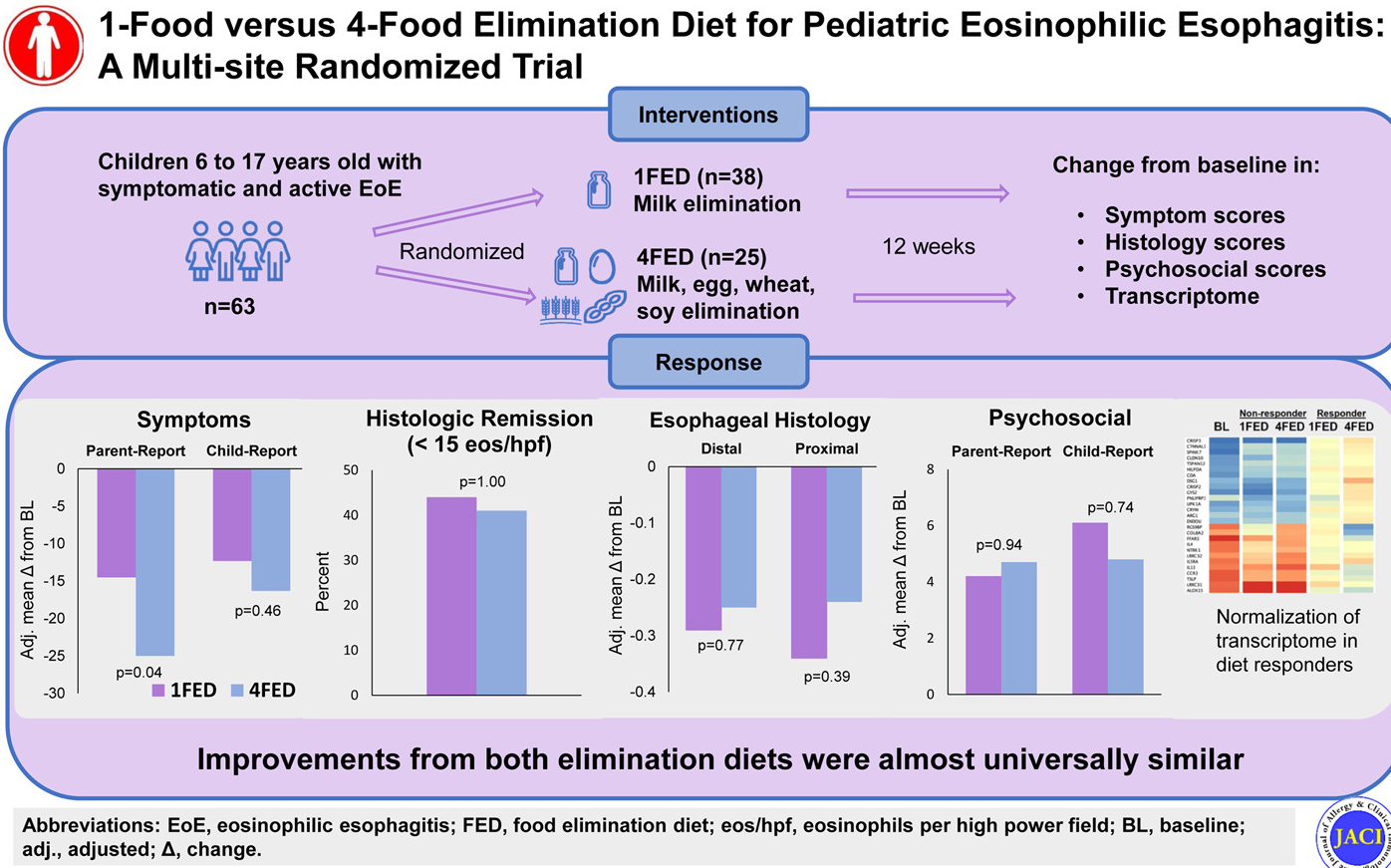
Methods: This was a multisite, randomized comparative efficacy trial of a 1-food (milk) elimination diet (1FED) versus 4-food (milk, egg, wheat, soy) elimination diet (4FED) in pediatric EoE. The 12-week study enrolled 63 patients (6-17 yrs). Primary end point was symptom improvement by Pediatric Eosinophilic Esophagitis Symptom Score (PEESS).
Key findings:
1FED vs 4FED: The mean PEESS improved −25.0 versus −14.5 (P = .04), but remission rates (41% vs 44%; P = 1.00), histology scoring system (−0.25 vs −0.29; P = .77), endoscopic reference score (−1.10 vs −0.58; P = .47), and QoL scores were similar between groups.
The 4FED withdrawal rate (32%) exceeded that of 1FED (11%) (P = .0496).
My take: A 4FED diet is difficult to maintain. In this 12 week study, more than 30% of patients withdrew from the 4FED diet. In addition, dairy elimination alone resulted in similar response rates.
Recently, Dr. Sana Syed gave Children’s Healthcare of Atlanta Grand Rounds. She provided an excellent update on the development of artificial intelligence (AI) to select targeted therapies for pediatric gastroenterology diseases. My notes below may contain errors in transcription and in omission. Along with my notes, I have included many of her slides.
