From Jeff Schwimmer’s twitter feed –here’s proof that social media can save a life:
ABC News Report on Facebook to Find a Liver Transplant Donor

From Jeff Schwimmer’s twitter feed –here’s proof that social media can save a life:
ABC News Report on Facebook to Find a Liver Transplant Donor
This blog entry has abbreviated/summarized this presentation. Though not intentional, some important material is likely to have been omitted; in addition, transcription errors are possible as well.
One of the topics debated at this year’s meeting was the issue of whether it is worthwhile for patients with esophageal varices to undergo primary prophylaxis.
Here’s a summary:
Esophageal Banding: Proactive vs Expectant Waiting Maureen Jonas (Boston Children’s) and Karen Murray (Seattle Children’s)
Reviewed definitions of portal hypertension. Hepatic venous portal gradient (HVPG) >12 associated with variceal bleeding is the standard in adult medicine.
Management issues: primary prophylaxis, treatment of acute bleeding, and secondary prophylaxis.
Adult Data/Guidelines:
Pediatrics and Beta-Blockers:
Non-Selective Beta-blockers.
Risks of primary prophylaxis with banding or sclerotherapy:
Rebuttal:
Take-home message: insufficient data to demonstrate efficacy of primary prophylaxis as well as to demonstrate adverse effects of primary prophylaxis.
Related blog posts:
“The best preparation for tomorrow is to do today’s work superbly well” –William Osler (quote cited in NEJM 2014; 371: 1565-66).
