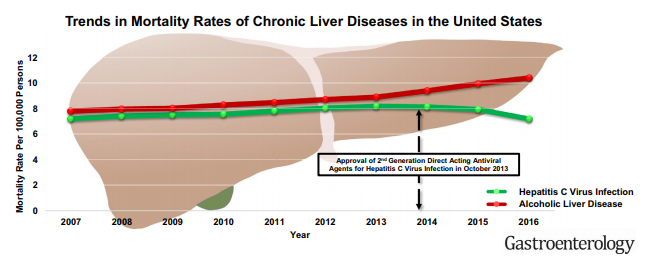
A recent study (D Kim et al. Gastroenterol 2018; 155: 1154-63) used a CDC database which captures >99% of deaths in the U.S. to analyze mortality trends from 2007 through 2016. Full text link available online: Changing Trends in Etiology-Based Annual Liver Mortality
When looking at all-cause mortality, there has been a significant decline in deaths associated with hepatitis C (HCV) but not in deaths associated with alcoholic liver disease (ALD). The image below shows the trend and the impact of direct-acting antivirals. Deaths associated with nonalcholic fatty liver disease (NAFLD) and due to hepatitis B (HBV) are described in this study as well, though both together account for less than 1/4th deaths associated with ALD. Interestingly, mortality related to NAFLD was increasing slowly over the study period.

Related blog posts:
- Direct-acting Antivirals in Patients without Advanced Hep C Liver Disease
- Word of Caution with New Hepatitis C Medications
- Hepatitis C Reactivation with Chemotherapy
- The Dark Cloud Inside the Silver Lining -What’s Really Going on with Hepatitis C Infection | gutsandgrowth
- Heroin Epidemic Causing Surge in HCV
- HCV now more deadly than HIV | gutsandgrowth
- Updated HCV Guidelines Published | gutsandgrowth