G Ding et al. N Engl J Med 2024;391: e34. DOI: 10.1056/NEJMicm2406623. Trichuriasis
Case report: A 2-year-old boy from a rural village in China was brought to the pediatric clinic with a 6-month history of diarrhea and poor weight gain. Laboratory studies showed iron-deficiency anemia, eosinophilia, and occult blood in the stool.
The worms, which were 3 to 4 cm in length, were identified as Trichuris trichiura — also known as human whipworm infection…Trichuriasis results from the ingestion of soil contaminated by whipworm eggs. Adult worms mature in the large intestine and affix themselves there by threading into the mucosa. Trichuriasis is usually asymptomatic but may result in diarrhea and growth retardation in cases of heavy infection, especially in young children. The child’s diarrhea resolved after treatment with albendazole.
CDC Link: Trichuriasis “The adult worms (approximately 4 cm in length) live in the cecum and ascending colon… The females begin to oviposit 60 to 70 days after infection. Female worms in the cecum shed between 3,000 and 20,000 eggs per day. The life span of the adults is about 1 year.”
One of the first warnings came in a paper published in 2021. There was an unexpected rise in pancreatic cancer among young people in the United States from 2000 to 2018… a new study published on Monday in The Annals of Internal Medicine suggests, the whole alarm could be misguided.
The authors of the paper, led by Dr. Vishal R. Patel, a surgical resident at Brigham and Women’s Hospital in Boston, did not dispute the data showing a rising incidence. They report that from 2001 to 2019 the number of young people — ages 15 to 39 — diagnosed with pancreatic cancer soared. The rate of pancreatic surgeries more than doubled in women and men…
With more pancreatic cancers in young people, there should be more pancreatic cancer deaths. And there were not. Nor were more young people getting diagnosed with later-stage cancers. Instead, the increase was confined to cancers that were in very early stages.
Many cancers will never cause harm if left alone, but with increasingly sensitive tools, doctors are finding more and more of them. Because there usually is no way to know if they are dangerous, doctors tend to treat them aggressively…It’s the hallmark of what researchers call overdiagnosis: a rise in incidence without a linked rise in deaths..
The sudden rise in pancreatic cancer incidence is largely being driven by another type of tumor — endocrine cancers [rather than the more dangerous adenocarcinomas]. They tend to be indolent, taking years or even decades to grow and spread, but occasionally they can turn malignant…
“A lot of patients say, ‘Get it out,’” said Dr. Adewole S. Adamson, an author of the new paper and an overdiagnosis expert at the University of Texas at Austin. “When someone tells you that you have cancer you feel like you have to do something.”
But, said Dr. William Jarnagin, a pancreatic cancer specialist at Memorial Sloan Kettering Cancer Center, removing early stage endocrine tumors “has never been proven to be a good strategy.”
My take: More cases of pancreatic tumors are being detected with the increased use of cross-sectional imaging (eg. CT scan, MRI). It is helpful to know that the increase in (mainly) pancreatic endocrine tumors is not leading to more deaths. Yet, each individual case presents some difficult decisions.
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
From the Museum of Illusions (Atlantic Station, Atlanta):
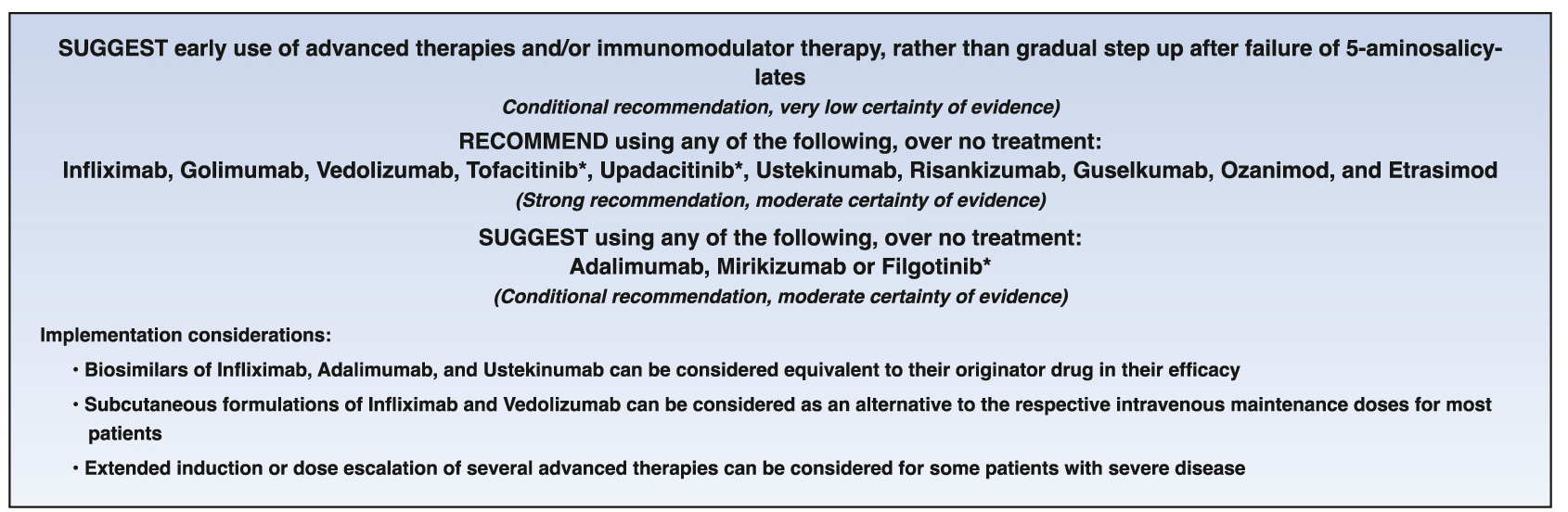
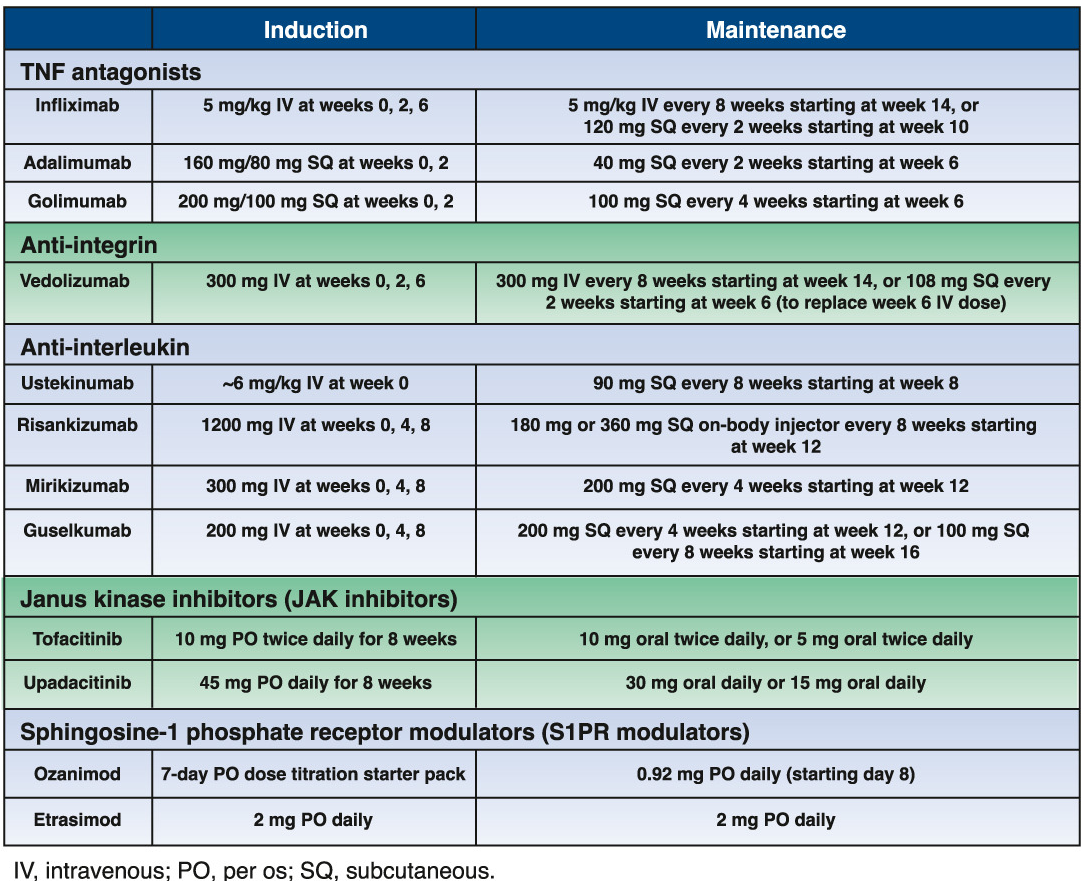
This is a recent clinical guideline intended to serve as the starting point of a “living guideline” for adults with moderate-to severe ulcerative colitis.
The good news is that the AGA plans to update these guidelines semi-annually. The bad news is that this guideline does not provide the best advice.
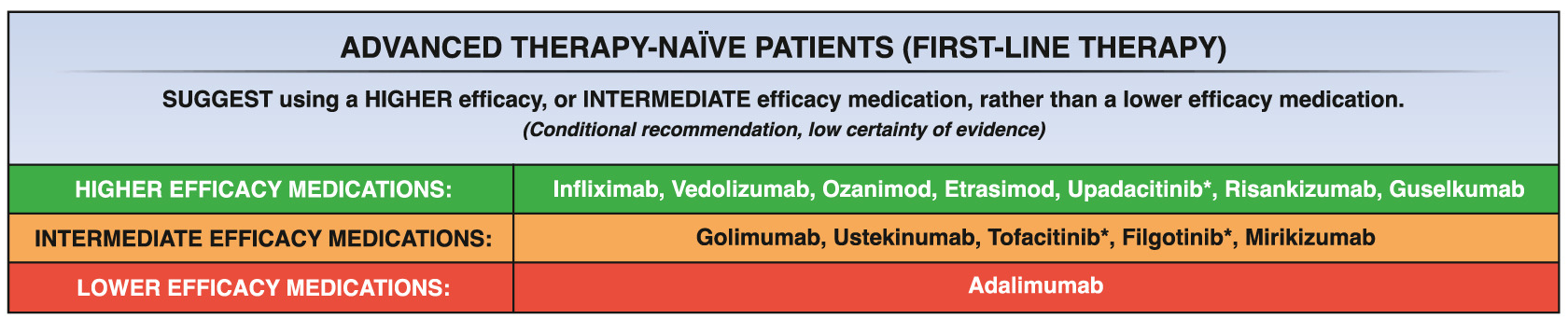
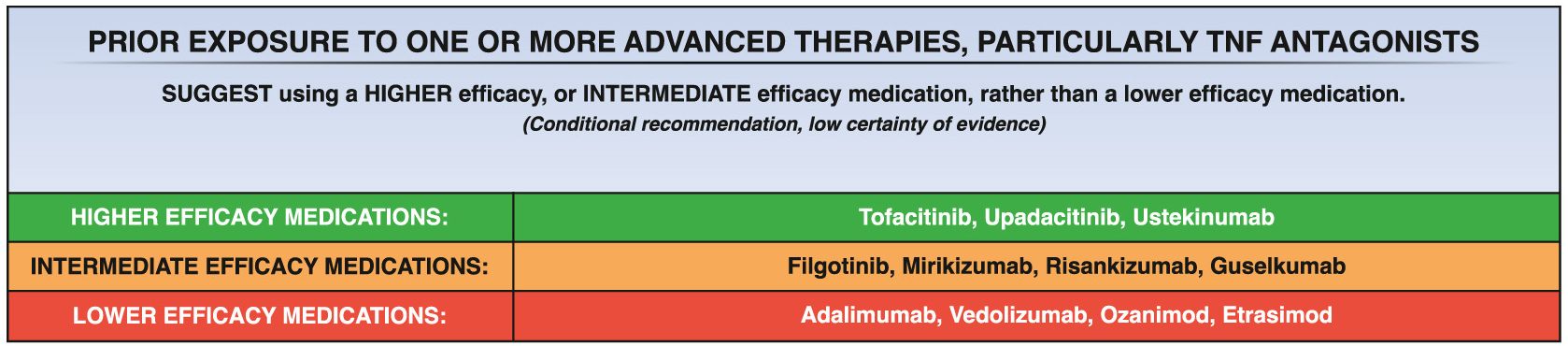
It lumps recommended treatments into broad categories rather than indicating which therapies have the most effectiveness.