Key points:
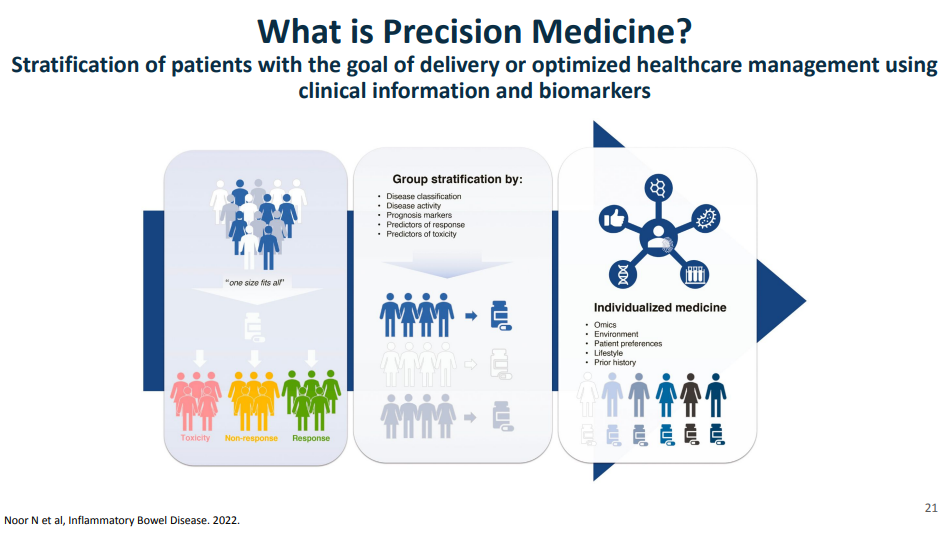
One of the goals of using AI is to identify the right therapy at the time of diagnosis. Currently, diseases like eosinophilic esophagitis (EoE) and Crohn’s disease have multiple treatment options. However, many patients do not respond to first-line treatments; many develop complications due to not responding to treatment.
Currently we are lacking adequate biomarkers for individualized therapy. AI has the potential to sort through massive amounts of data (histologic, genetic, pharmacokinetics, transcriptome, metabolomics, etc) to allow for precision therapy.
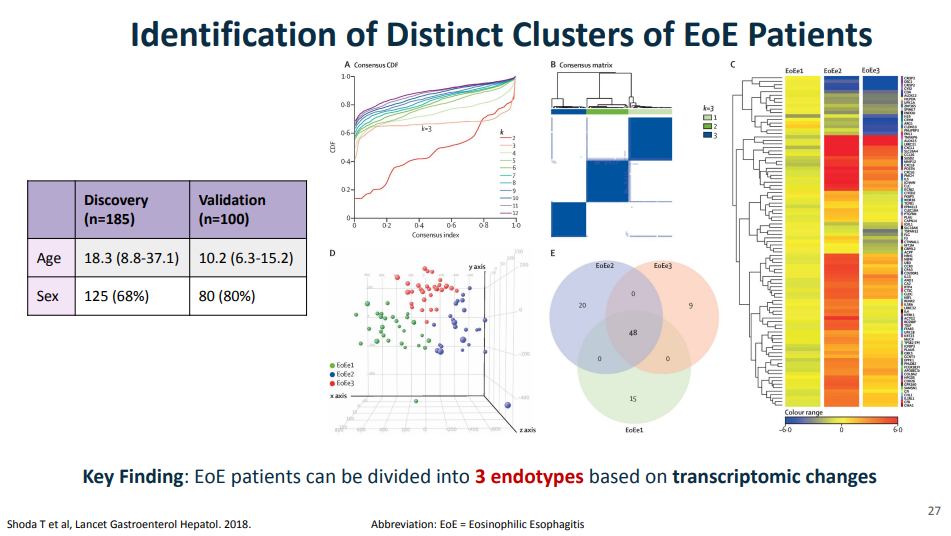
For EoE, machine-learning has already identified three subtypes that may affect clinical management. EoE1 is associated with a normal-appearing esophagus. EoE2 is associated with being steroid refractory. EoE3, when compared to the other two endotypes, is associated with adult-onset and narrow-caliber esophagus or stricturing.
