
A couple good review articles (though behind paywall):
PT Reeves, L James-Davis, M Khan. Neoreviews 2023;24(7):e403-e413. Gastrointestinal Bleeding in the Neonate: Updates on Diagnostics, Therapeutics, and Management This reviews covers the most important etiologies of GI bleeding in the neonate. A few interesting points were the potential use of calprotectin as a potential screen for necrotizing enterocolitis; “the median fecal calprotectin levels in infants with NEC were between 210 and 400 mg/g of stool.” The authors also point out that there is “limited evidence for performing endoscopy in infants with GIB…][In one study] Only 3 of 56 infants underwent therepeutic intervention during endoscopy. Five percent (n=3) of these neonates exhibited gastrointestinal perforation in the acute postoperative period after endoscopy.”
Related blog posts:
- Therapeutic Endoscopy Rarely Beneficial in Infants with Gastrointestinal Bleeding
- Timing of Upper Endoscopy with GI Bleeding -Is It Safer to Wait a Bit?
- GI Bleeding -Forrest Classification
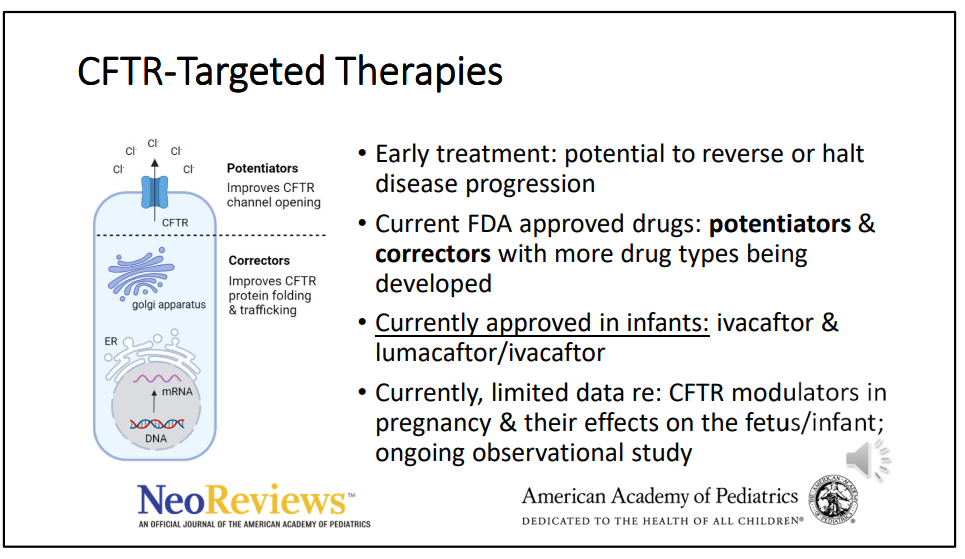
JT Duong, ZM Sellers. Neoreviews (2023) 24 (7): e414–e430. Cystic Fibrosis-Associated Gastrointestinal Disease in Neonates
Associated slides (13 slides) and presentation (~7 minutes ): Cystic Fibrosis-Associated Gastrointestinal Disease in Neonates






The actual article has many other useful points. For example:
- CFTR is not expressed in hepatocytes; “however, liver injury may occur patients with CF due to proximity to cholangiocytes (which may be inflamed) and/or through increased intestinal permeability.”
- Elastase levels are not affected by exogenous pancreatic enzyme supplementation and is expected to display levels within the normal adult range by 2 weeks of age.
- Sodium deficiency is common and needs to be prevented with sodium supplementation in first 12 months of life (one-eighth teaspoon (= 12.5 mEq) of salt in first 6 months, and one-fourth teaspoon (=25.2 mEq) from 6-12 months)
- The newest CFTR modulator, elexacaftor/tezacaftor/ivacaftor is approved for children 2 years of age and older
- There are case reports of in utero exposure to CFTR modulators associated with resolution/prevention of disease (eg. pregnant women starting CFTR-targeted treatment at 32 weeks gestation which resolved meconium ileus).
Related blog posts:
- Inconclusive Screening for Cystic Fibrosis and Outcomes
- Aspen Webinar 2021 Part 7 -Cystic Fibrosis Liver Disease
- CHOA Nutrition Support Lecture: Cystic Fibrosis Nutrition -Changing in the Age of ‘Miracle Drug’
- Data on Immobilized Lipase Cartridge for Patients with Cystic Fibrosis
K McNelis, ME Rogers, S Kocoshis. Neoreviews. 2023 Jul 1;24(7):e431-e439. Pediatric Intestinal Transplantation Management and Outcomes This is another useful review for pediatricians. Pediatric intestinal transplantation is most commonly (65%) related to short bowel syndrome, 20% due to motility disorders, 9% due to mucosal diseases, 5% due to retransplantation and 1% are due to a variety of causes. The evaluation and management of patients needing intestinal transplantation is succinctly summarized. “Overall, survival of pediatric patients after intestinal transplantation is 72.7% at 1 year and 57.2% at 5 years. The most common causes of death are sepsis/multiorgan system failure and cardiovascular/stroke (Fig 2).” Also, “current statistics about organ transplantation can be publicly accessed by health care team members, patients, and families at srtr.transplant.
hrsa.gov.” This site also includes data on transplantation for kidney, pancreas, heart, lung and liver.
Related blog posts:
- Surviving Pediatric Intestinal Transplantation
- Thrombosis in Pediatric Patients with Intestinal Failure
- Predicting Intestinal Failure After Gastroschisis Repair
- Nutritional Management of Intestinal Failure in Pediatrics
- #NASPGHAN19 Intestinal Failure Session Part 2
- #NASPGHAN19 Intestinal Failure Session Part 1