It is useful that the guidelines specifically recommend against step up therapy.
FDA labelling recommends upadacitinib only in patients who have not responded to anti-TNF therapy
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
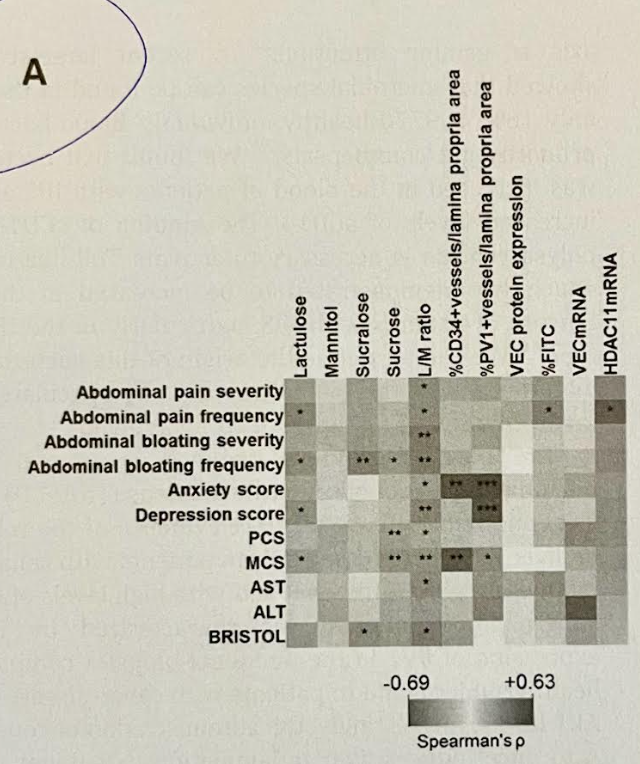
This study examined markers of the epithelial and vascular barriers in 223 patients with irritable bowel syndrome in comparison to 78 healthy subjects. In actuality, this lengthy report was a composite of about 8 different experiments.
Key findings:
Figure 2 summarizes in vivo and in vitro epithelial permeability testing using orally-administered sugars and using Caco-2 cell incubation of control/IBS supernatants. In all of these experiments, there was a significant mean increase in IBS-D permeability compared to controls.
Figures 3 and 4 report on significant changes the gut vascular barrier and specific mediators, respectively, in IBS compared to controls
One novel finding was correlation of epithelial barrier markers with gastrointestinal symptoms and gut vascular dysfunction with systemic systems including anxiety and depression (see heat map below)
Relationships between epithelial and endothelial permeability markers and symptoms. The asterisks on the heatmap indicate significances in the Spearman’s correlation.
My take: The term ‘leaky gut’ has a negative connotation among many gastroenterologists as it has been associated with misleading diagnostic and therapeutic claims. However, this study shows a correlation between epithelial and vascular barrier disruptions and symptoms in irritable bowel. This is useful information; nevertheless, there are not simple tests to identify these findings and there are not therapeutics with demonstrated efficacy.
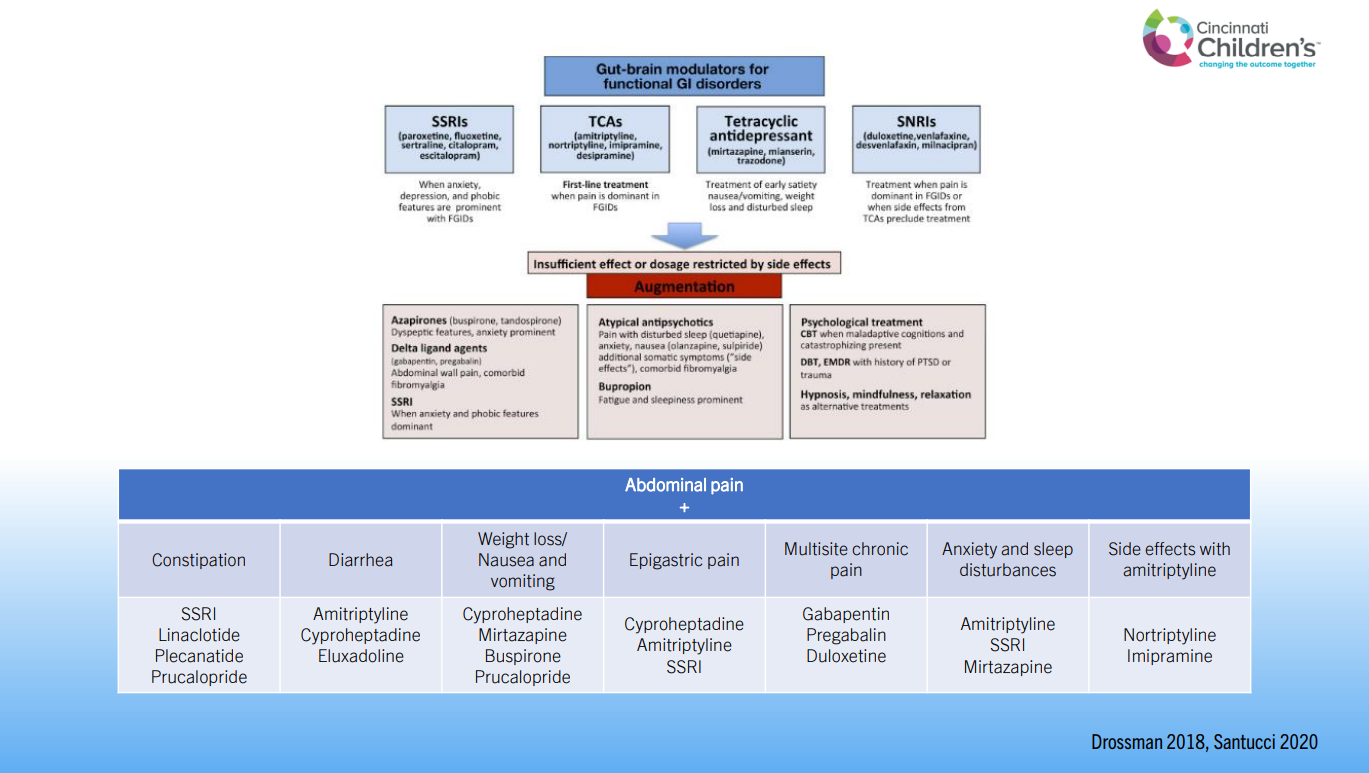
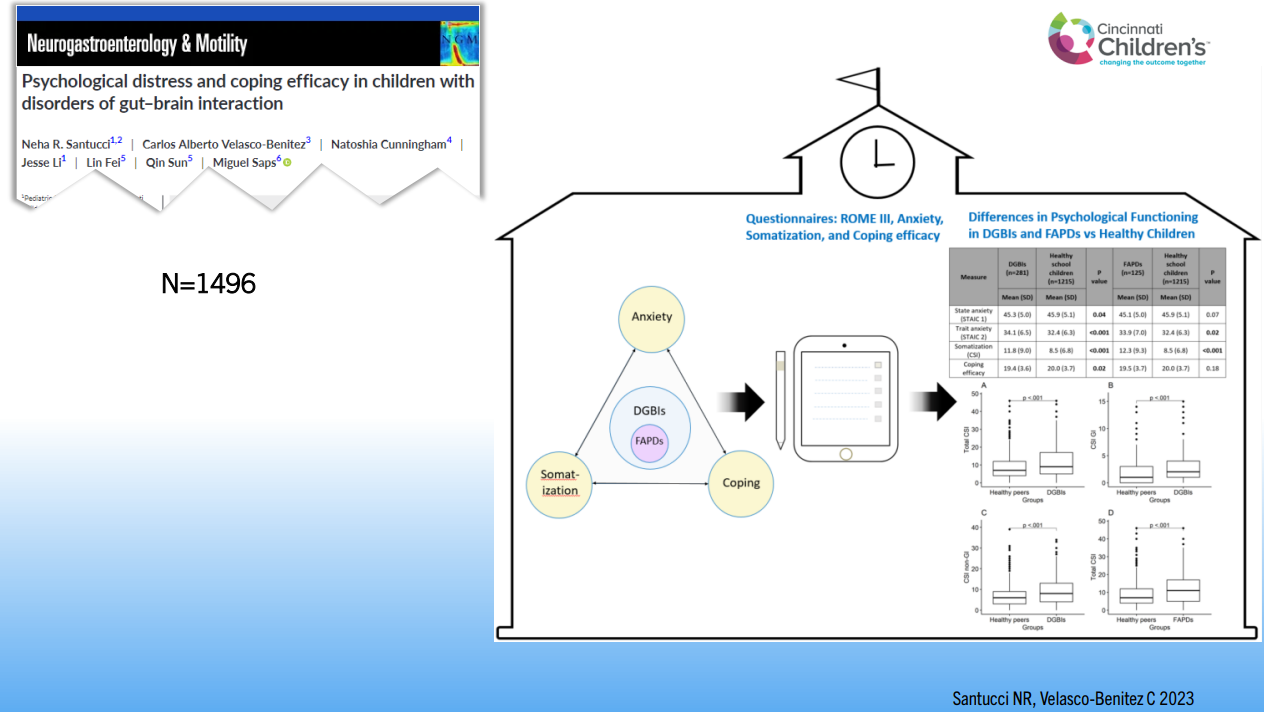
Recently, Dr. Neha Santucci gave our group an excellent update on disorders of gut-brain interaction. My notes below may contain errors in transcription and in omission. Along with my notes, I have included many of her slides.