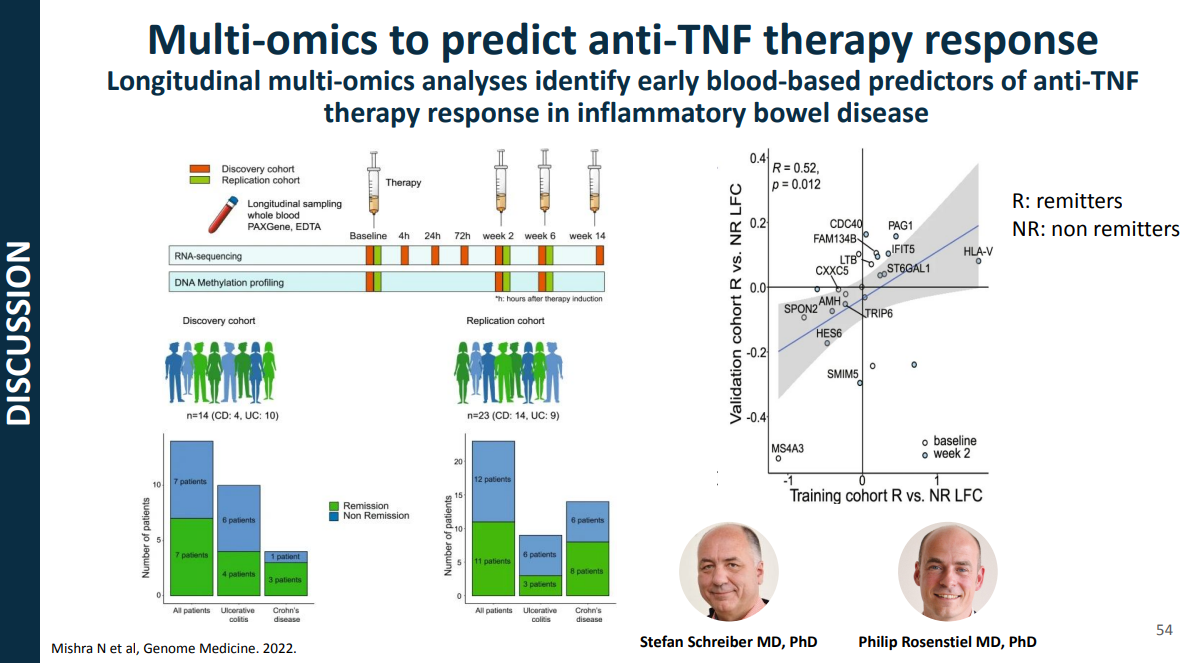
For Crohn’s disease, research has shown that younger age has been associated with an increased risk of not responding to anti-TNF therapy
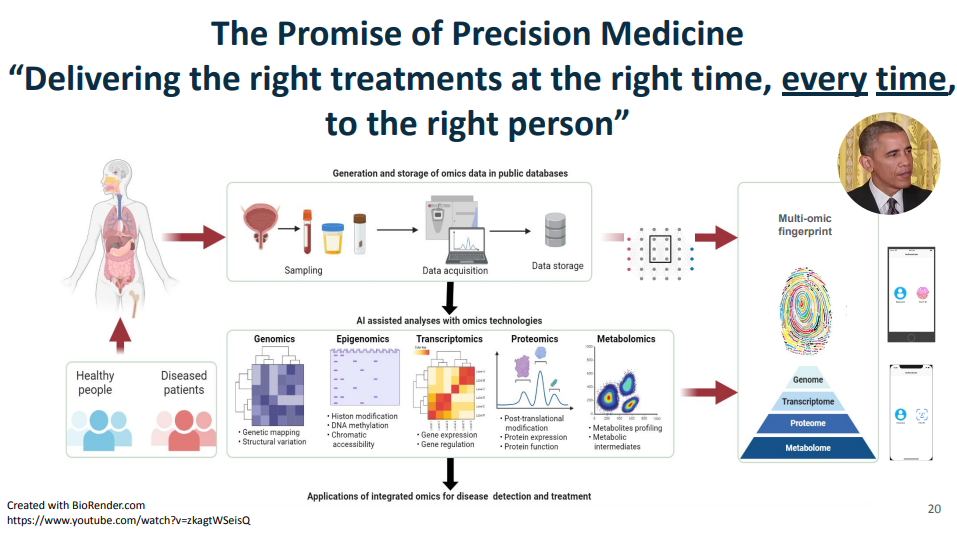
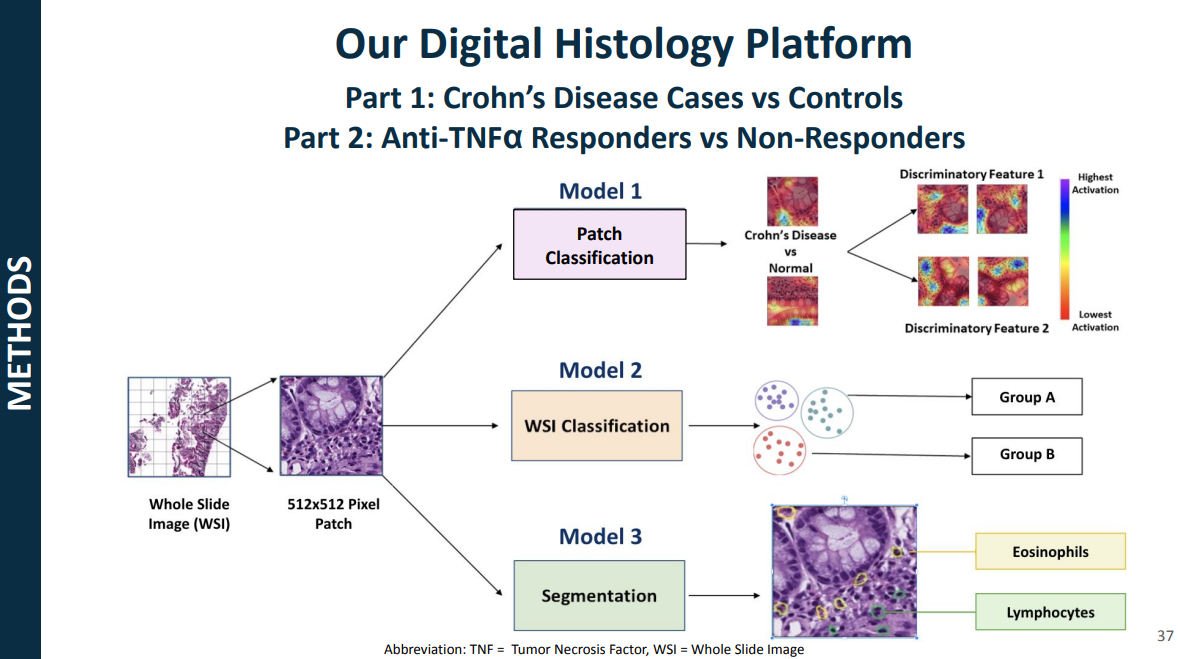
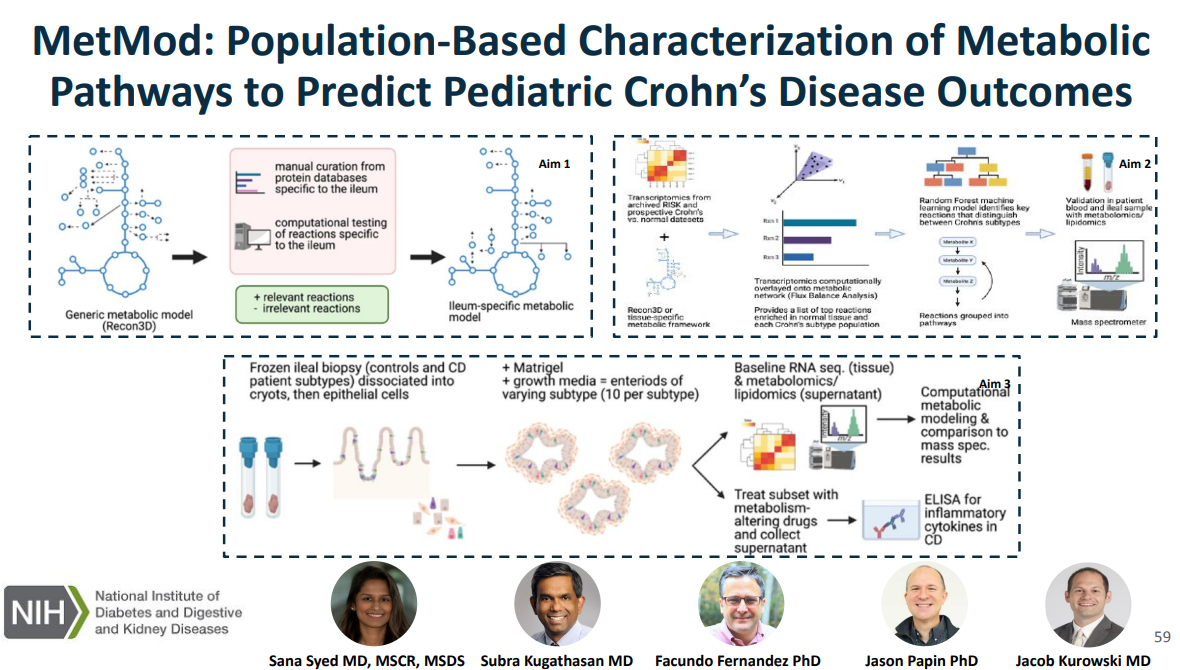
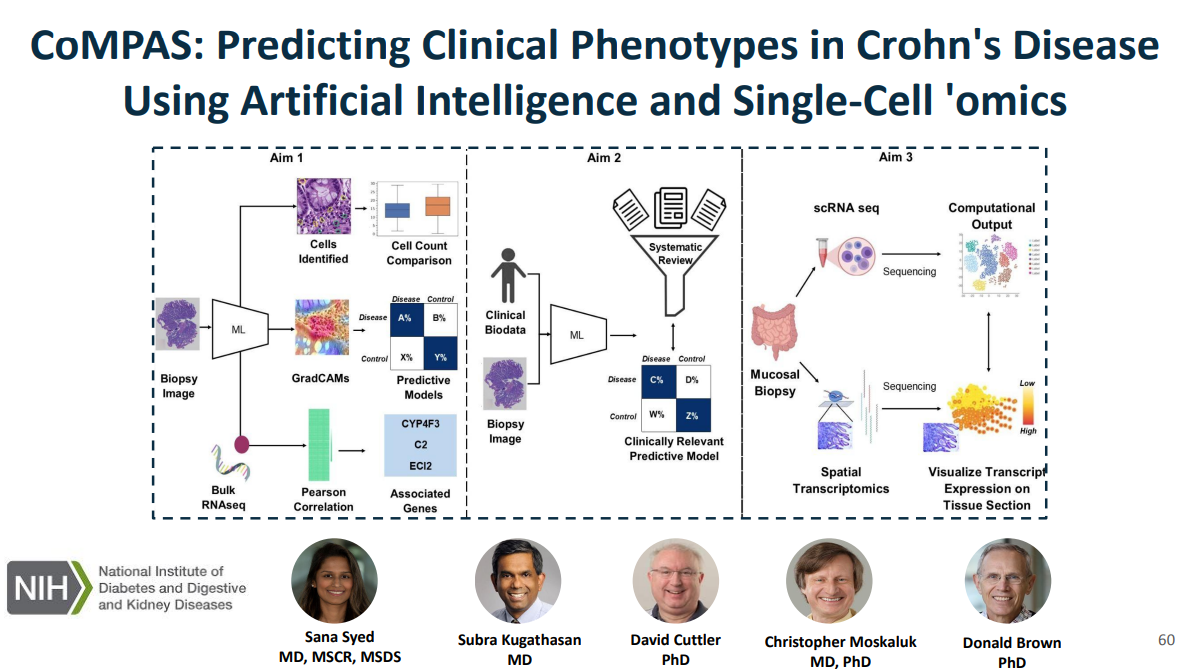
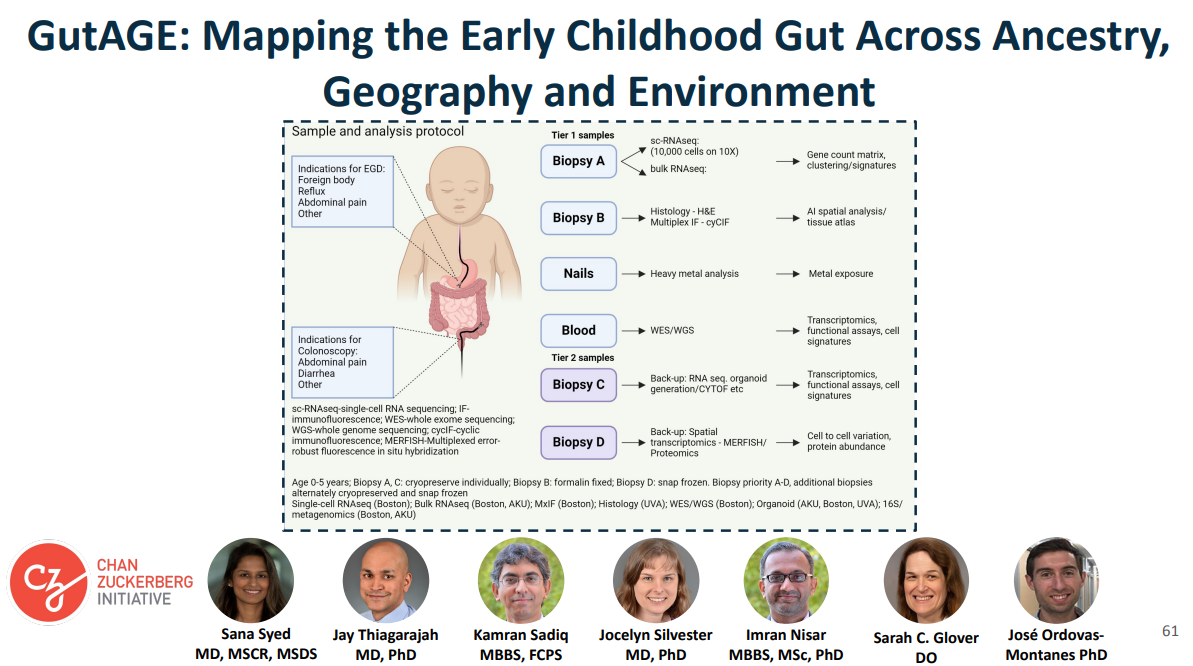
This is a quote from President Obama when his administration announced massive funding toward precision medicine in January of 2015, that the promise of precision medicine is ”delivering the right treatments at the right time, every time to the right person.” This figure illustrates some of the kinds of data that Dr. Syed had access to as faculty at UVA, including genomics, epigenome, transcriptomics, proteomics, metabolomics, etc.Shoda and colleagues, used a combination of histology data, endoscopic