This blog entry has abbreviated/summarized the presentations. Though not intentional, some important material is likely to have been omitted; in addition, transcription errors are possible as well.
For me, these lectures were a useful review and represent an effort to achieve Osler’s objective of doing superb work. If I had to choose a single issue that may affect my practice: when initiating infliximab, consider checking week 14 trough levels of infliximab and optimize dosing.
The role of the microbiome in IBD –Subra Kugathasan (Emory)
This was a terrific lecture though with some overlap with a number of other presentations at the meeting. The lecture reviewed how to interpret microbiome studies and what we are learning from these studies with regard to inflammatory bowel disease.
Enteral Nutrition and Microbiota –conclusion:
The Role of Drug Monitoring in Inflammatory Bowel Disease –Jennifer Strople (Children’s Hospital of Chicago)
TPMT Testing/thiopurine metabolite monitoring
Monitoring for anti-TNF Therapy
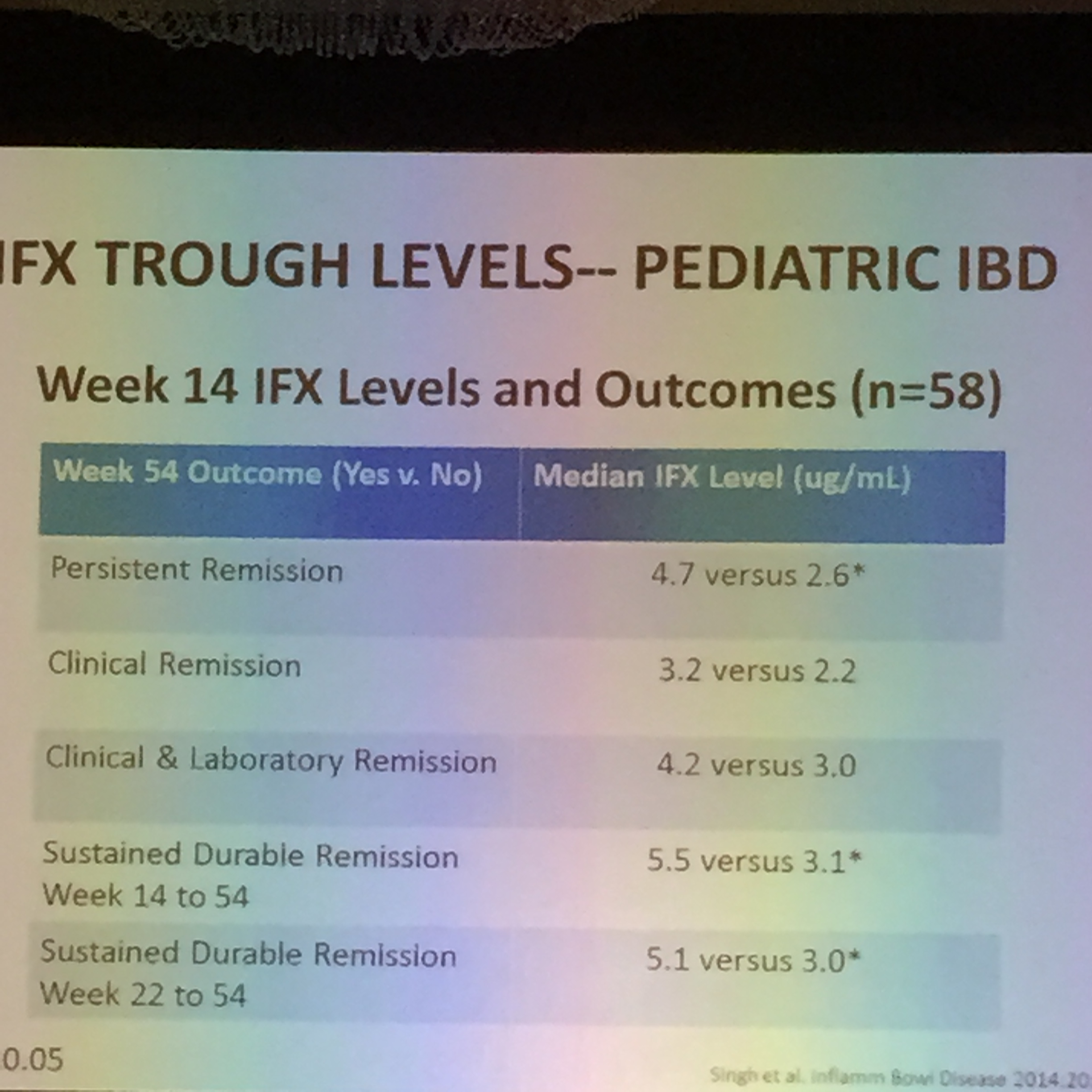
IFX Levels at 14 weeks
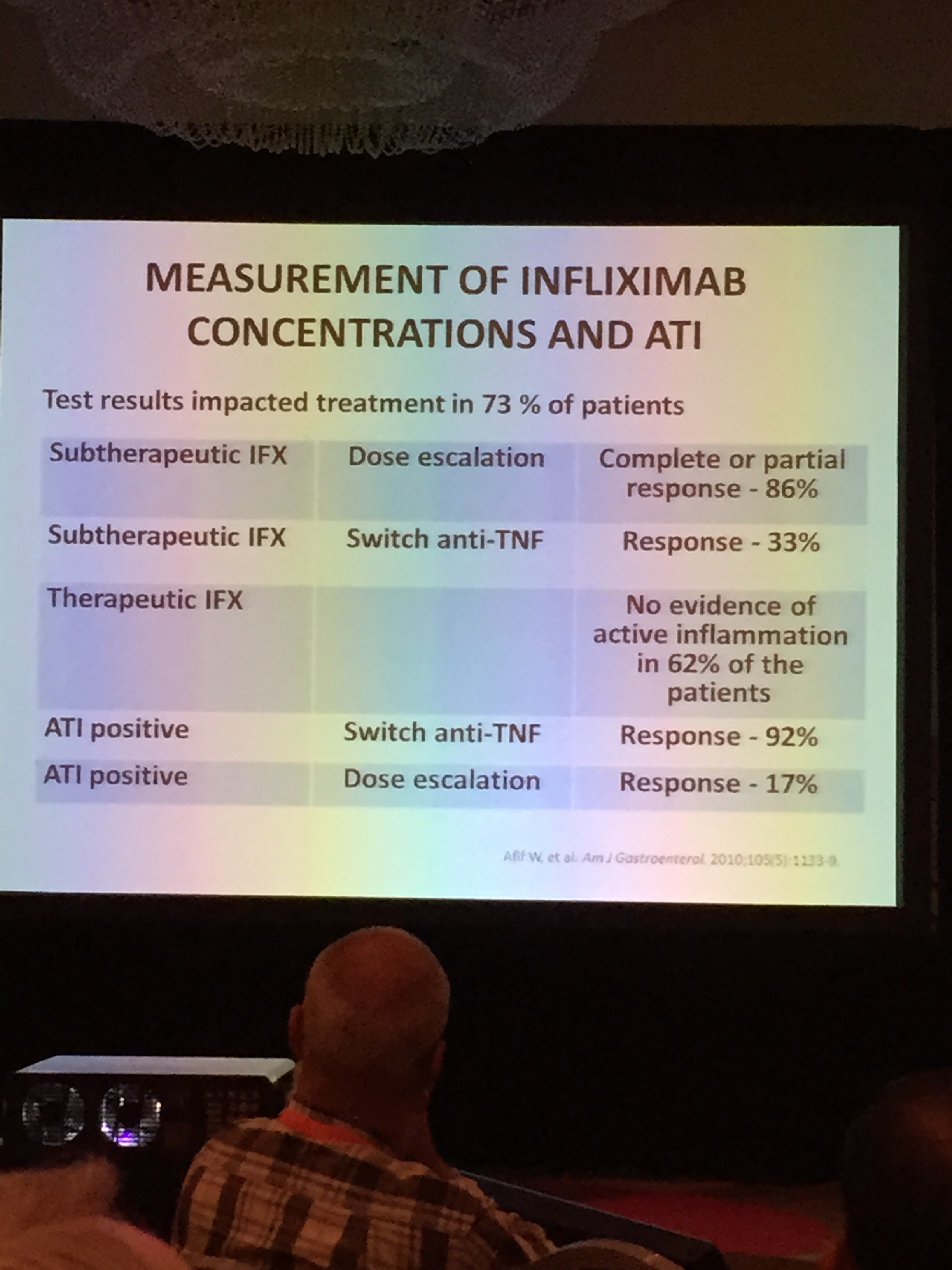
IFX Algorithm
Related posts on this topic:
Debate: Immunomodulators versus Biologic agents
In the face of the “Biologic Tsunami,” Dr. Markowitz suggested –“Don’t throw the baby out with the bathwater”
Biologics –important to start before disease phenotype changed to stricturing/penetrating disease. (See images below)
Related posts:
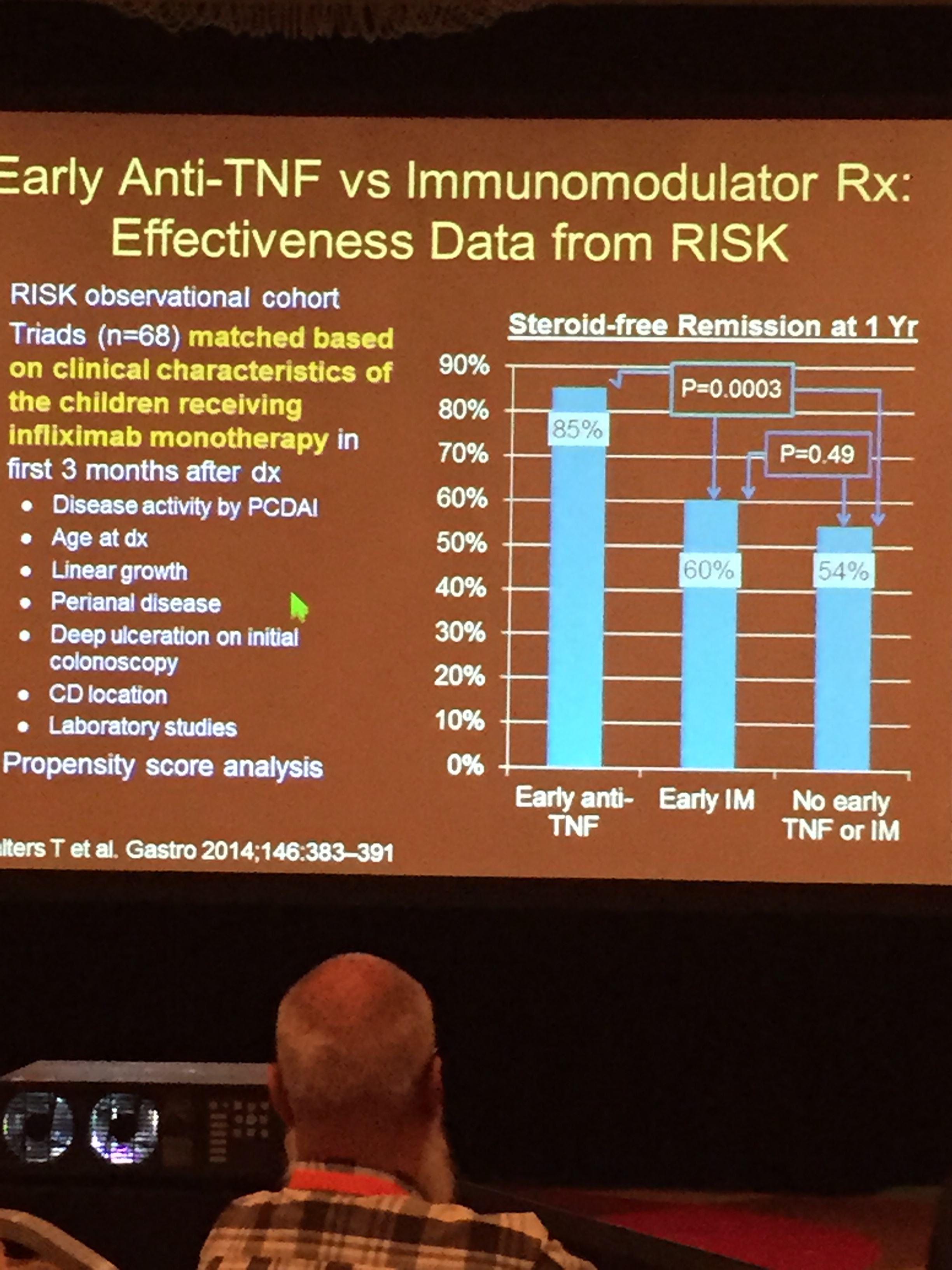
Early anti-TNF -RISK Cohort
