about 1 in 300. If a single patient develops bone marrow suppression due to a thiopurine medication, this can lead to a horrific and prolonged hospitalization. The cost of such a hospitalization, both economically and emotionally, is enormous.
My take: If I were taking a thiopurine, I would want to know if I metabolized this medication at a slower rate and was at increased risk for bone marrow suppression. My hunch is the authors would not forgo checking a TPMT level on themselves despite their study’s conclusion, particularly if they have ever witnessed a patient with thiopurine-induced bone marrow suppression.
Related blog posts:

Grand Prismatic Spriing, Yellowstone
U Lantto et al. J Pediatr 2016; 179: 172-7. This retrospective study showed that tonsillectomy was highly effective in children with PFAPA (periodic fever, aphthous stomatitis, pharyngitis, and adenitis) -both those with classic features and incomplete features.
“In the group that met Thomas criteria, 97% (56/58) had complete resolution of fever episodes after tonsillectomy; in the group that did not meet Thomas criteria (50/50) had complete resolution.”
Thomas criteria:

For those who missed this important pediatric study, a quick take ~2 min video link: Pediatric Migraine CHAMP Study
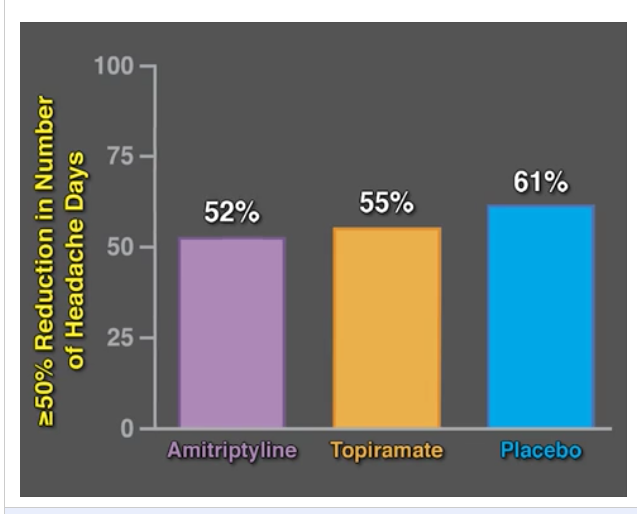
Related blog post: Topamax and Amitriptyline Did Not Work for Pediatric Migraines
My take: It looks like placebo did pretty well with >60% response rate. In a commentary on this subject, the authors noted that when patients are seen by the physician, the symptoms are often severe. So, some improvement is expected, in part, due to regression to the mean; that is, it is common to return to their baseline level of symptoms.
From A Riskin et al. Pediatrics Jan 2017 (Thanks to Seth Marcus for pointing out this study), Link: Rudeness and Medical Team Performance
Abstract
OBJECTIVES: Rudeness is routinely experienced by medical teams. We sought to explore the impact of rudeness on medical teams’ performance and test interventions that might mitigate its negative consequences.
METHODS: Thirty-nine NICU teams participated in a training workshop including simulations of acute care of term and preterm newborns. In each workshop, 2 teams were randomly assigned to either an exposure to rudeness (in which the comments of the patient’s mother included rude statements completely unrelated to the teams’ performance) or control (neutral comments) condition, and 2 additional teams were assigned to rudeness with either a preventative (cognitive bias modification [CBM]) or therapeutic (narrative) intervention. Simulation sessions were evaluated by 2 independent judges, blind to team exposure, who used structured questionnaires to assess team performance.
RESULTS: Rudeness had adverse consequences not only on diagnostic and intervention parameters (mean therapeutic score 3.81 ± 0.36 vs 4.31 ± 0.35 in controls, P < .01), but also on team processes (such as information and workload sharing, helping and communication) central to patient care (mean teamwork score 4.04 ± 0.34 vs 4.43 ± 0.37, P < .05). CBM mitigated most of these adverse effects of rudeness, but the postexposure narrative intervention had no significant effect.
CONCLUSIONS: Rudeness has robust, deleterious effects on the performance of medical teams. Moreover, exposure to rudeness debilitated the very collaborative mechanisms recognized as essential for patient care and safety. Interventions focusing on teaching medical professionals to implicitly avoid cognitive distraction such as CBM may offer a means to mitigate the adverse consequences of behaviors that, unfortunately, cannot be prevented.
This same group had a related study in 2015:The Impact of Rudeness on Medical Team Performance: A Randomized Trial
My take:The saying “you catch more flies with honey than you do with vinegar” is probably accurate.

Costa Maya, Mexico
A cautionary note on biosimilars has been discussed in a recent review (DT Rubin et al. Gastroenterol & Hepatol 2016; 12: 741-51)
In the recently completed NOR-SWITCH study presented at the United European Gastroenterology Week 2016 meeting, “a total of 481 patients were recruited across 40 centers: all patients had been on stable treatment with the originator infliximab for at least 6 months…When looking specifically at IBD patients, disease worsening was noted in 21.2% of originator infliximab-treated patients and 36.5% of CT-P13-treated Crohn’s disease patients (n=155).” The 15% difference did not reach statistical significance, but is concerning. The authors state that “subtle postranslational modifications unique to the biosimilars may be sufficient to lead to antidrug antibody formation with associated loss of response. Also, it is noted that this study did not include endoscopic evaluation.
The authors note that therapeutic monitoring worked with biosimilar product using available infliximab assays.
My take: We still have a lot to learn. The preliminary message, until more studies are available, indicate that switching stable patients could increase risk of losing response.
Related blog posts:

Puerto Rico