features, histologic and endoscopic scoring indices, and transcripts that make up the eosinophilic esophagitis diagnostic panel, a quantitative PCR assay with 96 EoE representative genes. The key message from all of those visualizations is that they found that EoE can be divided into three distinct endotypes after analyzing transcriptomics changes via partition-around-medoid clustering, a machine-learning method.In this project, the researcher intend to curate a novel metabolic network specific to the ileum, which is relevant to Crohn’s disease, link metabolic processes with Crohn’s disease phenotypes using in silico metabolic network modeling and ‘omics and characterize and target metabolic pathways in an organoid model generated from patient-derived Crohn’s disease tissue.In CoMPAS, the researchers aim to leverage artificial intelligence methods (AI) methods to build predictive models for CD using histology slides and single-cell RNA sequencing, allowing for risk stratification of B1 patients who will respond to anti-TNF therapyThe goal of our project is to create a multi-omics reference dataset with scRNA-seq data coupled with contextual data on tissue morphology, ancestry, social determinants of health, and the environment. The cohort for this study is enrolling patients who have clinical indications for endoscopy like foreign body removal, reflux, abdominal pain
My take: This work is necessary to identify the right treatments for each patient and will lead to better outcomes. We are already seeing the early stages of machine-learning’s impact on clinical care. In many other fields, AI work is much further along (especially in oncology). A recent study in Nature identified JAK inhibitors as potential life-saving therapy with toxic epidermal necrolysis (TEN).
