Briefly noted from Twitter:
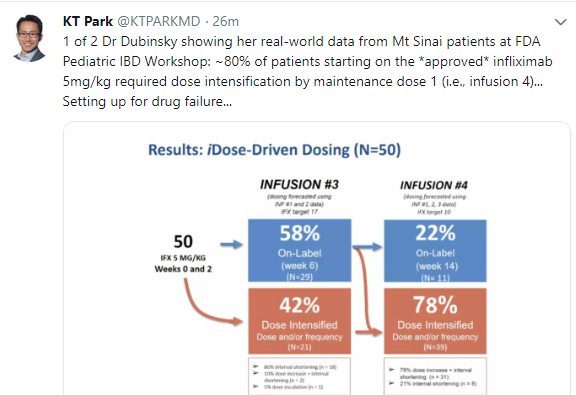
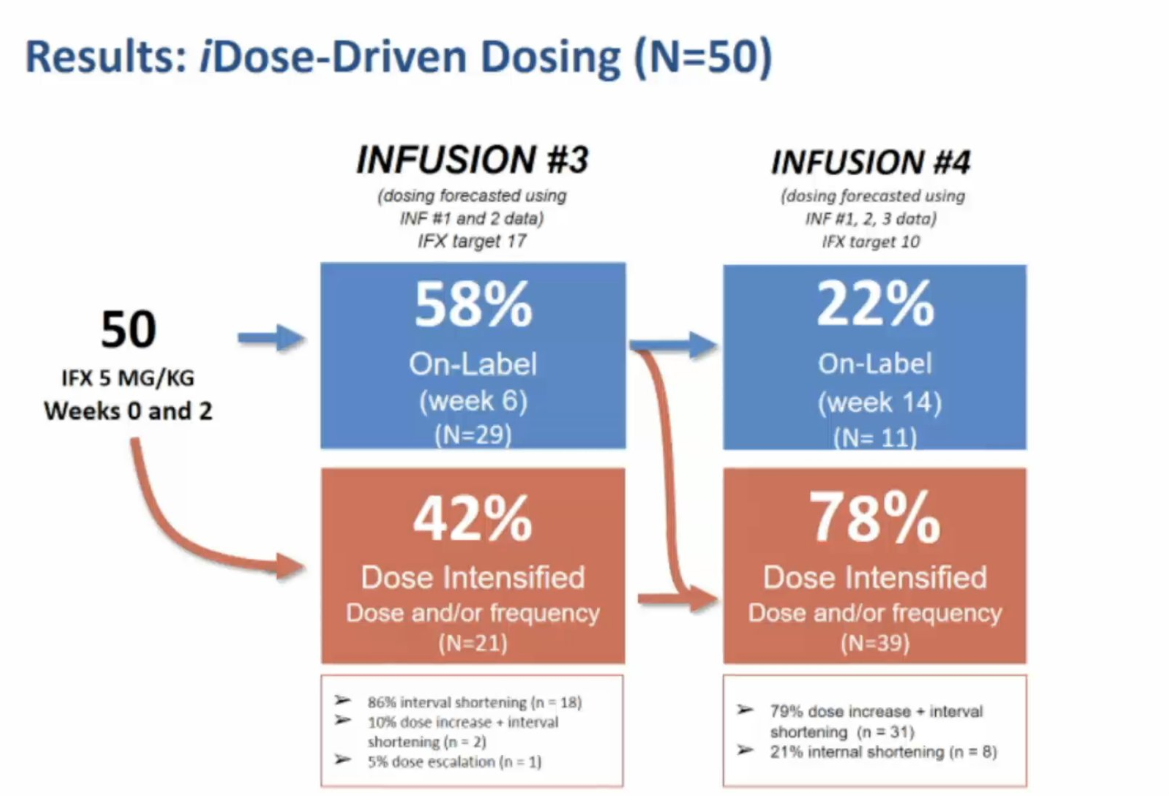
Close up of previous image
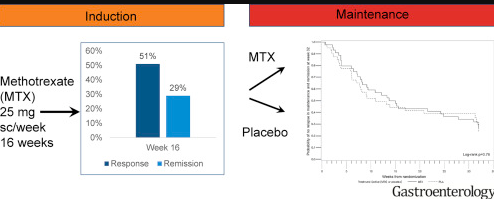
Also –with regard to Methotrexate:


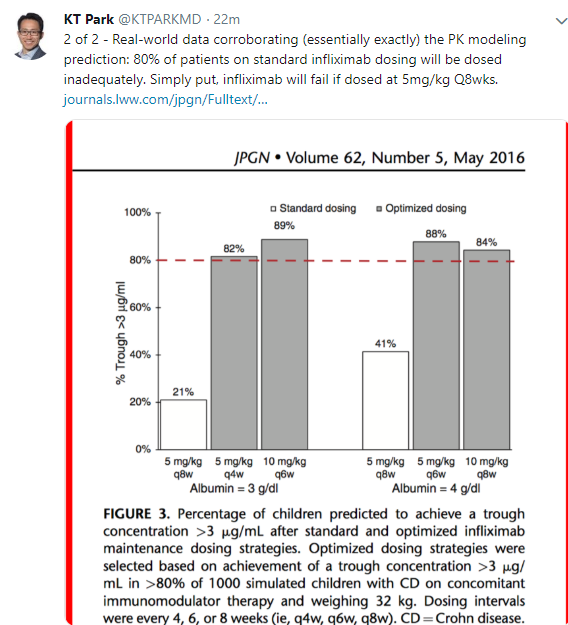
Briefly noted from Twitter:
Close up of previous image
Also –with regard to Methotrexate:
A recent study (H Hansfarth et al. Gastroenterol 2018; 155: 1098-1108) examined the use of methotrexate for ulcerative colitis (UC). The authors performed a 48-week trial (MERIT-UC trial) with 179 patients with a mean age of 42 years in the induction period. In those who improved during induction, methotrexate was continued in 44 patients and compared to 40 patients who received placebo; this was a double-blind, placebo-controlled trial.
Key findings:
The associated editorial by Dulai (pg 967-69) which reviewed this study and a prior study (METEOR) comes to the conclusion that: “there is likely no place for methotrexate monotherapy in UC.”
Related blog posts:
C Ma et al. Clin Gastroenterol Hepaatol 2018; 16: 1407-19. This study examined endpoints in randomized controlled trials (RCTs) of Crohn’s disease. Key finding: Among 116 included RCTs (n=27,263 patients), there were 38 unique definitions of clinical response or remission and 32 definitions of loss of response. The most common endpoint was CD activity index.
RP Hirten et al. Clin Gastroenterol Hepatol 2018; 16: 1374-84. This review examines the topic of combining biologics in inflammatory bowel disease. Currently, there is little data in IBD. From studies completed in rheumatology and dermatology, there are some safety concerns. One current study, the EXPLORER study, which is a phase 4 open label trial evaluating the use of vedolizumab in combination with adalimumab and methotrexate, will provide some useful information. With regard to safety, gut-specific anti-integrin therapies are likely to be safer in combination than other biologic therapies.