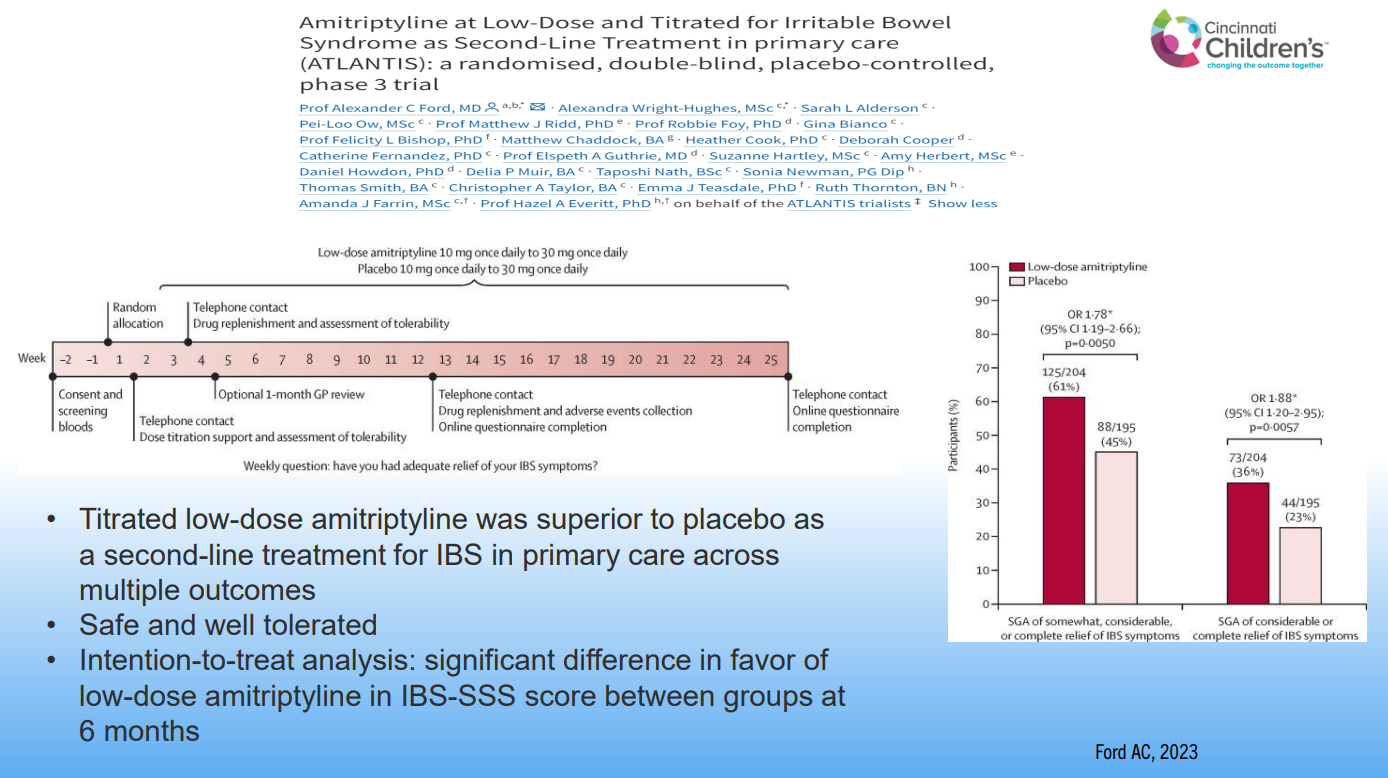
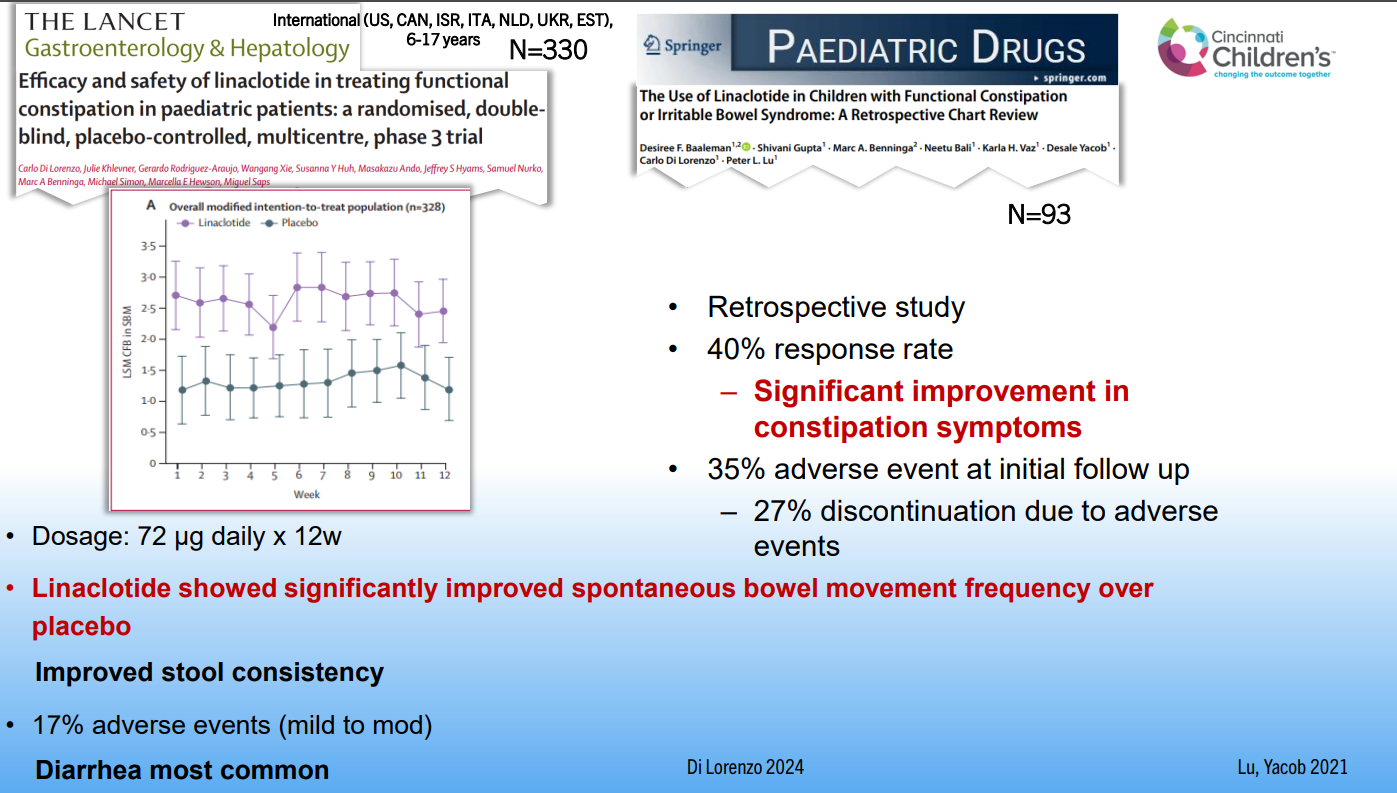
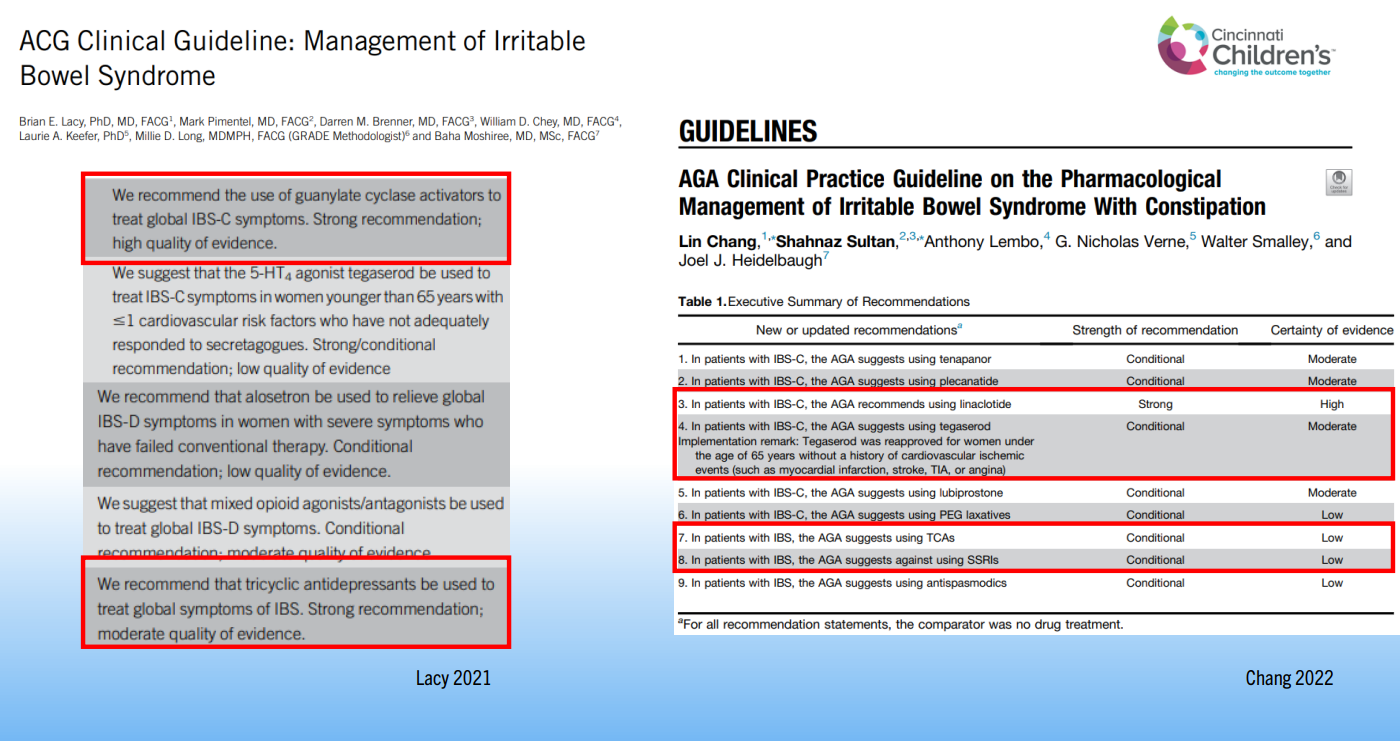
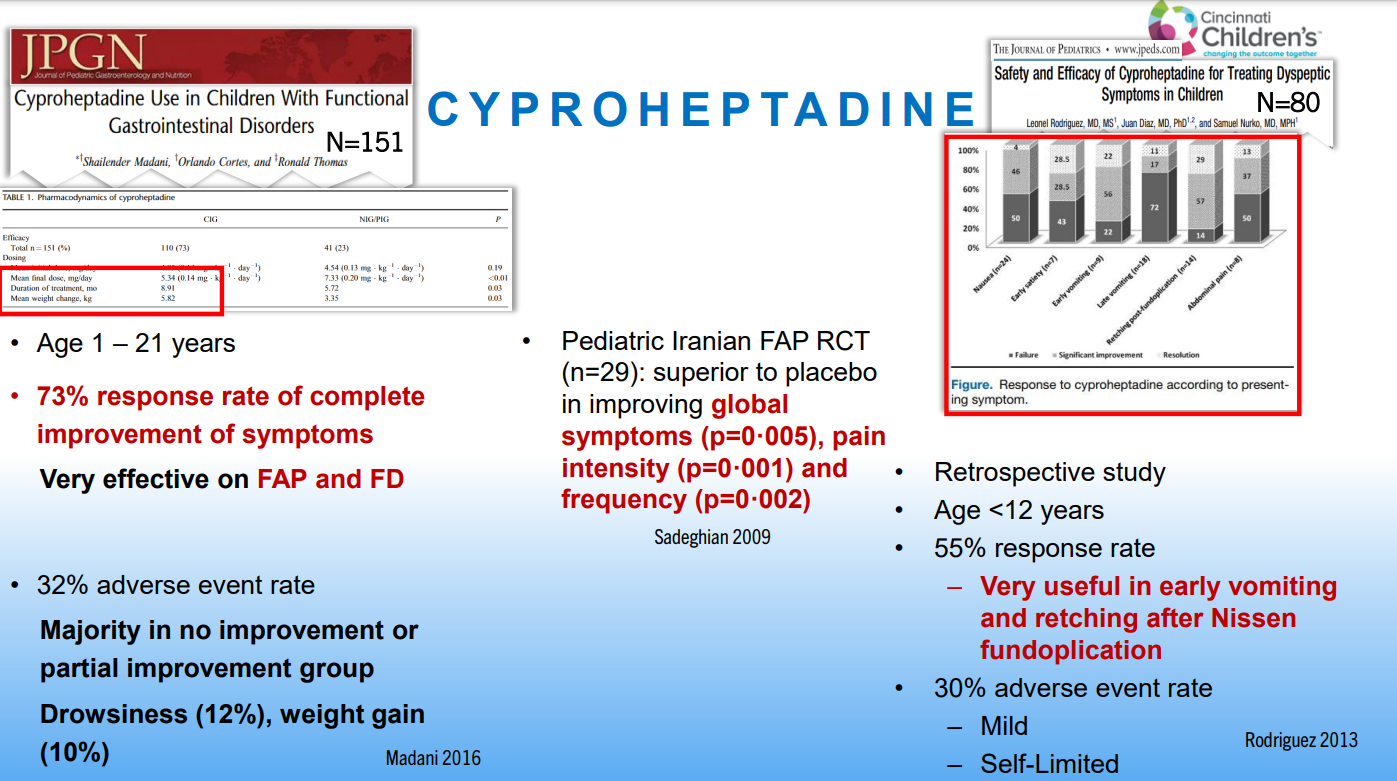
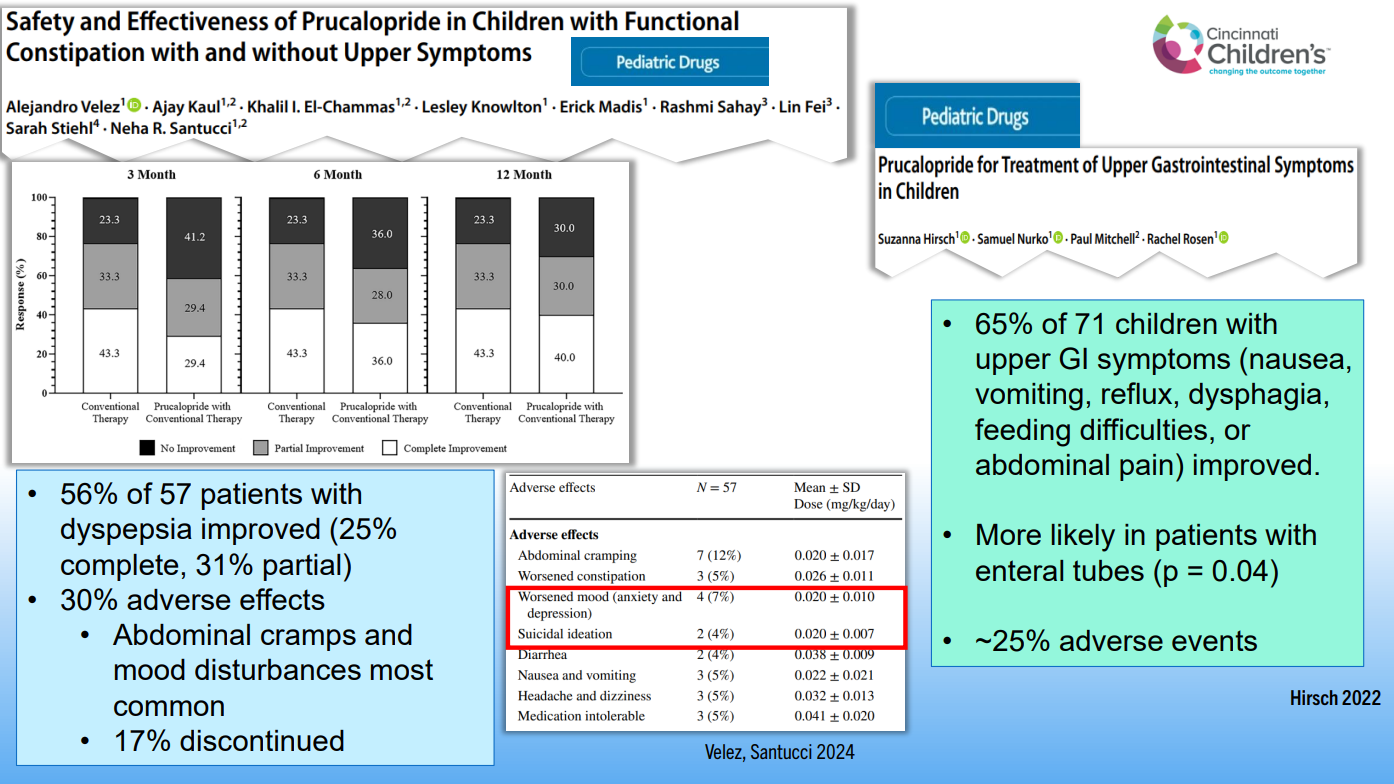
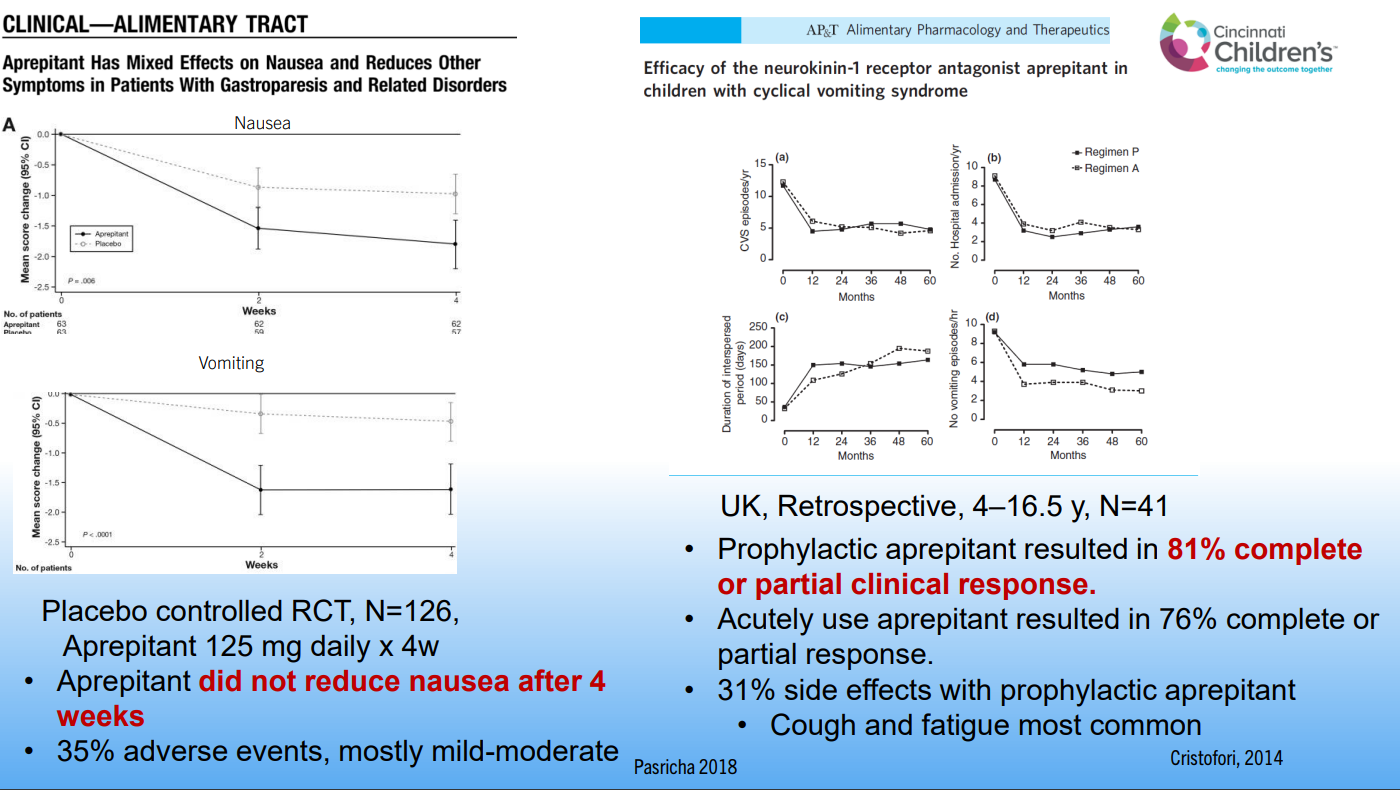
Dr. Santucci reviewed the evidence for linaclotide, cyproheptadine, mirtazapine, prucalopride, and aprepitant. The latter was effective for CVS but not functional nausea.