Reference: Nordmann, T.M., Anderton, H., Hasegawa, A. et al. Spatial proteomics identifies JAKi as treatment for a lethal skin disease. Nature (2024). https://doi.org/10.1038/s41586-024-08061-0
Summary from Eric Topol (Ground Truths) focusing on spatial omics: Thierry Nordmann, Matthias Mann and their international consortium, used deep visual proteomics from 3μm PPFE sections of skin biopsies in patients affected by TEN…
More than 5,000 proteins were quantified from single cells—keratinocyte and immune cells—using mass spec, for the 4 different skin conditions (proteome cluster in Figure below, left panel). This led to the finding that the TEN patients had marked increased in Type 1 and 2 interferon signaling and activation of phosphorylated STAT1, which invoked the janus kinase (JAK/STAT) pathway. Subsequent steps were to test JAK inhibitors in cell culture (with live cell imaging) and in two different mouse models, all showing highly potent, dose-dependent impact on inhibition of the intense inflammatory process and disease severity…
They went on to treat seven patients at Fuian Medical University, the course of one patient shown below, treated with a JAKi on day 4 after diagnosis, and manifesting a marked response starting within 48 hours. All 7 patients fully resolved, with no side effects…
For spatial medicine, there are multiple analytical challenges that invoke the need for machine learning and A.I., including segmentation of cell types, automated capture of cells of microdissection, extracting useful information from the >5,000 proteins quantified per cell, and ultimately, as we’ll see more in the future, A.I. powering the construction of high-resolution 3D maps.
This report makes 52 statements and 44 recommendations. Overall this is a helpful report but there are many statements and recommendations that have NO value for pediatric gastroenterologists (except for those trapped in a cave for the last 10 years). Here are a couple examples of that:
“ESPGHAN EGID WG recommends that pediatricians should be aware of the higher incidence of EoE in relatives.”
“ESPGHAN EGID WG recommends that a high index of suspicion for EoE must be maintained in children with concomitant atopic disease.”
“ESPGHAN EGID WG recommends the peak value of 15 eos/HPF as the cut‐off value in esophageal biopsy specimens, for the histological diagnosis of EoE in an appropriate clinical context”
Some helpful recommendations:
“ESPGHAN EGID WG recommends against using available allergy tests to predict dietary triggers of EoE.” This is not new information but helpful to have clearly stated in guidelines.”
“ESPGHAN EGID WG recommends maintenance therapy to all patients after achieving histological remission” Commentary: “There are no prospective data on the best duration of maintenance therapy in pediatric EoE…[In a large study of adults} sustained untreated combined remission was seen in only 1.3% of patients who discontinued treatment.”
“ESPGHAN EGID WG suggests endoscopic and histological re‐evaluation after 1‐3 years during the maintenance phase in cases of stable clinical remission”
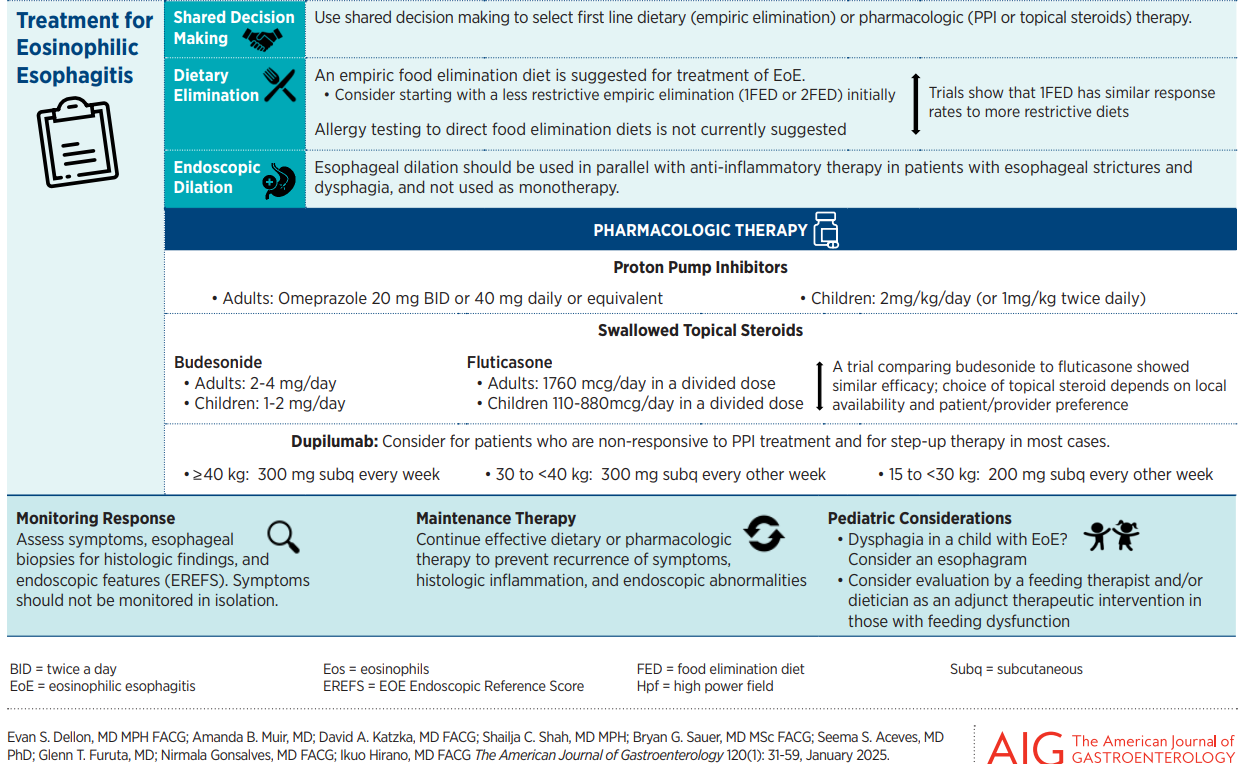
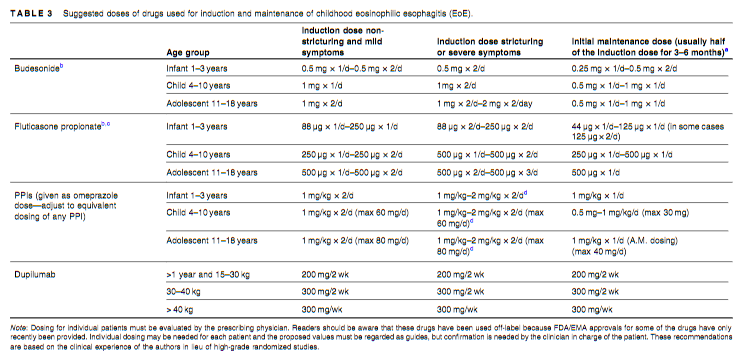
“ESPGHAN EGID WG recommends that dupilumab can be used in selected cases of children over1 year old weighing >15 kg with EoE refractory to conventional treatment and in those with concomitant atopic burden with approved indications for biologics”
“ESPGHAN EGID WG suggests that a short course of systemic steroids be considered as an alternative to dilation in the presence of moderate to severe esophageal strictures with severe symptoms.” “Treatment with short term systemic steroids can significantly reduce the need for mechanical esophageal dilation in moderate to severe strictures associated with pediatric EoE”