RJ Colman et al. Inflamm Bowel Dis 2018; 24: 2135-41. This systematic review and meta-analysis which included 14 eligible studies showed that the pooled clinical remission rate with methotrexate monotherapy for pediatric Crohn’s disease was 57.7% at 3-6 months and 37.1% at 1 year.
AA Wren et al. Inflamm Bowel Dis 2018; 24: 2093-2105. This study with 93,668 patients in a cohort from Truven MarketScan Database (2007-2015) identified a high rate of opioid therapy usage in U.S. adolescents and young adults (15-29 year olds). Annual prevalence of chronic opioid use was 9.3% in 2007 and peaked at 12.2% in 2011. In 2015, the prevalence dropped to 10.8%. Overall, 18.2% had received chronic opioid therapy. Among the 2503 with chronic opioid usage who were followed longitudinally, 30.5% received opioids for 2 years and 5.3% for 4 years. The associated editorial (ME Kuenzig, EI Benchimol, pg 2140-5) note that these prevalence data may underestimate the true rate of opioid use due to the case definition of IBD used when analyzing the administrative data.

Lake Moraine, Banff
This blog entry has abbreviated/summarized this terrific presentation; most of the material has been covered in this blog in prior entries but still this was a useful review. Though not intentional, some important material is likely to have been omitted; in addition, transcription errors are possible as well.
2nd Lecture: What is Next in Treatments for Pediatric Patients? –Dr. Michael Rosen
I really enjoyed meeting Dr. Rosen. He is super-friendly and knowledgeable.