Placebo has been shown to have some beneficial effects in DGBIs; this affects the results of clinical trials
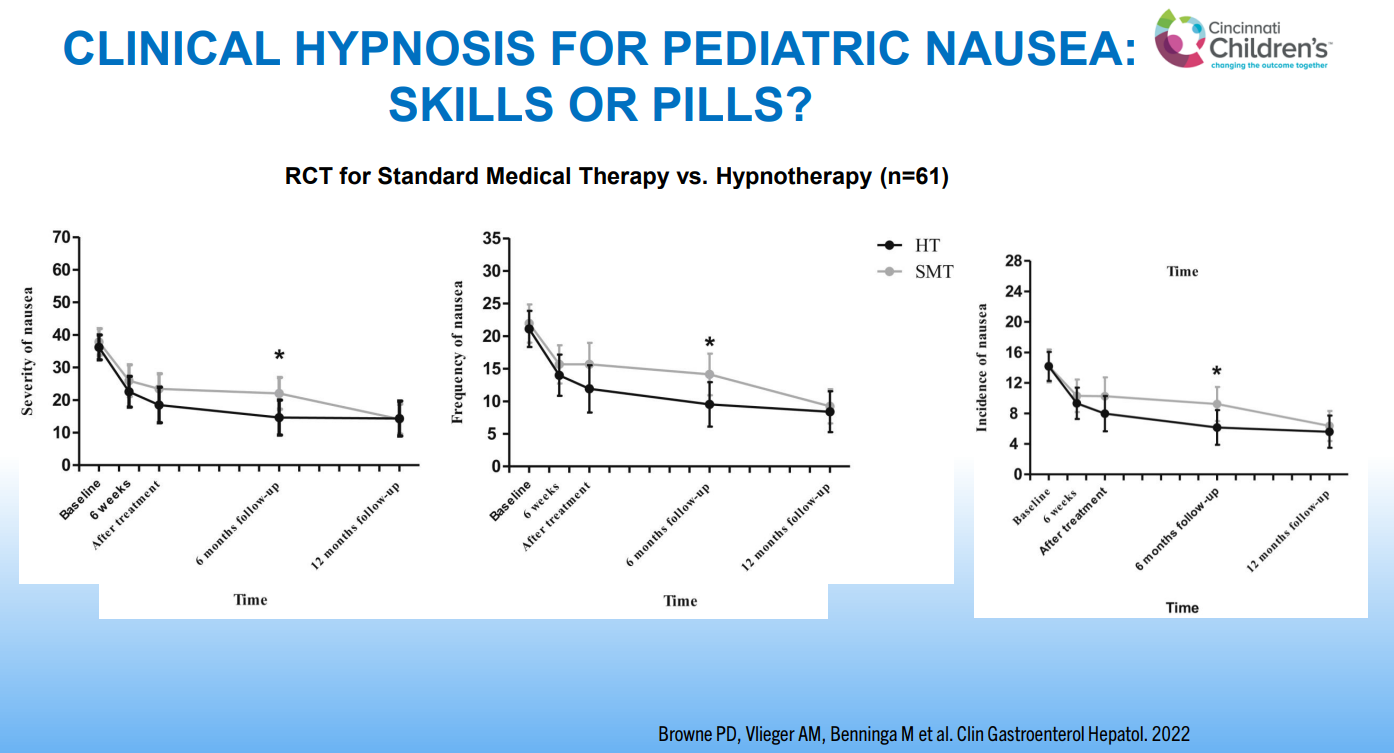
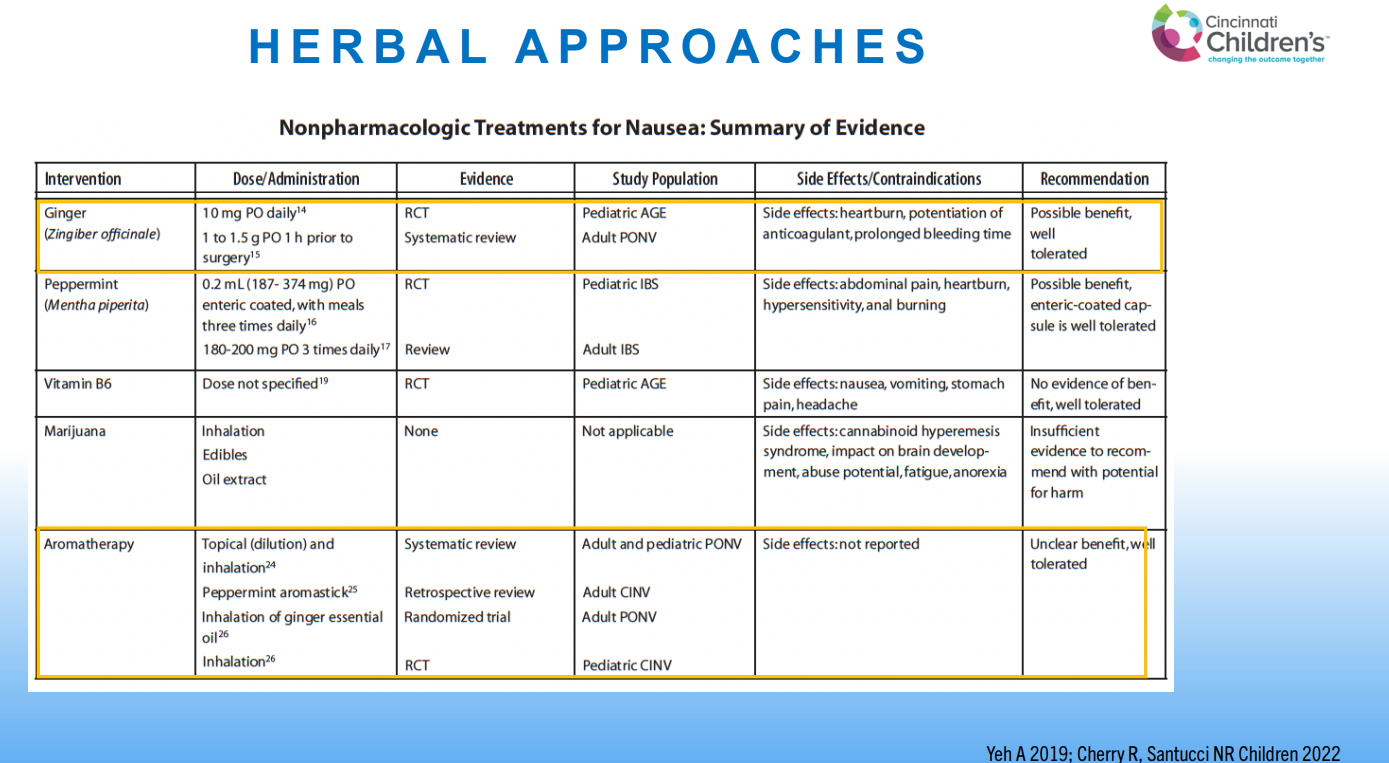
Ginger may be beneficial for nausea
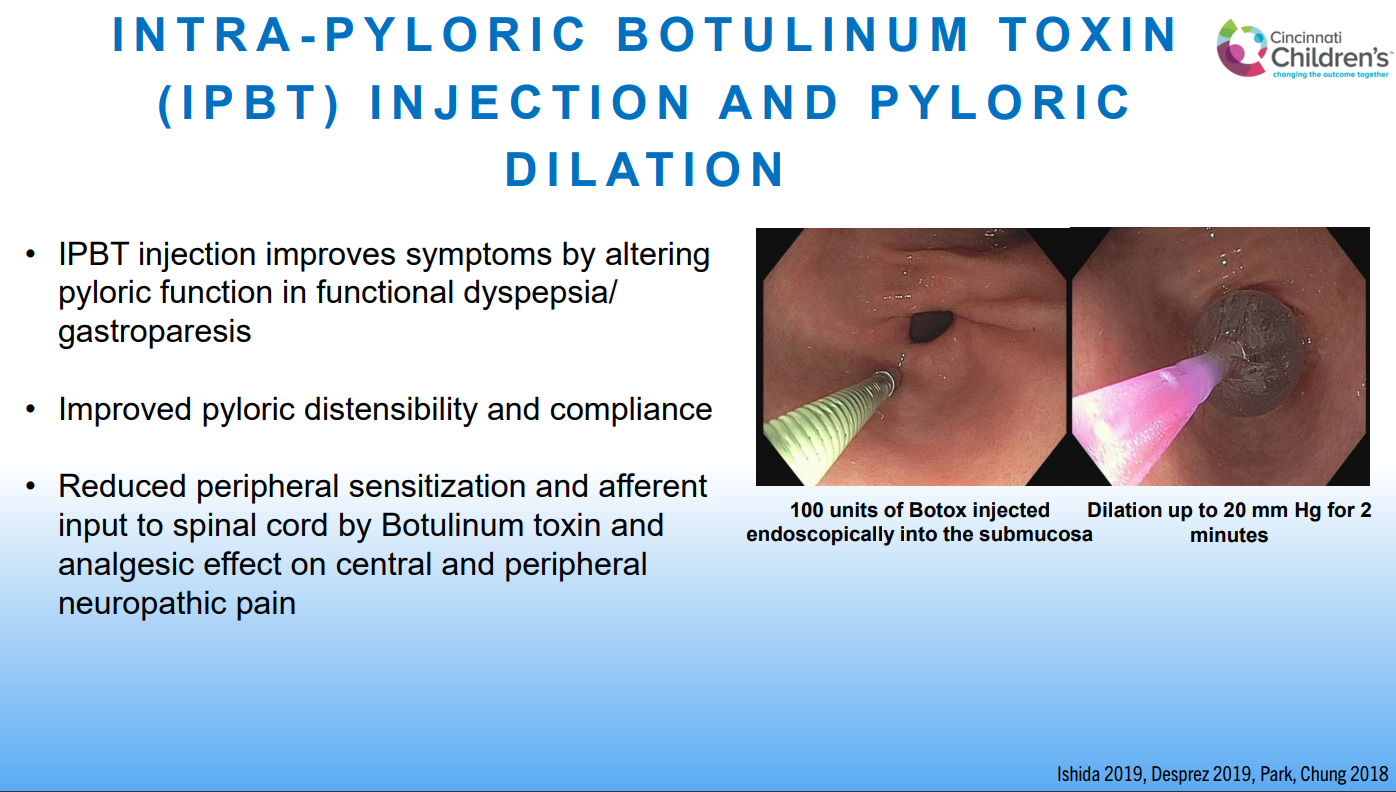
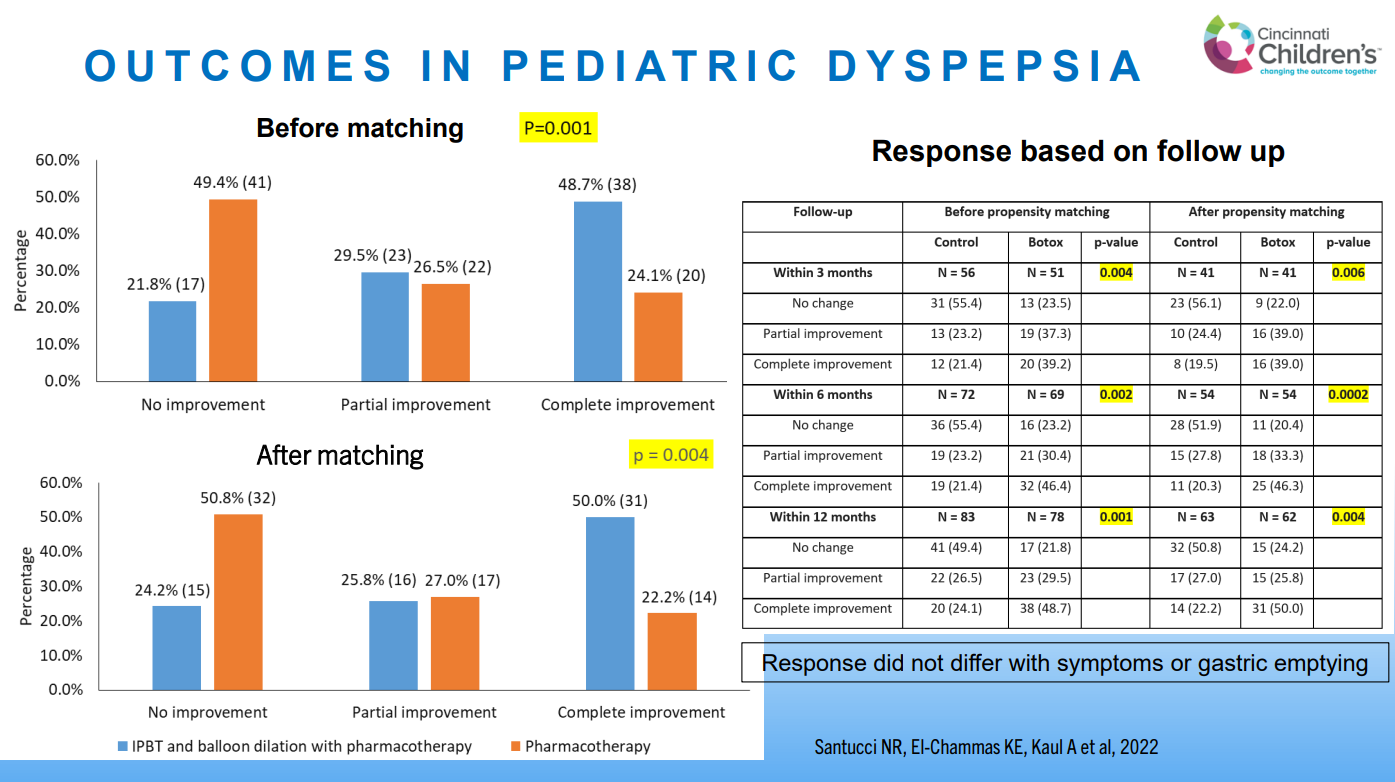
Intrapyloric botox has been associated with improvement in functional dyspepsia. Improvement did not correlated with gastric emptying