Suggested drug dosing is noted in Table 3 (see below)
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
The authors retrospectively studied a cohort of children (n=782) with eosinophilic gastrointestinal disorders (EGID) including 592 with isolated eosinophilic esophagitis (EoE), 190 with EGID which included esophageal involvement (“EI”) and 35 EGD without esophageal involvement (“Non-EI”).
Key findings:
Abdominal pain was more frequent in EI than isolated EoE: 61% vs 45%, p=.002)
EI patients had more dense esophageal eosinophil infiltrate (peak) than isolated EoE: 115 vs 92; P=.036) and higher peripheral blood eosinophil level (0.44 vs 0.38; p=0.027)
94-Gene expression profiles from esophageal biopsies from a 168 subgroup showed that EoE and EI were not significantly different. The heat map for upregulated and downregulated gene expression was different based on disease activity but not significantly different between EoE or EI in either state.
My take (borrowed from authors): The similar molecular transcriptome between EI and EoE are indicative of a shared pathogenesis.
Part A -In this phase 3 trial, we randomly assigned, in a 2:2:1:1 ratio, patients 1 to 11 years of age (n=102) with active eosinophilic esophagitis who had had no response to proton-pump inhibitors to 16 weeks of a higher-exposure or lower-exposure subcutaneous dupilumab regimen or to placebo (two groups)
Part B- At the end of Part A, eligible patients in each dupilumab group continued the same regimen and those in the placebo groups were assigned to higher-exposure or lower-exposure dupilumab for 36 weeks
Key findings:
In Part A, histologic remission occurred in 25 of the 37 patients (68%) in the higher-exposure group, in 18 of the 31 patients (58%) in the lower-exposure group, and in 1 of the 34 patients (3%) in the placebo group
The higher-exposure dupilumab regimen led to significant improvements in histologic, endoscopic, and transcriptomic measures as compared with placebo
The improvements in histologic, endoscopic, and transcriptomic measures between baseline and week 52 in all the patients were generally similar to the improvements between baseline and week 16 in the patients who received dupilumab in Part A
Similar adverse effects were noted across all groups. There was an increased rate (at least 10%) of COVID infections in participants receiving dupilumab whereas the incidence of vomiting was at least 10 percentage points lower among patients who received dupilumab (either group) than among those who received placebo
My take: Dupilumab is an effective option for eosinophilic esophagitis.
In this 10-year retrospective review (2013-2023), the authors reviewed children with EoE referred for high-resolution impedance manometry (HRIM) due to persistent dysphagia despite histologic healing (i.e., <15 Eos/hpf).
Key findings:
Among a cohort of ~1500 children, only 4 patients met inclusion criteria: histologic remission (<15 eos/hpf) and absence of fibrostenotic features on endoscopic evaluation
Thus, the estimated prevalence of post-remission dysphagia in this cohort was exceedingly rare (<0.05%).
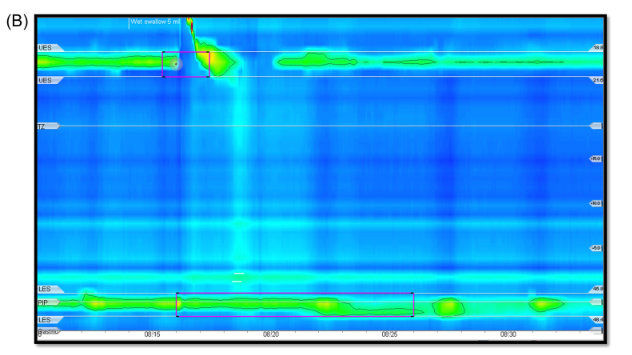
On HRIM, all four patients had a hypomotile esophagus and abnormal bolus clearance. Lower esophageal sphincter integrated relaxation pressure values were normal in three patients and elevated in one. Two patients were diagnosed with ineffective esophageal motility, one with aperistalsis and one with achalasia type 1.