Combination therapy. Grossi V et al showed improvement in infliximab durability with concomitant therapy.



Now starting COMBINE trial (ImproveCareNow)–randomized to low dose MTX or placebo in combination with anti-TNF agent.

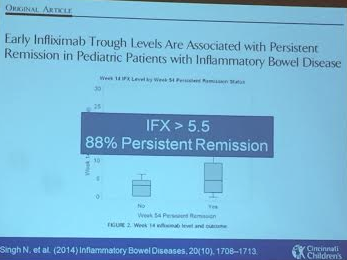
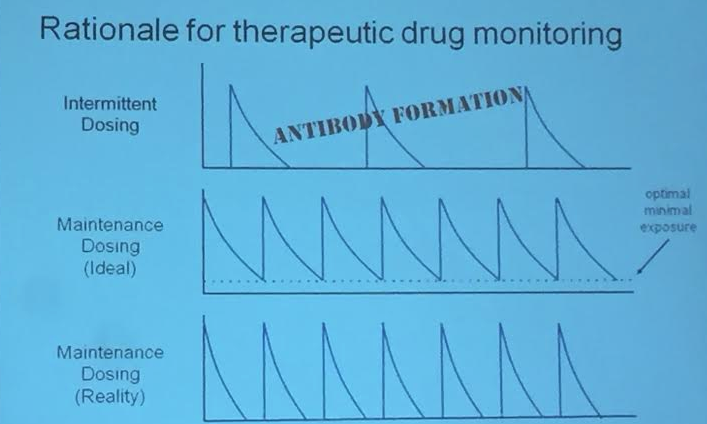
Therapeutic drug monitoring in pediatrics. Is this an alternative to combination therapy? Rationale (see slide): lower antibody formation if trough levels maintained. IFX level >5.5 associated with persistent remission (Singh et al 2014). Children are growing and they may need more adjustments. In Cincy, checking levels at week 14 after initiation and then every 6-12 months.
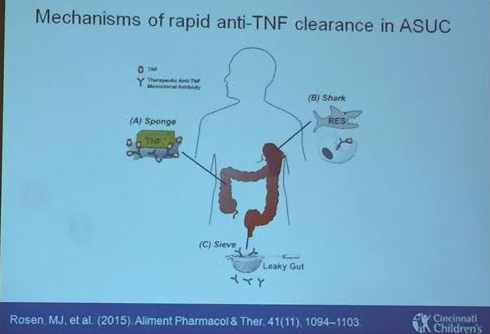
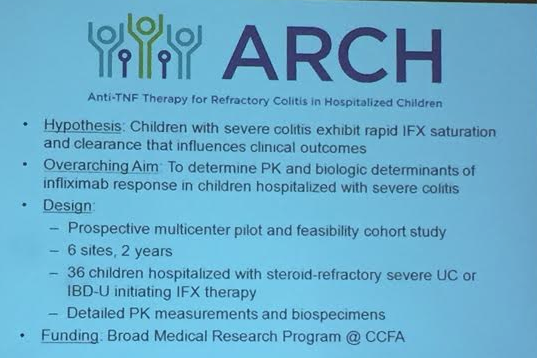
Acute Severe Ulcerative Colitis. High rates of dose escalation in this population. Some of this is due to more rapid clearance of anti-TNF –leaking in gut and other mechanisms as well. Week 8 level of 40 associated with clinical response. Thus, this population may benefit from 10 mg/kg at start (in those with albumin <3) and may need more frequent dosing, especially early into treatment (?0, 2, 6, 10). ARCH study to look into this further
Vedolizumab. Conrad MA 2015. About 1/3rd of these refractory patients in this abstract responded.

Ustekinumab . IL-12 & IL-23 blockage. No studies in pediatrics. Case report reviewed of good response in a refractory case.