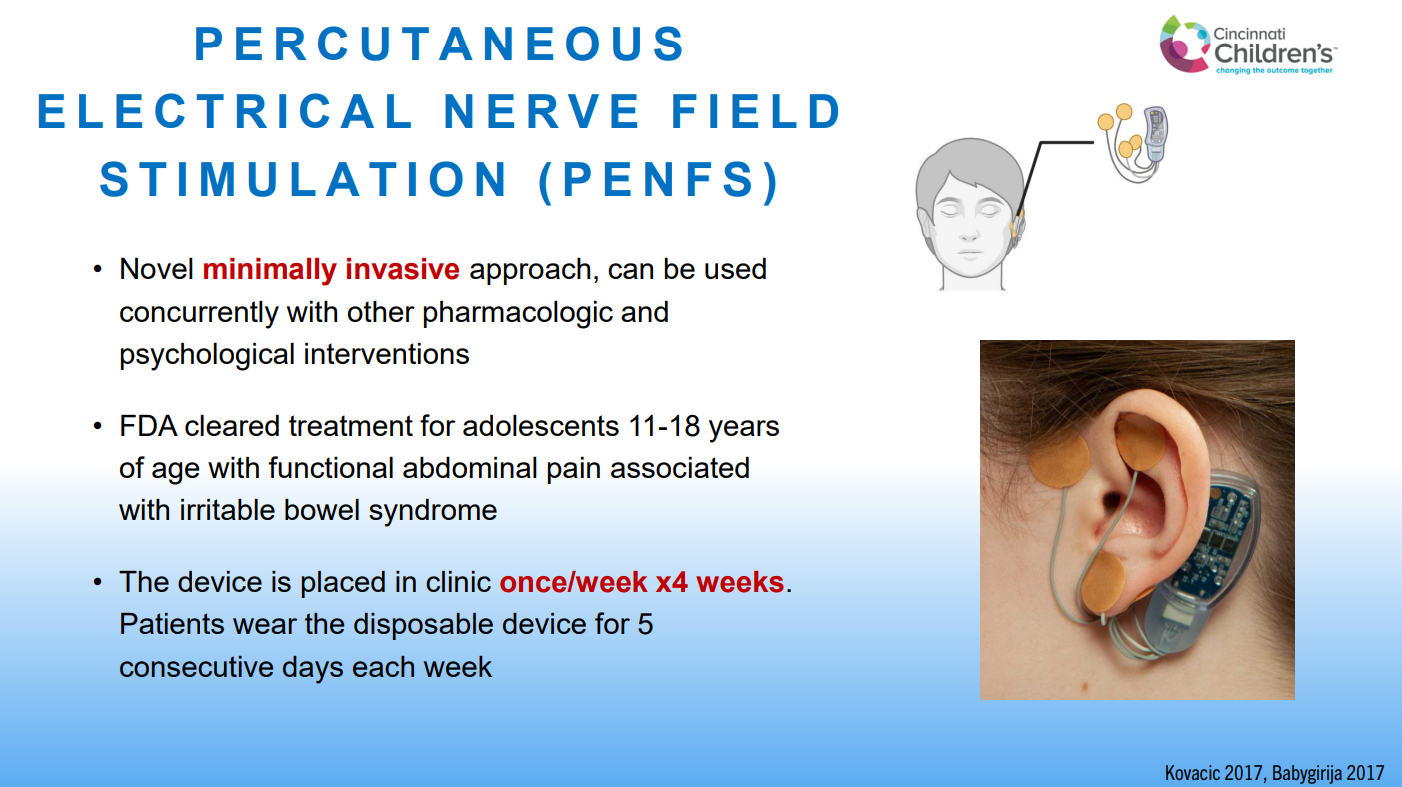
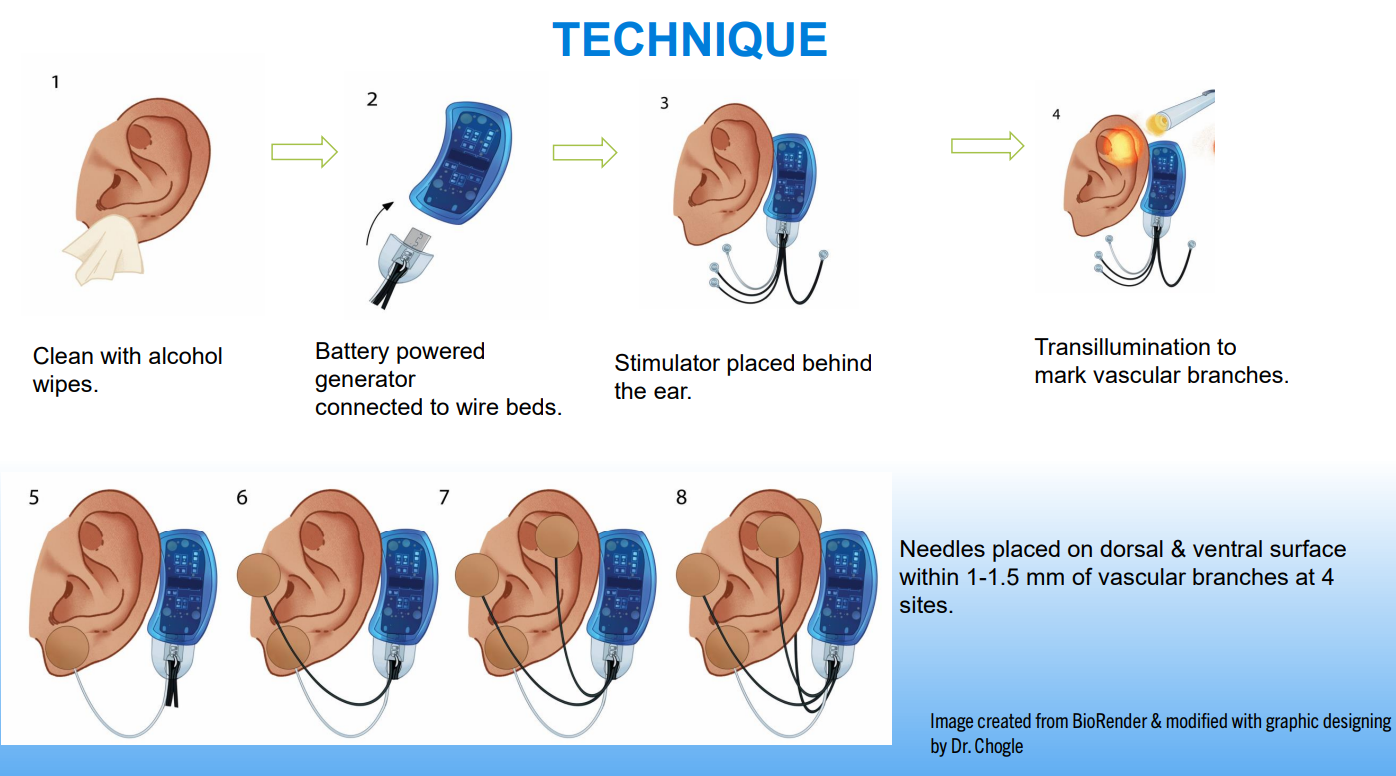
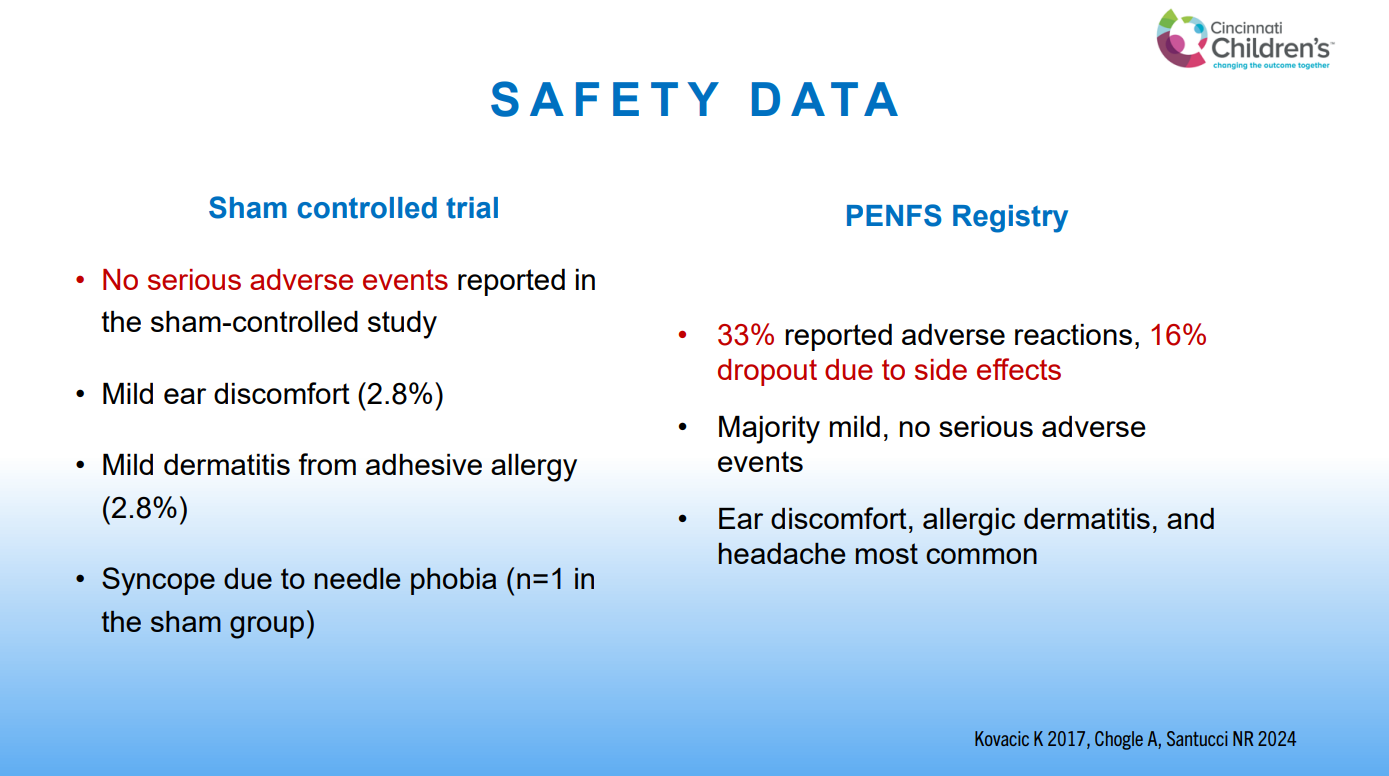
Percutaneous electrical nerve field stimulation (PENFS) is associated with improvement in multiple aspects of functional disorders including pain, nausea, somatization, sleep and anxiety.
The improvements in abdominal pain and functional disability with PENFS are still present at least 6-12 months afterwards
PENFS can be repeated and has similar effectiveness
PENFS can be used in children >8 yrs, can be used with other treatments (pharmacologic, psychologic, or dietary).
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
Recently, Dr. Neha Santucci gave our group an excellent update on disorders of gut-brain interaction. My notes below may contain errors in transcription and in omission. Along with my notes, I have included many of her slides.
