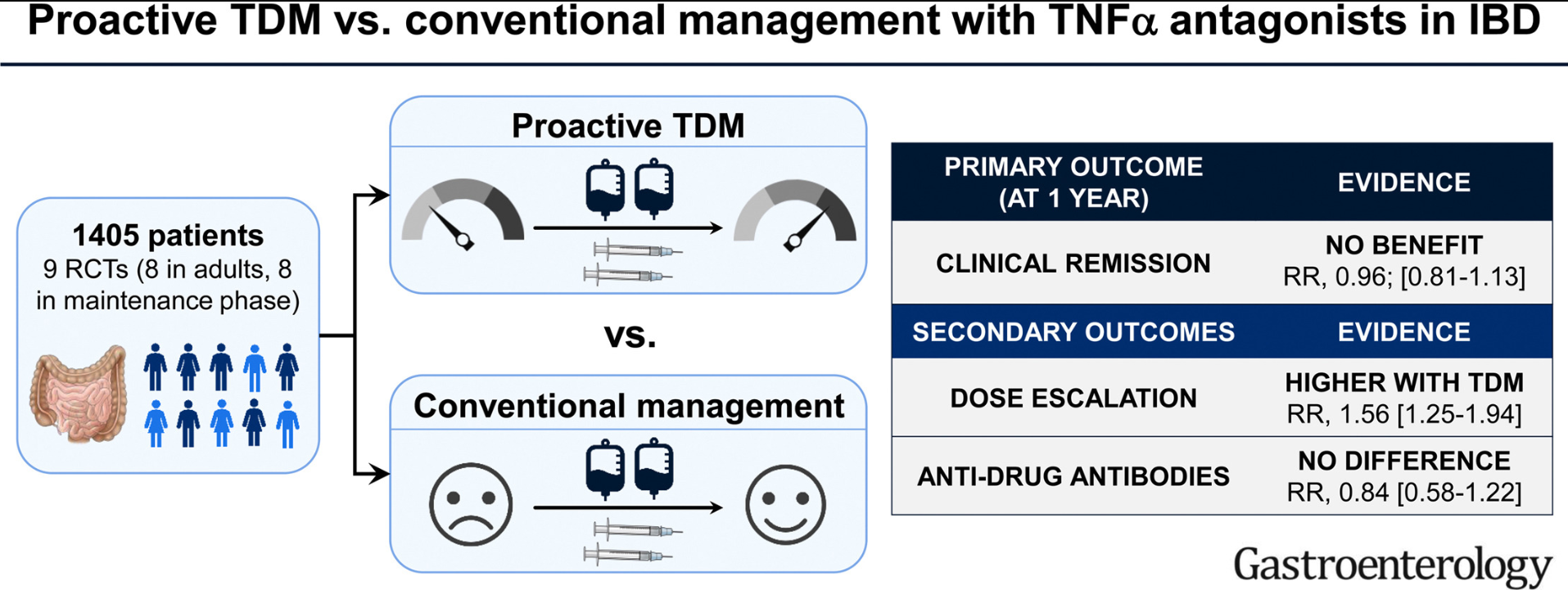
NH Nguyen et al. Gastroenterol 2022; 163: 937-949. Open Access! Proactive Therapeutic Drug Monitoring Versus Conventional Management for Inflammatory Bowel Diseases: A Systematic Review and Meta-Analysis
Key finding:
- On meta-analysis of 9 RCTs (8 RCTs in adults, and focusing on maintenance phase), there was no significant difference in the risk of failing to maintain clinical remission in patients who underwent proactive TDM (267/709; 38%) vs conventional management (292/696; 42%) (relative risk [RR], 0.96)
The discussion in this paper makes some important points, as there are some populations in which proactive TDM is more likely to be beneficial.
Pediatrics:
“The impact of proactive TDM in pediatric patients also merits further consideration. This concept may be particularly important in pediatrics due to the variability in size of patients, which may not be adequately addressed by weight-based dosing.33 This is especially important in younger children, where it has been shown that standard TNFα antagonist regimens and trough levels may not be applicable in this age group, and may require more frequent escalation of therapy.34,35 In the PAILOT trial, proactive TDM in children with clinical response to adalimumab was associated with higher rates of maintaining sustained corticosteroid-free clinical remission at all visits from week 8–72, compared with reactive TDM in which physicians were informed of trough concentration only after loss of response.”
Induction Dosing (Adults and Children):
“It is possible that the early measurement of biologic drug concentrations, to identify patients who may have accelerated clearance, and optimization of a subset of these patients early in the course of therapy may offer benefit.1,30 …Ongoing trials such as OPTIMIZE (NCT04835506) and TITRATE (NCT03937609) in which infliximab is optimized during the induction phase through a pharmacokinetic dashboard in patients with Crohn’s disease and acute severe ulcerative colitis will shed further light on this.”
My take: So far, studies in adults have not shown that proactive therapeutic drug monitoring has been effective in improving clinical outcomes. This may change particularly if studies focus on patients on monotherapy who are at increased risk of subtherapeutic levels. No matter what happens in adults, there is sufficient data showing that proactive therapeutic drug monitoring is essential in children. This is especially important as ‘routine” dosing of infliximab in children may be subtherapeutic in nearly 80%.
Related blog posts:
- Improving Outcomes with Proactive Therapeutic Drug Monitoring (JAMA 2021 study)
- Expert Consensus: New Recommendations for Therapeutic Drug Monitoring
- Can Therapeutic Drug Monitoring with Monotherapy Achieve Similar Results as Combination Therapy?
- Real-World Experience with Proactive Therapeutic Drug Monitoring in Inflammatory Bowel Disease
- Here’s The Proof That Proactive Drug Monitoring Improves Outcomes in Children With Crohn’s Disease
- Combination Therapy Study Points to Central Role of Adequate Drug Levels | gutsandgrowth
- Proactive Therapeutic Drug Monitoring -Different Time Points | gutsandgrowth
- For the Next Insurance Appeal: Therapeutic Drug Monitoring in Adalimumab Treatment (Pediatrics) & Satire on Prior Authorizations | gutsandgrowth