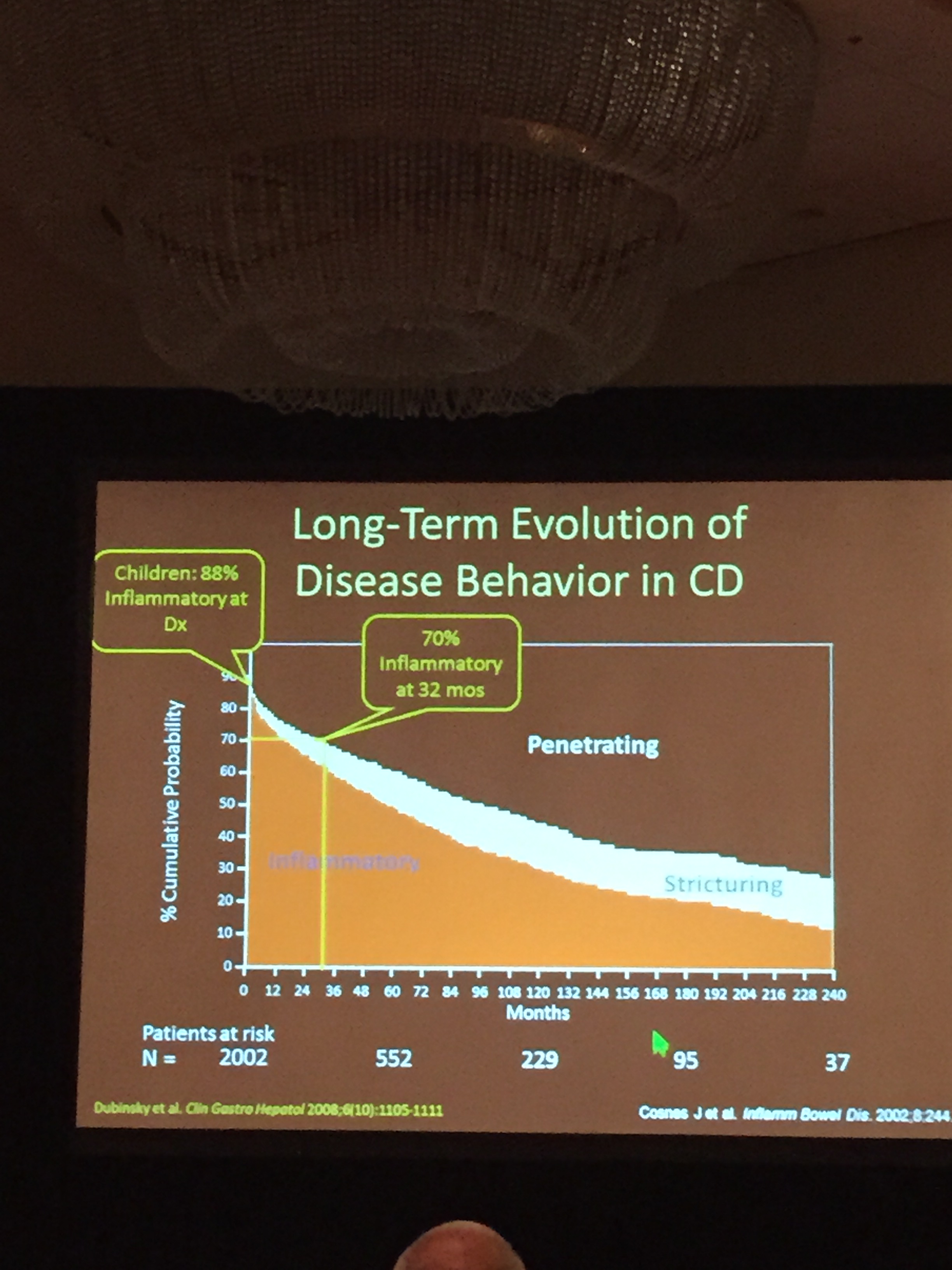
Long Term Risk of Stricturing (Cosnes et al)
At this year’s NASPGHAN meeting, the keynote lecture was given by Brennan Spiegel. (Brennan Spiegel, MD (@BrennanSpiegel) | Twitter) This was a great talk!
This blog entry has abbreviated/summarized the presentation. Though not intentional, some important material is likely to have been omitted; in addition, transcription errors are possible as well.
Challenges in healthcare:
We spend all our time within walls of our clinic/hospital, but patients spend 99% time outside
How do we tailor care to the individual and make it more cost-effective? How do we get there? Potential/Emerging Tools:
Key question for patients: What is the most important goal for you/your family today?