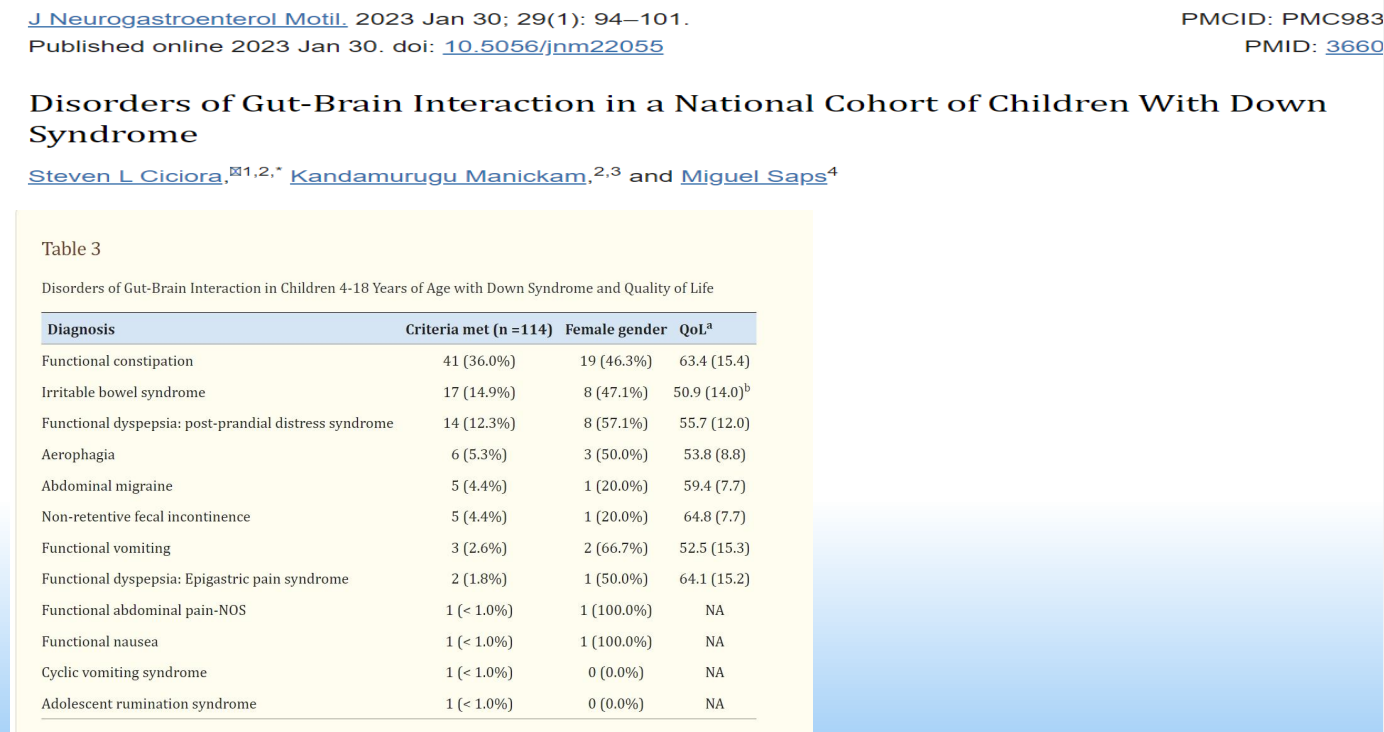
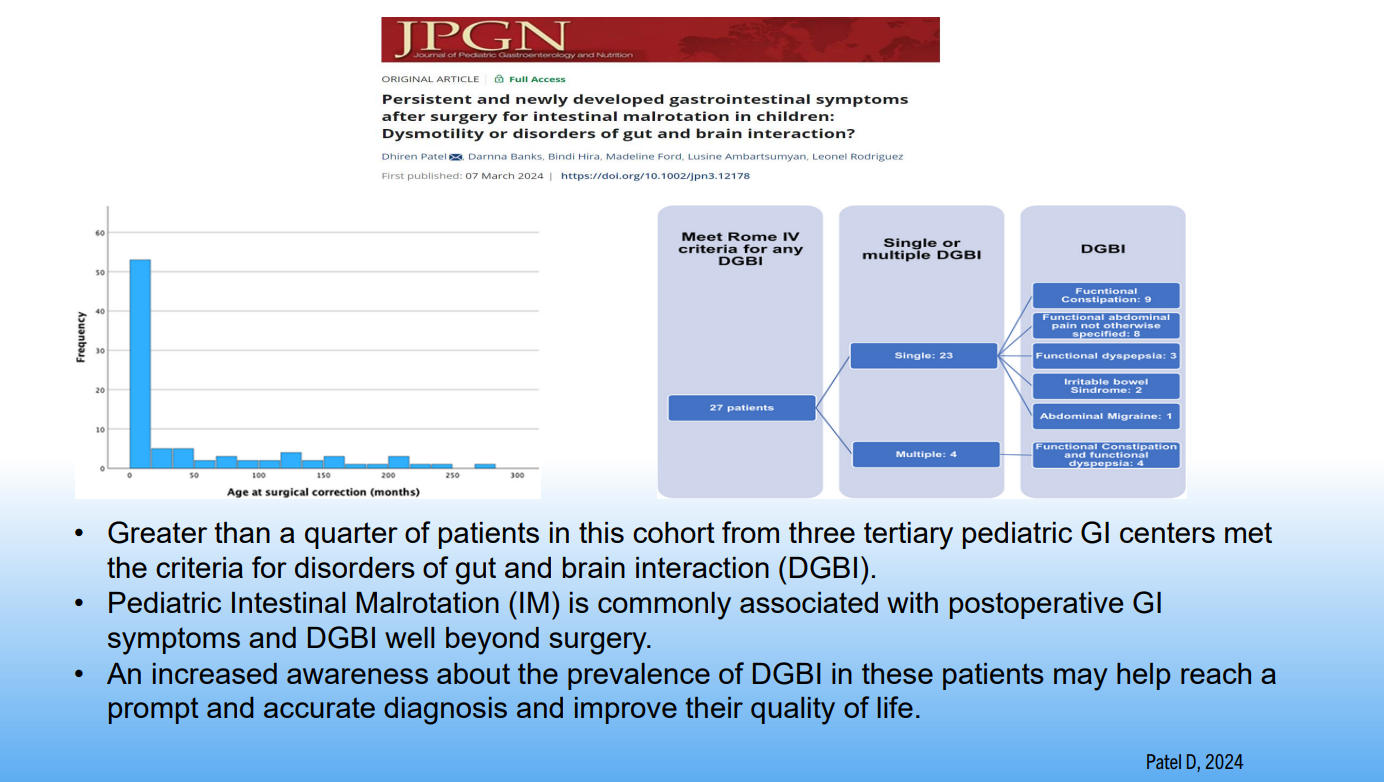
John Apley’s monograph The Child with Abdominal Pains provided an early understanding of the prevalence of DGBIs.An increase in DGBIs occurred with COVID. This study in adults showed a greater increase in functional dyspepsia compared to IBS. DGBIs occur in Children with Down syndrome. This cohort showed high rates of functional constipation (36%), irritable bowel syndrome (14.9%), functional dyspepsia (12.3%) and aerophagia (5.3%).DGBIs were common after surgery for malrotation
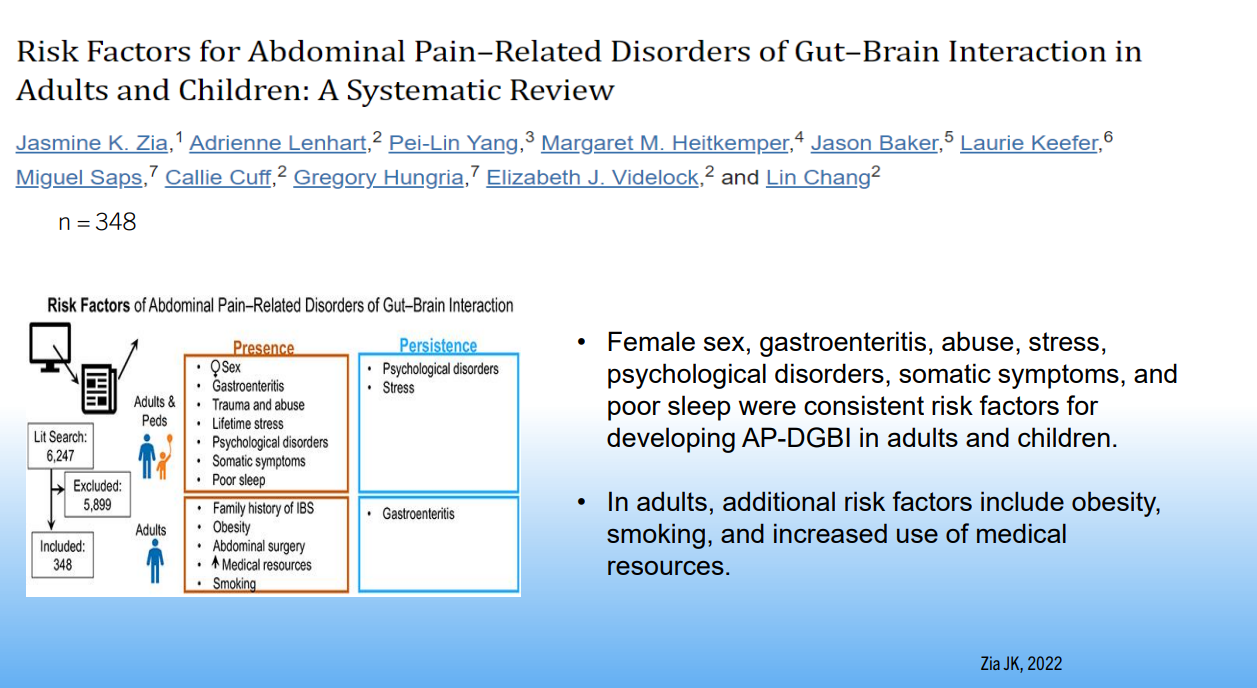
Development of DGBIs is influenced by psychological factors, early life events, chronic stress, gut motility, inflammation, mucosal immune activation and altered gut microbiota
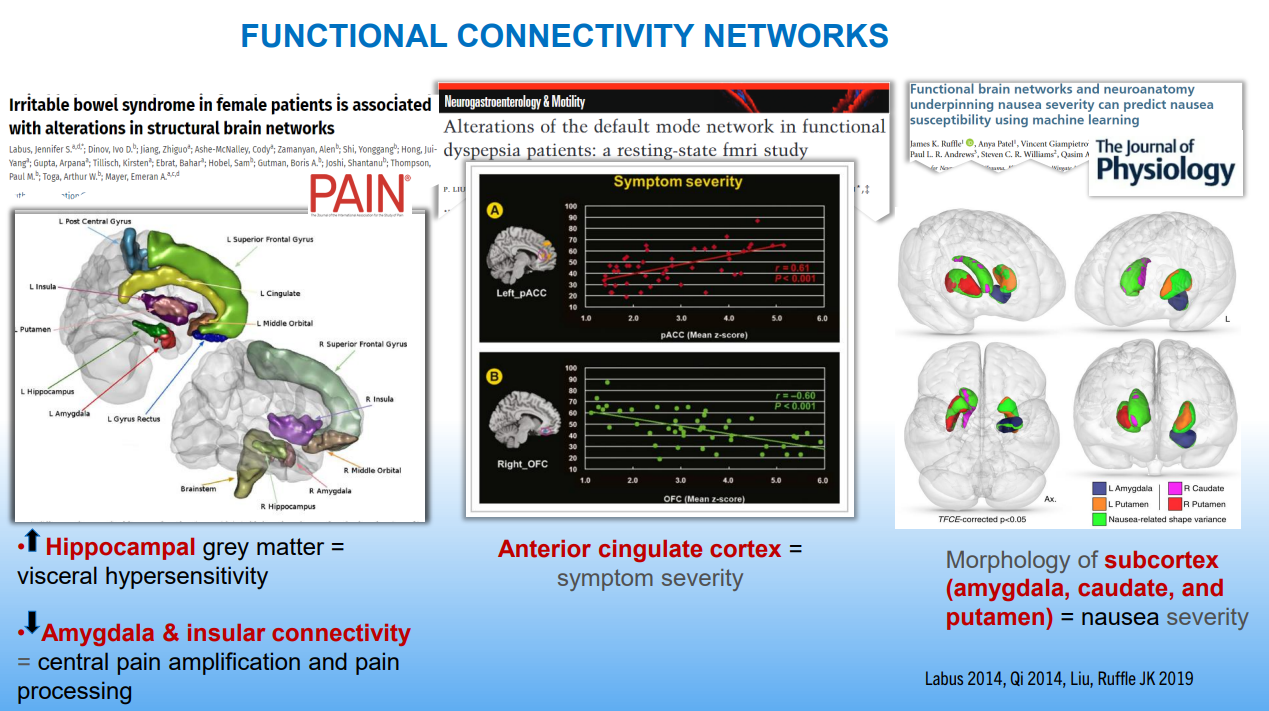
DGBIs are associated with altered brain networks
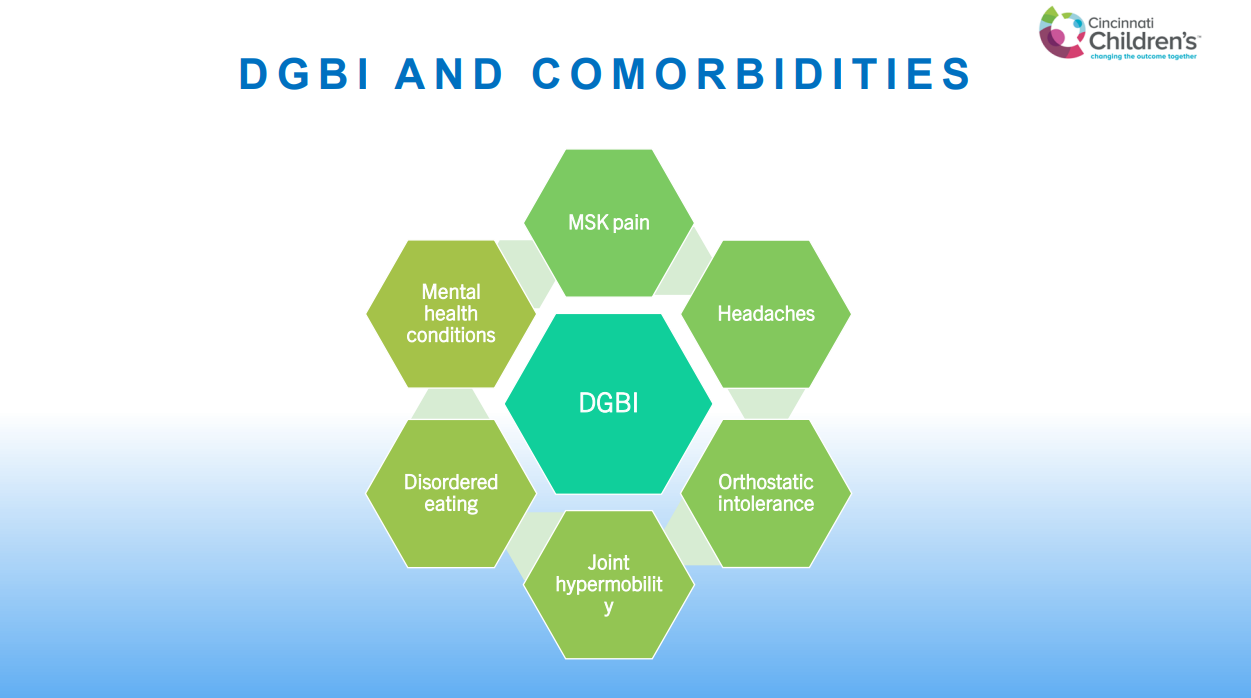
DGBIs are associated with a number of comorbidities including mental health disorders, joint hypermobility, headaches, POTS, musculoskeletal pain, disordered eating, and poor sleep
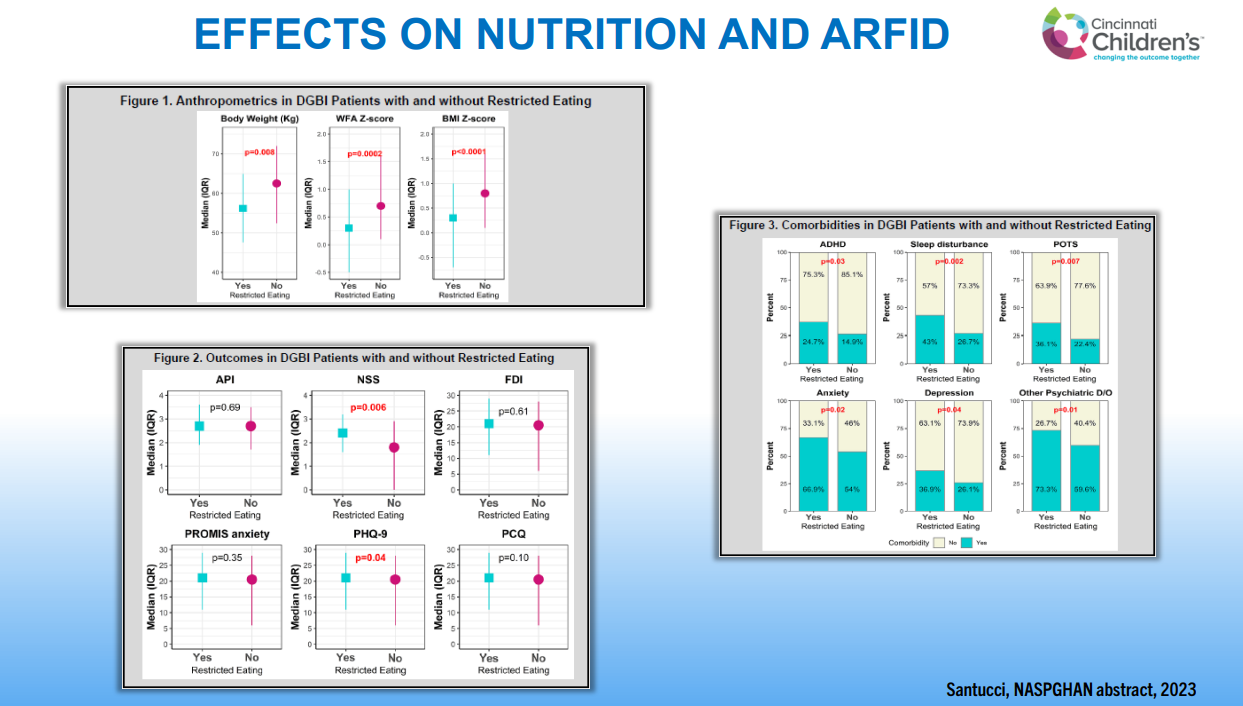
Individuals with DGBIs are at increased risk of eating disorders including ARFID. Presence of ARFID with DGBIs has been associated with more anxiety, depression, ADHD and sleep disturbance
Poor sleep in previous night is associated with increased pain the next day in individuals with DGBIs
DGBIs are common in children with organic diseases, including IBD, EoE, Celiac disease, Recurrent Pancreatitis, Malrotation and Anorectal disorders
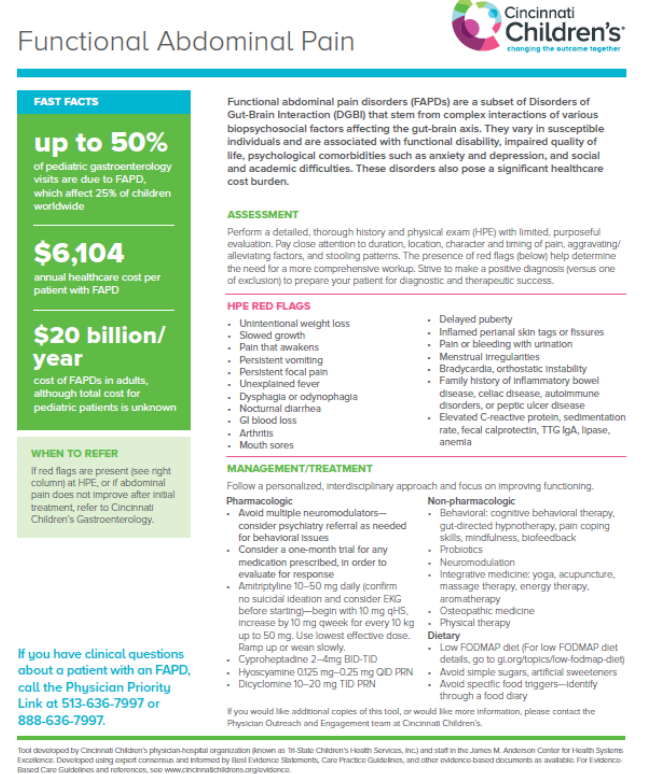
Up to 50% of pediatric GI visits are for functional disorders and ~25% of all children have DGBIs
Strive to make a positive diagnosis (rather than simply a diagnosis of exclusion)
Avoid excessive testing
Dyspepsia and gastroparesis are not distinct disorders and likely exist on a spectrum (some of the same treatments for both)
First treatment goals: develop a good rapport with family and focus on improved functioning
Children with DGBIs had more problems with coping skills.Individuals with DGBIs are at increased risk of eating disorders including ARFID. Presence of ARFID with DGBIs has been associated with more anxiety, depression, ADHD and sleep disturbance.Initial treatment needs to address these questions
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
A Watson et al. JPGN 2024;79:1081–1083. Cat scratch colon in a patient with very early-onset Crohn’s disease with diverting ileostomy
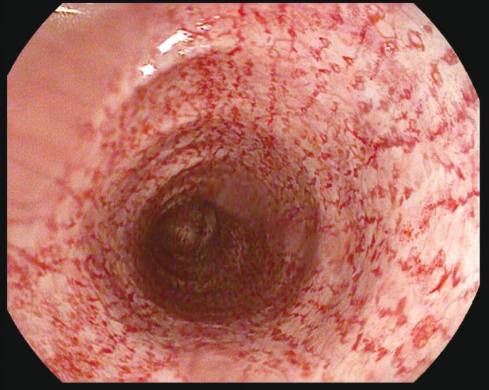
Case report: This image is from the ascending colon of a 12 yo with Crohn’s disease sp diverting ileostomy.
“Cat scratch colon refers to the rare endoscopic finding of erythematous linear breaks that arise spontaneously, typically in the ascending colon and/or cecum, resembling scratches made by a cat, on otherwise unremarkable mucosa…It is presumed to be a benign condition likely caused by barotrauma from air insufflation during colonoscopy in a colon with altered elasticity or when the rate of insufflation exceeds the rate of air passage, such as in a diverted colon.2, 3“
My take: Surprisingly, the cat scratch colon finding is not consequential.
From the summary of the study by Dr. Keszthelyi-a few excerpts: Background: “Blastocystis is the most common gastrointestinal protist found in humans and animals… At the same, Blastocystis remains one of the most enigmatic gut microbial organisms that has puzzled clinicians for decades… scores of patients with positive stools for Blastocystis have been treated with antimicrobial agents such as metronidazole.”