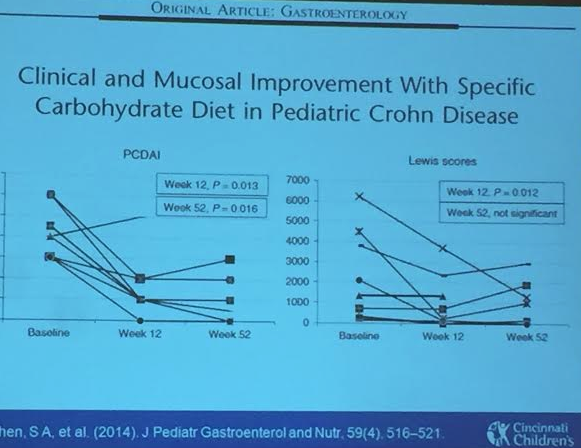
Enteral therapy. Specific carbohydrate diet experience. These diets have some published data, most retrospective studies. Our group (Cohen SA et al) did perform a small prospective study. Sigall-Boneh R et al showed improvement with partial enteral nutrition.




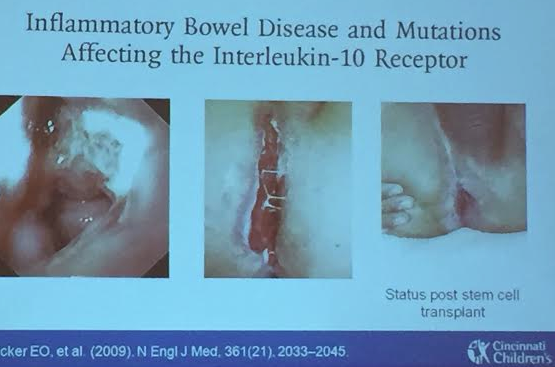
Very early-onset of IBD. IL-10 receptor deficiency was a key early discovery and can be treated with stem cell transplant. STAT3 mutation case reviewed which was managed with tocilizumab. More targeted therapy expected based on specific mutations.
A recent study (F Carbonnel et al. Gastroenterol http://dx.doi.org/10.1053/j.gastro.2015.10.050, article in press; thanks to KT Park twitter feed for reference) with 111 patients provides more questions than answers. It appears that methotrexate improved clinical remission but the overall difference is fairly small; the abstract is below.
My initial impression: Immunomodulators (including methotrexate and thiopurines) have some efficacy as monotherapy agents in patients with inflammatory bowel disease. Their role as part of combination therapy (with anti-TNF agents) has been associated with improved outcomes but how long to use combination therapy and at what dosage is still being worked out.
Here’s the abstract and a link: Methotrexate is not Superior to Placebo in Inducing Steroid-free Remission, but Induces Steroid-free Clinical Remission in a Larger Proportion of Patients with Ulcerative Colitis
Parenteral methotrexate is an effective treatment for patients with Crohn’s disease but has never been adequately evaluated in patients with ulcerative colitis (UC). We conducted a randomized controlled trial to determine its safety and efficacy in patients with steroid-dependent UC.
We performed a double-blind, placebo-controlled trial to evaluate the efficacy of parenteral methotrexate (25 mg/week) in 111 patients with corticosteroid-dependent UC at 26 medical centers in Europe, from 2007 through 2013. Patients were given prednisone (10 to 40 mg/day) when the study began, and randomly assigned to groups (1:1) given placebo or methotrexate (intramuscularly or subcutaneously, 25 mg weekly) for 24 weeks. The primary endpoint was steroid-free remission (defined as a Mayo score ≤ 2 with no item > 1 and complete withdrawal of steroids) at week 16. Secondary endpoints included clinical remission (defined as a Mayo clinical subscore ≤ 2 with no item > 1) and endoscopic healing without steroids at weeks 16 and/or 24, remission without steroids at week 24, and remission at both weeks 16 and 24.
Steroid-free remission at week 16 was achieved by 19/60 patients given methotrexate (31.7%) and 10/51 patients given placebo (19.6%)—a difference of 12.1% (95% confidence interval [CI], –4.0% to 28.1%; P=.15). The proportions of patients in steroid-free clinical remission at week 16 were 41.7% in the methotrexate group and 23.5% in the placebo group, for a difference of 18.1% (95% CI, 1.1%–35.2%; P=.04). The proportions of patients with steroid-free endoscopic healing at week 16 were 35% in the methotrexate group and 25.5% in the placebo group—a difference of 9.5% (95% CI, –7.5% to 26.5%; P=.28). No differences were observed in other secondary endpoints. More patients receiving placebo discontinued the study because of adverse events (47.1%), mostly caused by UC, than patients receiving methotrexate (26.7%; P=.03). A higher proportion of patients in the methotrexate group had nausea and vomiting (21.7%) than in the placebo group (3.9%; P=.006).