Manometry findings from 12 yo diagnosed with Achalasia Type 1
Discussion:
“Endoscopic evaluation of fibrosis is somewhat limited as less than 50% of biopsies contain an adequate sample of the lamina propria for evaluation..[Also, these] patients did not undergo endoluminal functional lumen imaging (Endoflip) which has been recently shown to correlate with fibrotic changes of the esophagus in pediatric patients…Nonetheless, this case series highlights the fact that esophageal dysmotility can persist, even in the absence of endoscopic or histologic findings”
The authors “did not study all EoE patients treated in our facility who had persistent dysphagia despite histologic remission of EoE, but rather explored just those who were referred for manometry. This methodology creates a risk of referral bias.”
My take: Though there is a referral bias due to the methodology, this study suggests that persistent dysphagia is rare in children who achieve EoE histologic remission. In addition, in those with significant dysphagia despite improvement in EoE, manometry is worthwhile.
This study of 171 adult patients (mean age 38 years) who had FLIP at time of an EGD determined the degree of esophageal distensibility and its association with eosinophilic esophagitis disease duration.
Key findings:
The median symptom duration was 8 (interquartile range, 3–15) years and diagnostic delay was 4 (interquartile range, 1–12) years
Symptom duration and diagnostic delay were negatively correlated with distensibility plateau (DP) (rho = –0.326 and –0.309; P values < .001)
Abnormal esophageal distensibility (DP ≤17 mm) was more prevalent with increased duration of symptoms (P < .004): 23% at <5 years to 64% at ≥25 years
Patients with ≥15 eos/hpf had significantly lower DP with greater symptom duration (P = .004), while there was not a significant difference among patients with <15 eos/hpf (P = .060).
My take: Longer duration of disease increases the risk of esophageal fibrosis and lack of distensibility. We need better tools to predict who is at most risk for developing fibrosis.
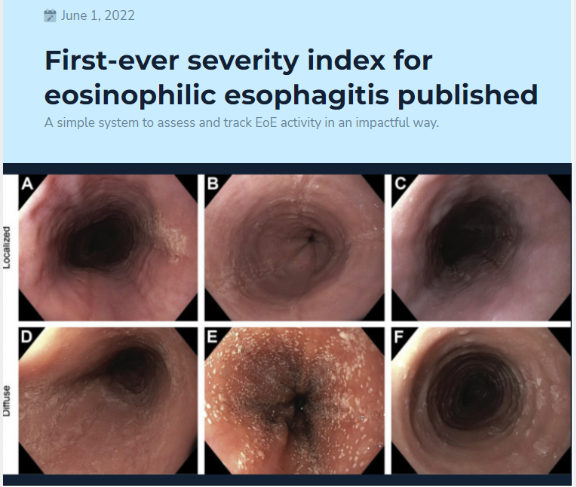
This was a retrospective analysis on a prospectively enrolled cohort of children at a single center who were treated as part of routine clinical care. I-SEE was calculated at the diagnostic and follow-up endoscopies over a mean of 6.6 years.
Key findings:
Of 67 children who met study criteria of at least 3 endoscopies over at least 2 years of follow-up time, 43%, 36%, and 21% had mild, moderate, and severe I-SEE scores at baseline, respectively.
By the last instance, the overall I-SEE score dropped to 3.9 (P < .001). Body mass index <5% and poor feeding were more common in the children with severe I-SEE scores at baseline, and both improved by the last instance.
The discussion notes that I-SEE metric was developed to determine EoE severity and for tracking purposes to gauge effectiveness of therapy. They note that most patients improved but a score of 0, indicating deep remission, was difficult to achieve at the population level. They also anticipate further modifications to I-SEE “such as age or an assessment of symptoms that reflects inflammatory or fibrotic disease.”
My take: I-SEE provides a way to objectively assess and follow EoE severity at all ages.
The summary with nine “best practice advice” statements is not very helpful. However, Figure 2 and Table 1 are very useful.
From Figure 2 -not shown below (but in article) are Prague classification for Barrett’s and EREFS for eosinophilic esophagitis. The remaining parts of this figure include the Los Angeles classification for erosive esophagitis, the Hill classification of the gastroesophageal flap, and the Forrest classification of peptic ulcers:
From Table 1:
Table 1 also gives guidance for biopsies with peptic ulcer disease, Barrett’s esophagus, gastric preneoplasia, and for gastric polyps.
My take: When suspicious of underlying disease, this article recommends taking more biopsies and in more jars.
Best Approach for Identifying Eosinophilic Esophagitis Prior studies have shown higher yield when taking 5 or 6 biopsies rather than fewer biopsies; thus, the location of biopsies may not be as important as the number of specimens. Also, prior studies have shown that having another pathologist review the slides can increase the yield by ~20%; this indicates that careful review of specimens by itself is helpful. Perhaps, more specimen containers will increase the time that a pathologist reviews the biopsies.