How to improve communication with family? Electronic medical records often designed for billing rather than educating
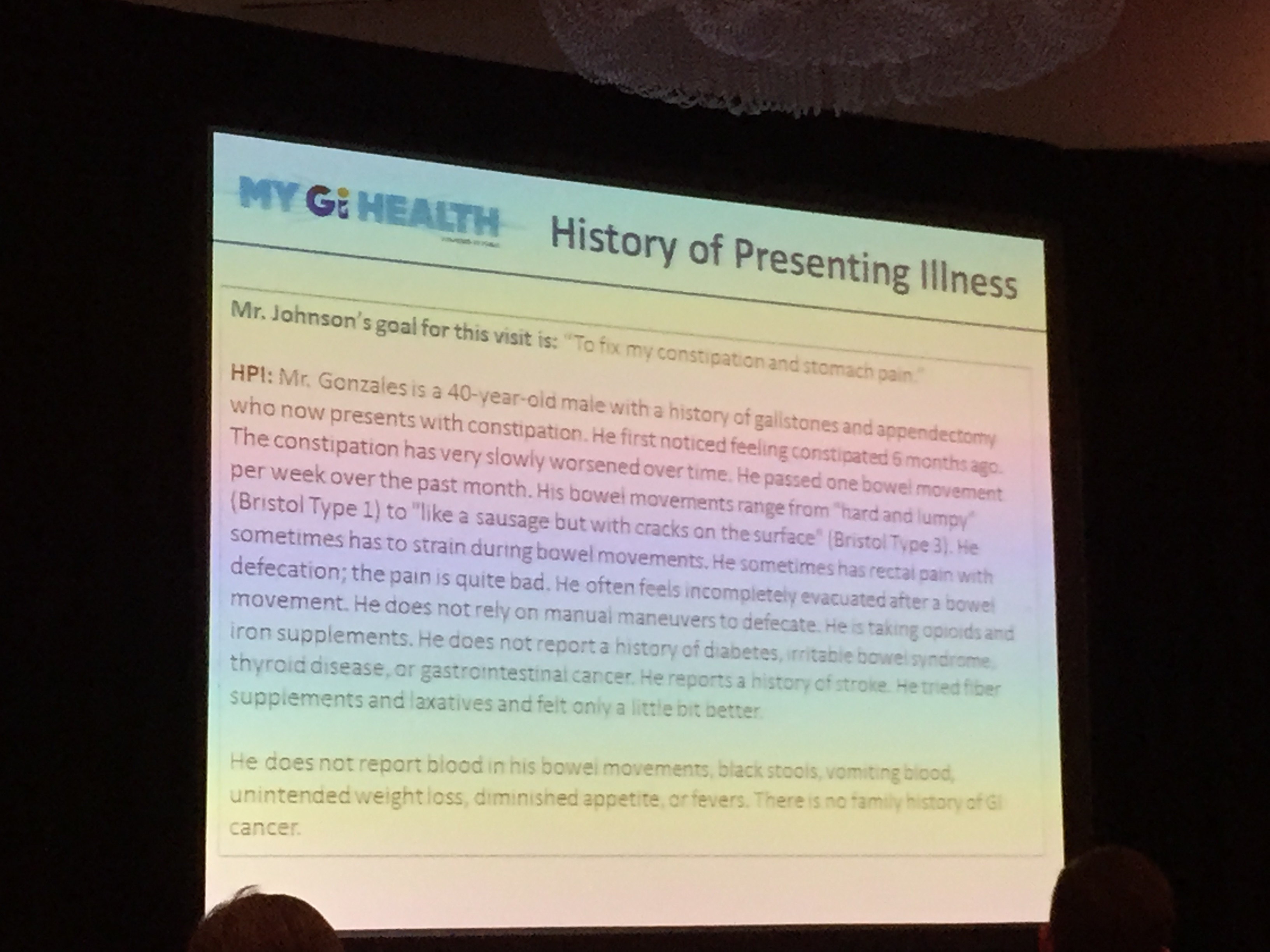
MyGiHealth website/soon-to-be-app. Here’s a link to YouTube video introduction.
History by computer outperformed physicians
Obtaining information outside the confines of the office can help overcome Hawthorne effect. (Related blog post: Checklists -Helpful? Overhyped? Hawthorne Effect …). Passive vs Active monitoring.
Twitter: “What you say on twitter may be seen by everyone all over the word instantly”
Mayo clinic is studying the impact of social media.
Example of patients initiating research. “Spontaneous Coronary Artery Dissection: A Disease-Specific Social Networking Community-Initiated Study” Lead author: Marysia Tweet
Biosensors:
75,000 health apps available at this time.
Recommended Reading by Dr. Spiegel: The Creative Destruction of Medicine by Eric Topol. The Creative Destruction of Medicine: How the Digital …
A recent publication in JPGN indicates that resuming low dose soy-based parenteral lipid can be effective in patients (n=7) whose cholestasis had resolved on a fish oil-based parenteral lipid. It does not resolve the larger question of whether fish oil-based parenteral lipids are truly more effective than soy-based parenteral lipids (see previous blog links below).
