MY Yousif et al. JPGN 2024; 79:1009–1016. Open Access! The association between erythema nodosum and pyoderma gangrenosum and pediatric inflammatory bowel disease
Using the ImproveCareNow prospective registry, the authors analyzed a total of 285,913 visits from 32,497 patients aged ≤ 21 years.
Key findings:
- The occurrence of erythema nodousm (EN) was 1.57% and the occurrence of pyoderma gangrenosum (PG) was 0.90%. Co-occurrence of EN and PG was reported in 0.30% patients.
- Both EN and PG were associated (p < 0.0001) with worse intestinal disease, lower remission, higher inflammatory markers, and extraintestinal manifestations (EIMs) arthritis and uveitis.
- Limitations: “imperfect and incomplete data entry that may introduce bias. However, due to the extensive longitudinal data, we expect any bias to be minimal.”
My take: This study clarifies how common these dermatologic findings occur in pediatric patients with IBD. Prompt recognition of these disorders is important. Recently, our group cared for a 20 yo patient with inadequately-treated PG by multiple internal medicine physicians; this led to prolonged hospitalization.
Related blog posts:
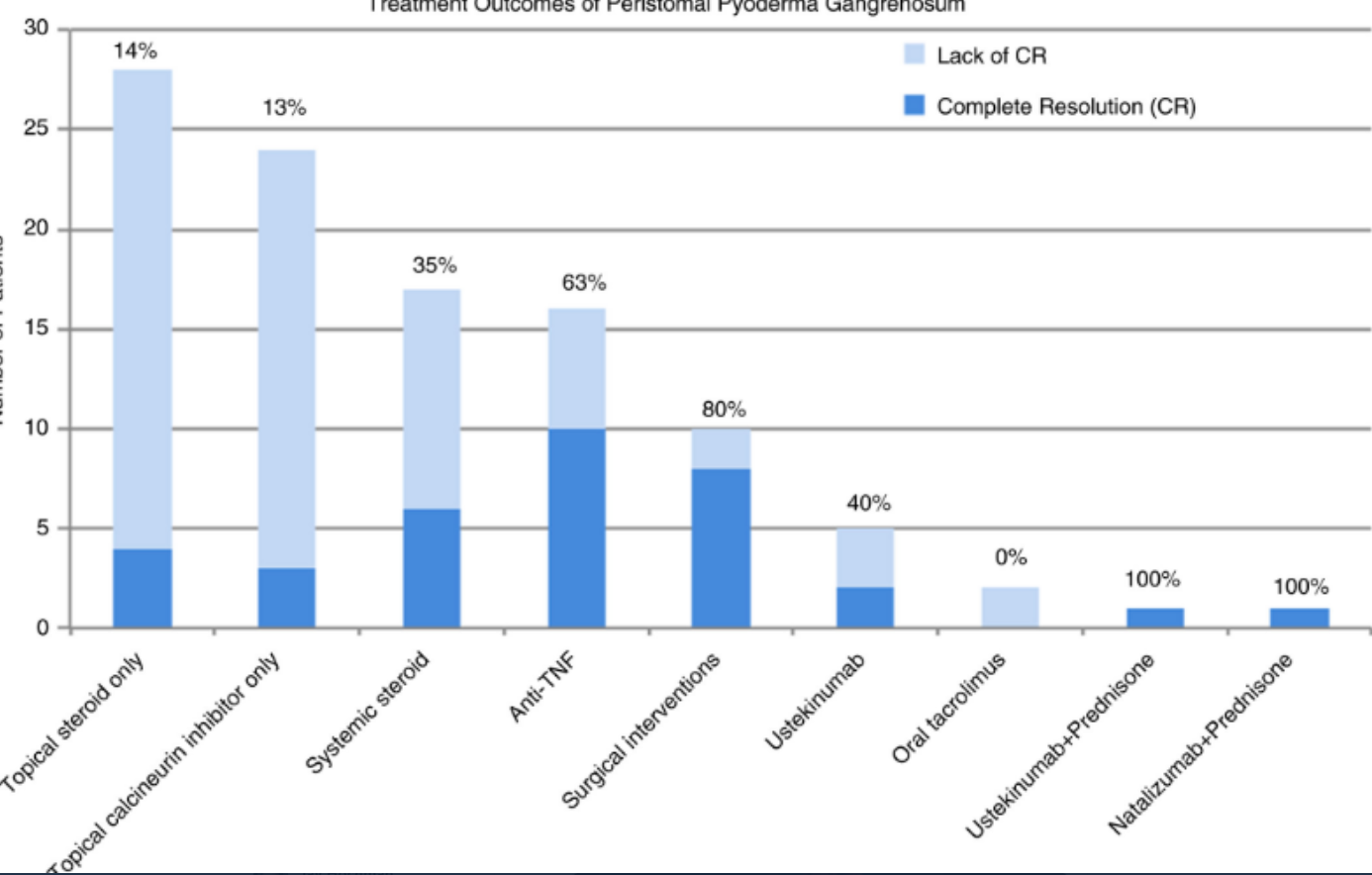
- Image Only: Pyoderma Gangrenosum
- Review of Pyoderma Gangrenosum
- Tofacitinib Case Reports for Acute Severe UC and Pyoderma Gangrenosum
- IBD Updates: Fatigue Trajectory, Risk of IBD with Derm Findings
- Ustekinumab Efficacy in Crohn’s Disease With Concurrent Autoimmune Skin Disease
- IBD and Immune-Mediated Diseases