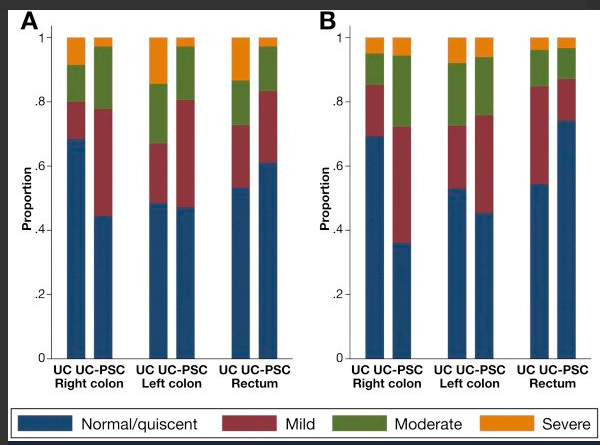
A recent retrospective study (Clin Gastroenterol Hepatol 2018; 16: 68-74) compared adult patients who had ulcerative colitis (UC) with (n=23) and without primary sclerosing cholangitis (n=120) (PSC). All patients had pancolitis and were in clinical remission.
Key finding:
- Patients with UC-PSC had more subclinical endoscopic activity (odds ratio (OR) 4.21) and histologic activity (OR 5.13) in the right colon compared with patients without PSC
It is known that the presence of PSC is a risk factor for colorectal cancer (CRC). A previous meta-analysis (RM Soetiknno et al. Gastrointest Endosc 2002; 56: 48-54) described a OR of CRC of 4.09.
My take: This study shows that UC patients with PSC who are in clinical remission have a greater degree of endoscopic and histologic inflammation in the proximal colon compared to patients without PSC. This increased inflammation is a likely factor in the increased risk for CRC.
Related blog posts:
- Annual Meeting #NASPGHAN17: PSC
- #NASPGHAN17 PSC-IBD: Fellow Research Award: Symptoms Underestimate Endoscopic Activity in PSC-IBD. Amanda Ricciuto et al. Hospital for Sick Children
- Big Pediatric PSC Study
- Should we care about subclinical PSC? (This post has links to others related to PSC)
- PSC -Natural History Study (pediatric)
- Primary Sclerosing Cholangitis (PSC) –Natural History Study