Here’s the abstract:
Objectives: Intestinal failure associated liver disease (IFALD) contributes to significant morbidity in pediatric intestinal failure (IF) patients. However, the use of parenteral nutrition (PN) with a fish oil-based IV emulsion (FO) has been associated with biochemical reversal of cholestasis and improved outcomes. Unfortunately, FO increases the complexity of care: as it can only be administered under FDA compassionate use protocols requiring special monitoring, is not available as a 3-in-1 solution and is more expensive than comparable soy-based lipid formulation (SO). Due to these pragmatic constraints a series of patient families were switched to low-dose (1 g/kg/day) SO following biochemical resolution of cholestasis. This study examines if reversal of cholestasis and somatic growth are maintained following this transition.
Methods: Chart review of all children with IFALD who switched from FO to SO following resolution of cholestasis. Variables are presented as medians (interquartile ranges). Comparisons performed using Wilcoxon signed-rank test.
Results: 7 patients aged 25.9 (16.2,43.2) months were transitioned to SO following reversal of cholestasis using FO. At a median follow up 13.9 (4.3,50.1) months there were no significant differences between pre- and post-transition serum alanine and aspartate aminotransferases, direct bilirubin, and weight-for-age z-scores. Due to recurrence of cholestasis, one patient was restarted on FO after four months on SO.
Conclusions: Biochemical reversal of IFALD and growth were preserved after transition from FO to SO in 6/7 (86%) patients. Given the challenges associated with the use of FO, SO may be a viable alternative in select home PN patients.
Related blog posts:
Cool picture:
Link (from NEJM twitter feed) to contrast study showing tracheoesophageal fistula: NEJM Image of TEF in newborn. Video available at website.
This blog entry has abbreviated/summarized the presentations. Though not intentional, some important material is likely to have been omitted; in addition, transcription errors are possible as well.
Link: PG Course Syllabus – FINAL (entire syllabus)
The speakers reviewed a lot of IBD material (both at the postgraduate course and at the meeting); much of it has been has been covered in previous blog posts:
Early Onset Inflammatory Bowel Disease –Scott Snapper (Boston Children’s Hospital) pg 170 in Syllabus
Infantile IBD (age <2 years)
Surgery in Crohn’s Disease –Jason Frischer (Cincinnati Children’s)
Perioperative care
Surgical problems (JPGN 2013; 57: 394 NASPGHAN Guidelines): Abscess, Fistula, Stricture
Crohn’s and UC ‐ What to do when anti‐TNF isn’t working? –Athos Bousvaros (Boston Children’s) pg 190 in Syllabus
Off-label IBD drugs in children for medically-refractory disease.
Potential Rescue treatments
Before off-label drugs:
Data for tacrolimus from Boston. n=46. (Watson et al, IBD Journal 2011). Used most frequently with severe UC.
Data for thalidomide –31 of 49 achieved remission. Lazzerini et al, JAMA. 2013;310(20):2164‐2173. Side effects -birth defects, neuropathy. STEPS program.
Data for vedolizumab. Feagan et al NEJM 2013; 369:699. Remission (in the responders) for ulcerative colitis at 52 weeks:
For Crohns’ disease , Vedolizumab also works in Crohn’s disease, but it takes time (Sands et al: Gastroenterology 2014 147:618‐627)
Off-label does not equate to experimental! pg 199:
FDA Statement: The FD&C Act does not, however, limit the manner in which a physician may use an approved drug. Once a product has been approved for marketing, a physician may prescribe it for uses or in treatment regimens or patient populations that are not included in approved labeling. Such “unapproved” or, more precisely, “unlabeled” uses may be appropriate and rational in certain circumstances, and may, in fact, reflect approaches to drug therapy that have been extensively reported in medical literature.