Methods: “Piperni et al examined 8 of these STs previously described in humans in a global-scale metagenomic exploration in 56,989 individuals from 32 countries. The analysis also included 4590 gut metagenomes from 214 nonhuman species (spanning mammals, reptiles, birds, amphibians, insects, crustaceans, mollusks, nematodes, and metazoans) from 49 public datasets, and paleofeces based on 28 publicly available ancient human gut metagenomic samples with archaeological dating ranging from 3000 BC to the Post-Medieval Age.”
Key findings:
“Blastocystis was found in 8190 human stool samples and was fairly common in healthy individuals (16%). Blastocystis was hardly ever found in newborns, suggesting that it is likely acquired later in life and not vertically transmitted”
“The 8 human Blastocystis STs were not detected in most of the animal species tested, except for nonhuman primates kept in captivity”
“Blastocystis was detected in ancient human samples”
“The presence of Blastocystis was positively associated with more favorable cardiometabolic profiles and negatively with obesity. In addition, adherence to a plant-based diet was associated with carriage of Blastocystis.”
“In particular, individuals who consumed higher quantities of unprocessed plant-based foods, such as avocados, dried fruits, nuts, seeds, legumes, and cruciferous vegetables, were more likely to be Blastocystis-positive compared with individuals with lower intake of such foods.”
Implementing “a 6-month personalized diet intervention study involving 1124 individuals, in which improvements in dietary quality and weight loss were paralleled with an increase in Blastocystis abundance.”
My take: The authors of the Cell study: “our results linking Blastocystis to host health support its non-pathogenic, if not favorable, role.”
For the Green family, the memory of Oct. 1, 1994 is many things at once: the date of their greatest pain and their finest hour; a day of unspeakable loss and life-giving gifts.
It is the date their 7-year-old son, Nicholas, died in an Italian hospital, two days after being shot during an attempted robbery on a family vacation from California…
Seven people, five of them teenagers, received Nicholas’ corneas, kidneys, liver, heart and pancreas. The family’s story prompted a surge in interest that continues to drive new donor registrations in Italy…
At the time, Italy had one of the lowest organ donation rates in Western Europe. The Greens’ decision, along with the awful circumstances of the boy’s death, led to a swell of media attention across Italy…The year before Nicholas’ death, 6.2 people per million in Italy donated their organs. Ten years later, as the story circulated and the numbers of parks, playgrounds and streets in Italy named after Nicholas grew, the number had tripled to nearly 20 people per million…
Over the years, members of the family have made dozens of trips to Italy to speak on behalf of organ donation and to check in on the people whose lives were saved by their loss…five are still living. His liver recipient, who was 19 at the time of the transplant, went on to marry and have children. The Greens have met her eldest son. His name is Nicholas.
Potassium-competitive acid blockers are generally not recommended as first line therapy. This rationale is based on cost, greater obstacles to obtaining medication, and fewer long-term safety data.
Clinicians may use P-CABs in selected patients with documented acid-related reflux & erosive esophagitis who fail therapy with twice-daily PPIs.
Clinicians should use P-CABs in place of PPIs in eradication regimens for most patients with H pylori infection.
P-CABs may be beneficial in high-risk bleeding peptic ulcer disease. “Although there is currently insufficient evidence for clinicians to use P-CABs as first-line therapy in patients with bleeding gastroduodenal ulcers and high-risk stigmata, their rapid and potent acid inhibition raises the possibility of their utility in this population.”