In a randomized controlled trial, parenteral methotrexate was not superior to placebo for induction of steroid-free remission in patients with UC. However, methotrexate induced clinical remission without steroids in a significantly larger percentage of patients, resulting in fewer withdrawals from therapy due to active UC.
Related blog posts:

Banning Mills
Among patients/families who are not in denial about their inflammatory bowel disease, especially Crohn’s disease, an important discussion is the use of combination therapy. This has been discussed on this blog before (see some links below). More data on this subject has been published and again favors the use of combination therapy (V Grossi, T Lerer, et al. Clin Gastroenterol Hepatol 2015; 13: 1748-56).
This study collected data from 2002-2014 on 502 children who participated in a prospective multicenter study. This data was derived from an observational registry rather than a randomized trial, but likely reflects real-world experience with regard to newly diagnosed patients. The authors excluded those with prior biologic therapy and prior resectional surgery.
KEY FINDINGS:
Among patients who stopped IFX, the reasons included loss of response (n=61, 43%), hypersensitivity reaction (n=41, 29%), elective (n=25, 18%), lost to f/u (n=5, 3%), and other causes (10, 7%).
The “right” dose of methotrexate as a combination agent remains unclear. There was a wide range of dosing schedules in this study. It is worth observing that the COMMIT study in adults found no significant difference in adults who received methotrexate in addition to infliximab compared with those receiving infliximab monotherapy.
Take-home message: In this large pediatric observational study, the use of immunomodulators increased the likely durability of infliximab. Given prior conflicting data (particularly with regard to methotrexate), even more studies are needed to determine exactly how useful combination therapy is and when monotherapy will suffice. From my viewpoint, I worry much more about loss of efficacy to infliximab than I worry about medication adverse effects. As such, I will continue to inform families that combination therapy appears to improve infliximab durability.
Related blog posts:
Mount Washburn, Yellowstone
A group of 23 experts followed a rigorous process over a 1-year period to assess the quality of evidence and develop consensus statements regarding the medical management of ulcerative colitis (UC) in adults (Bressler B, Marshall JK et al. Gastroenterol 2015; 148: 1035-58, editorial 877-80).
The need for updated guidelines has emerged due to practice variation related in part to a wider availability of treatments and diagnostic tools. It is recognized that early institution of effective therapy is associated with the best outcomes. In addition, due to the chronic nature of ulcerative colitis and the potential for reduced durability of biologic agents, careful decision-making can improve response.
Table 4 in the article summarizes the recommendations. I will list a few:
1. Thiopurines:
2. Anti-TNF therapy:
3. Vedolizumab
4. Fecal microbial transplant (FMT)
5. 5-ASA and Corticosteroids
With all of the treatments, the authors recommend followup to assure response to therapy; this followup ranges from within 2 weeks for steroids, to 4-8 weeks with 5-ASA products, to 8-14 weeks for biologic agents.
Overall, the emphasis of this consensus statement is on maximizing the response to biologic agents. By optimizing dosing and using combination therapy, the treatment guidelines aim to lower rates of antidrug antibody formation. This in turn should improve results and is in agreement with data from both the SONIC study and the UC-SUCCESS study.
The editorial comments that methotrexate “may be an attractive option for young male patients;” however, “the absence of data on risk of malignancy with methotrexate in IBD may reflect lower frequency of use for this indication.”
While these guidelines will be useful, there are many unanswered questions (discussed in editorial).
Bottomline: These guidelines are likely to promote the use of more combination therapy and help define the current role of vedolizumab.
Related blog posts:
Disclaimer: These blog posts are for educational purposes only. Specific dosing of medications/diets (along with potential adverse effects) should be confirmed by prescribing physician/nutritionist. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
“The addition of immunomodulators increases the efficacy of maintenance therapy with infliximab for up to one year in patients with Crohn’s disease who have not been previously treated with immunomodulators. However, there are questions about the effect of withdrawing immunomodulator therapy from these patients. David Drobne and colleagues studied the effects of treatment with infliximab and immunomodulators (co-treatment) and then immunomodulator withdrawal on long-term outcomes of patients, as well as trough levels of infliximab and formation of anti-infliximab antibodies (ATI). Reporting in Clinical Gastroenterology and Hepatology, they find that, in a retrospective analysis, withdrawal of immunomodulators after at least six months (median, 13 months) of co-treatment with infliximab does not reduce the trough levels of infliximab in patients with Crohn’s disease. Detectable trough levels of infliximab at the time of immunomodulator withdrawal are associated with long-term response.”