“Luminitis:” When Inflammation is Not IBD (Microscopic Colitides) –Robbyn Sockolow (Weill Cornell Medical School) pg 180 in Syllabus
Microscopic Colitis -pediatric prevalence unknown (JPGN 2013;57:557-561). Nonbloody diarrhea with normal-appearance grossly.
Eosinophilic colitis
This recent study (summarized in earlier post today/Dr. Barnard’s talk) provides more information on the microbiome in patients with pediatric Crohn’s. Here’s a link to full article: Specific transcriptome and microbiome signature in pediatric Crohn’s Here’s the abstract:
From Cincinnati Children’s Pediatric Insights (summary of findings):
“The discovery of specific bacterial populations and a core gene signature associated with Crohn’s disease could lead to new diagnostic testing and improved treatment for inflammatory bowel disease (IBD), according to a study led by researchers at Cincinnati Children’s.
‘This study identifies a set of bacteria that are associated with symptoms, and a group of anti-inflammatory genes that are associated with intestinal damage in children with Crohn’s disease,’ says Lee (Ted) Denson, MD, Medical Director of the Inflammatory Bowel Disease Center, senior investigator for the study, published online July 8 in the Journal of Clinical Investigation. Yael Haberman Ziv, MD, was the study’s first author.
Denson’s team studied tissue samples from the ileum, the lowermost portion of the small intestine, in a large number of children with Crohn’s disease. They found specific types of bacteria and a “core” gene expression signature, both of which appear to affect inflammatory changes in the gut. Certain genes in the core signature appeared to be specifically associated with intestinal damage from deep ulcers.”
John Barnard –Basic Science Year in Review
“Emerging Trends and Provocative Findings in Basic Science”
This blog entry has abbreviated/summarized this terrific presentation. Though not intentional, some important material is likely to have been omitted; in addition, transcription errors are possible as well. To minimize these issues, I have placed a link to most of Dr. Barnard’s slides which he shared:
“Big Data” –big increase in “big data” cited in pubmed over past year.
Scientific fraud –more attention to this issue this past year. Two papers in Nature were retracted. One researcher committed suicide and one arrested. Scientific fraud undermines important messages & ruins credibility of other important advances.
CRISPR-Cas9: Gene editing. CRISPRs –“RNA guides” Cas9: “molecular scissors” (endonucleases)
“Genome editing has never been easier.” Examples:
Liver regeneration in zebrafish. Implication: Liver cells will be regenerated in humans. Gastroenterol 2014; 146: 789.
Microbiome Big Data:
Microbiome –affects the entire body:
Recommended Reading by Dr. Barnard: “Missing Microbes” How the overuse of antibiotics is fueling our modern plagues. Martin Blaser
This blog entry has abbreviated/summarized the presentations. Though not intentional, some important material is likely to have been omitted; in addition, transcription errors are possible as well. Link to full syllabus:
The Dreaded Wake-Up Call (Part A) –Maercedes Martinez (NY Presbyterian Hospital) (pg 55 syllabus)
Variceal Bleeding – “When RED is not attractive”
Discussed presentation of varices (gastric/esophageal), etiologies, association with portal hypertension. Reviewed variceal grading.
Medical management:
The Dreaded Wake-Up Call (Part B) –Lee Bass (Children’s Hospital of Chicago) (pg 67 in syllabus)
Nonvariceal GI Bleeding Management
Endoscopic Interventions for Biliary Tract Disease — Victor Fox (pg 75 in Syllabus)
Choledocholithiasis is most common need for interventional biliary endoscopy and increasing related to increase risk with increase in obesity.(Buxbaum J. Gastrointest Clin N Am 2013;23:251‐75)
Requires advanced training to achieve high level of skill and experience
Other points:
“Most strictures and leaks can be successfully managed endoscopically without need for surgical intervention”
Take-home message: Endoscopic biliary interventions are increasingly employed in children with similar safety and technical success as adult patients
Related blog posts:
Disclaimer: These blog posts are for educational purposes only. Specific dosing of medications/diets (along with potential adverse effects) should be confirmed by prescribing physician/nutritionist. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