Clinical Gastroenterology and Hepatology 2015: 13(3): 514-521.e4
Some additional details:
This was a retrospective open-label cohort study with 223 patients and median followup of 34 months. At baseline, 65 received infliximab (IFX) monotherapy and 158 received co-therapy with an immunomodulator (46 methotrexate, 112 thiopurine). Immunomodulators were withdrawn “only in patients with durable response (ongoing clinical benefit with lasting disease control with low C-reactive protein [CRP] [below 10 mg/L]).” Among the 158 on co-therapy, 117 reached a durable response and had withdrawal of immunomodulator after >6 months of combination therapy (median time 13 months).
Key findings:
Though the headlines covering this article have suggested that IFX levels will stay stable when immunomodulators are withdrawn after >6 months, the authors proposed algorithm only recommends withdrawal for those with IFX trough level >5 mcg/mL. In addition, the data showed that a large number of patients required dose escalation and/or lost detectable IFX levels. Despite their proposed algorithm to withdraw in this small group, the authors further backtrack in their conclusion: “a prospective parallel group trial during a period of 5-10 years in a large group of patients is required to ascertain the real long-term benefit to risk ratio of continuing combined infliximab and immunomodulator treatment.”
Bottomline: If a patient is doing well, withdrawing immunomodulator co-therapy still has risks. I worry that the misleading reporting of this article will result in detrimental outcomes.
Related blog posts:
Disclaimer: These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
A recent retrospective study (DOI: http://dx.doi.org/10.1093/ecco-jcc/jjv027 first published online: 23 January 2015 -reference from KT Park’s twitter feed) has suggested that high-dose methotrexate (MTX) (15-25 mg/week) is more effective than low-dose MTX (≤12.5 mg/week) as part of dual therapy for inflammatory bowel disease.
Here’s the abstract: Optimal Doses of Methotrexate
Background and Aims: Methotrexate is sometimes used as part of combination therapy for the treatment of inflammatory bowel disease (IBD), however the optimal MTX dose for combination therapy has not been established. This study compared the efficacy of lower dose and higher dose methotrexate with anti-TNF therapy among IBD patients.
Methods: Retrospective chart review was performed of 88 IBD patients at our center between 2010-2013. Low-dose methotrexate was defined as ≤ 12.5mg/week and high-dose methotrexate as 15-25mg/week. Patients who met the criteria for clinical remission (Harvey-Bradshaw Index ≤ 4, Simple Clinical Colitis Activity Index ≤ 2) at baseline were followed for up to 42 months. Chart review occurred in six-month intervals. The primary outcome was consecutive months in remission prior to relapse. Secondary outcomes included other indicators of worsening disease (endoscopic inflammation, steroid use, therapy escalation/addition, or surgery) and adverse events. Regression analysis and Kaplan-Meier survival analysis were completed.
Results: We identified 73 (83%) dual-therapy patients, of which 32 low-dose and 14 high-dose individuals achieved remission. When compared with high-dose patients, low-dose patients were more likely to relapse (log-rank test, P<0.01). Secondary indicators of worsening disease occurred during 34.4% of low-dose review periods and 31.4% of High-dose review periods (P=0.67). 3/52 (6%) low-dose patients and 3/21 (14%) high-dose patients (P=0.34) discontinued methotrexate therapy due to adverse events.
Conclusions: When combined with anti-TNF therapy, methotrexate at doses of >12.5mg/week were more effective at maintaining clinical remission than lower doses. These findings will guide management of combination therapy in IBD patients.
Related blog posts:
A useful review on the hepatobiliary manifestations of inflammatory bowel disease (IBD): Inflamm Bowel Dis 2014; 1655-67.
A few topics/comments from review:
Primary sclerosing cholangitis (PSC):
Cholelithiasis: Gallstones are reported in 13% to 24% of all patients with CD. In UC, the risk of cholelithiasis “does not seem to be increased.”
Drug-induced liver disease: (see liver tox website)
Viral hepatitis in immunosuppressed IBD patients:
Hepatitis B reactivation -algorithm for screening/management of latent hepatitis B provided in Figure 3
Other liver problems seen in IBD patients:
Related blog posts:
