JF Gould et al. NEJM 2022; 387: 1579-1588. Neonatal Docosahexaenoic Acid in Preterm Infants and Intelligence at 5 Years
Background: “Because its accretion into the brain is greatest during the final trimester of pregnancy, infants born before 29 weeks’ gestation do not receive the normal supply of DHA.”
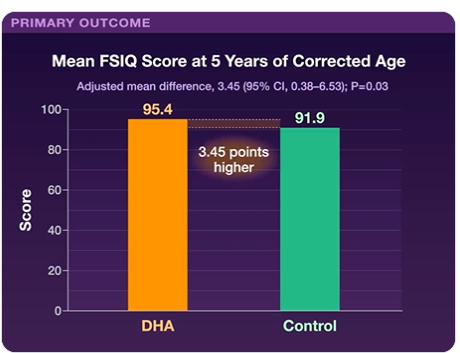
In this randomized placebo-controlled study of infants born prior to 29 weeks gestation, DHA supplementation 60 mg/kg/day was given to the study group and cognitive outcomes were measured at 5 yrs. 480 (73%) had an full-scale intelligence quotient (FSIQ) score available — 241 in the DHA group and 239 in the control group.
Key findings: FSIQ scores were 95.4±17.3 in the DHA group and 91.9±19.1 in the control group. Adverse events were similar in the two groups.
Key findings from this retrospective review (2011-2019):
Of 1801 cases of histologic colitis, 11 patients had CMV found by histology (mean age 15.4, 72.7% female), with an incidence of 0.6%
Nine out of these 11 (81.8%) patients were immunocompromised and 4 (36.4%) had inflammatory bowel disease (IBD) as an underlying diagnosis of whom 2 had new-onset ulcerative colitis
5 of 6 post-transplant patients with CMV colitis had preexisting CMV viremia
An independent analysis of 54 consecutive IBD-associated colectomy cases at TCH showed no histologic evidence of CMV
The study finding that half of the cases of CMV in the IBD population were identified prior to treatment indicates that the underlying IBD may be a more important susceptibility factor than the immunosuppressive medications.
My take: This study indicates that CMV colitis remains important in the post-transplant population but is rarely consequential in the pediatric IBD population.
IBD Updates -January 2017 With regard to CMV and IBD, this study showed “that in most cases the virus is nonpathogenic and thus antiviral is usually ineffective”
Little O’Malley Peak Trail, near Anchorage AK. Denali is visible in background, even though it is ~180 miles away.
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
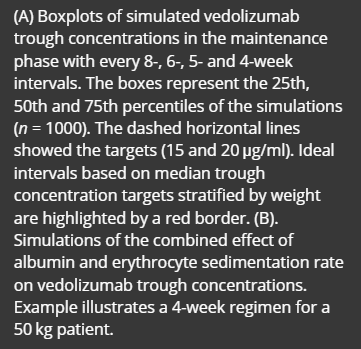
“The study included data from 463 observed vedolizumab concentrations (59 peaks and 404 troughs) from 74 patients with IBD (52 with Crohn’s disease and 22 with ulcerative colitis or unclassified IBD, median age 16 years)…This study was part of the multicentre REFINE study, which aimed to investigate paediatric PK factors among different biological therapies. Both induction and maintenance doses were between 6 and 10 mg/kg for patients less than 30 kg and 300 mg for patients above 30 kg.”
Key findings:
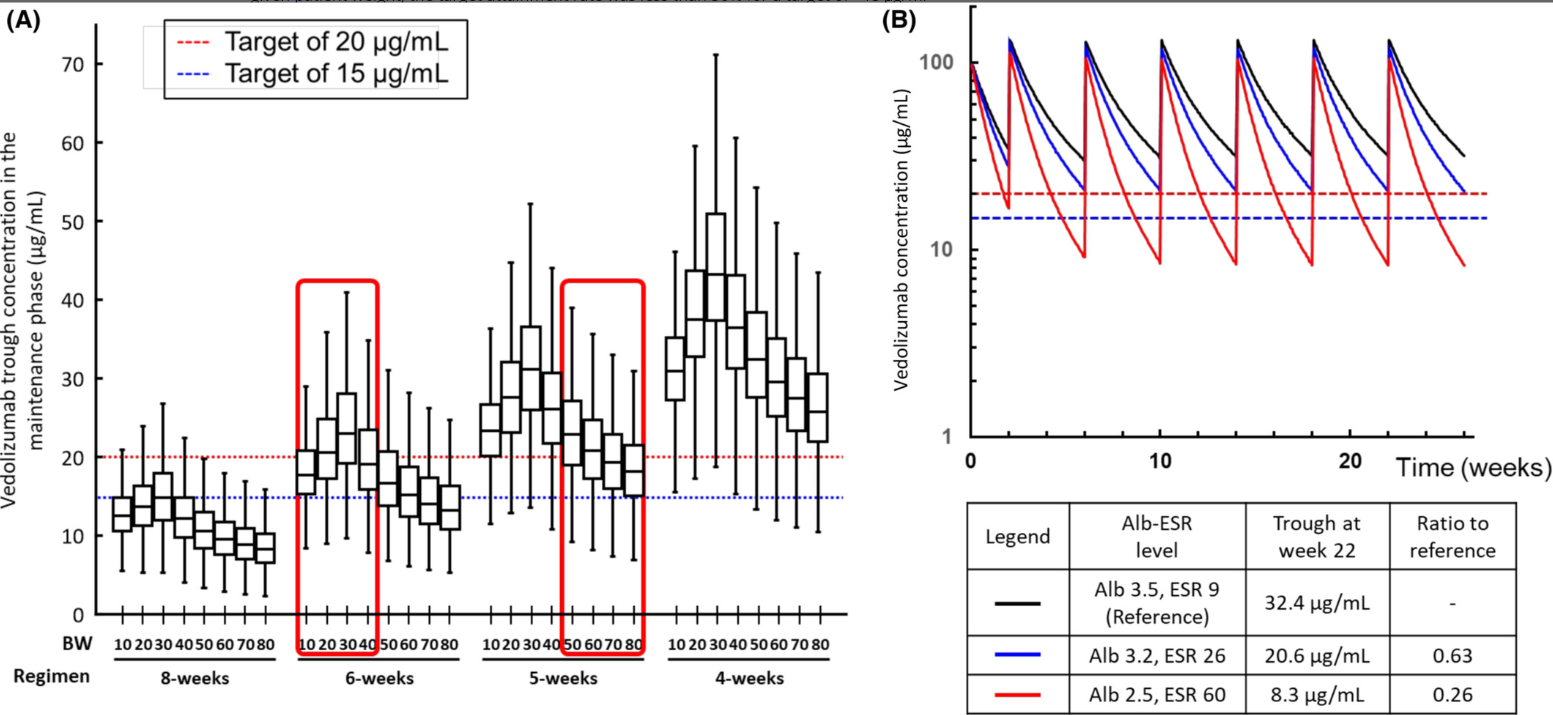
“Using the new model in a simulation analysis of standard vedolizumab infusions (0, 2 and 6 weeks followed by every 8 weeks), we demonstrate that the expected cTrough at week 22 (infusion-5) in the majority of patients would result in drug exposure below current cTrough targets..The dosing simulations in our current study found that receiving standard dosing would lead to <20% of patients achieving a cTrough of 20 μg/ml at infusion-5.”
“The severity of hypoalbuminemia resulted in higher drug CL (lower cTrough) than the inflammatory burden (elevated ESR).”
Infusion-3 cTrough of at least 37 μg/ml and infusion-4 cTrough of at least 20 μg/ml best predicted SFCR (steroid-free clinical remission) at infusion-4. In contrast, we showed inadequate drug exposure during induction (AUCweek 14 of <134,580 μg h/ml) was associated with clinical non-response
My take: This study shows that therapeutic drug monitoring (TDM) is likely to be beneficial in improving outcomes in pediatric patients receiving vedolizumab. Low albumin in particular is associated with increased drug clearance. From this study, it looks like most pediatric patients will need dosing every 4 to 6 weeks to achieve good levels. The authors in their discussion reinforce the utility of TDM to “guide anti-TNF dose optimisations has been shown to improve durability and reduce both immunogenicity and loss of response.”
51 Strik AS, Löwenberg M, Mould DR, Berends SE, Ponsioen CI, van den Brande JMH, et al. Efficacy of dashboard driven dosing of infliximab in inflammatory bowel disease patients: a randomized controlled trial. Scand J Gastroenterol 2021; 56: 145– 154.
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
Background: NSAIDs are well-known to cause gastrointestinal injury. While single center studies have suggested that NSAIDs are associated with increased IBD flares, a systemic review of 18 studies found no consistent association between NSAIDs and IBD exacerbation.
This study included 15,705 (44.8%) and 19,326 (55.2%) IBD patients with and without an NSAID exposure.
Key findings:
Findings from a Cox proportional hazards model suggest an association between NSAIDs and IBD exacerbation (HR 1.24; 95%CI 1.16-1.33)
However, the likelihood of an IBD exacerbation in the NSAID exposed arm preceding NSAID exposure was similar (HR 1.30; 95%CI 1.21-1.39).
Those who received NSAIDs were already at increased risk of experiencing a disease flare. And the prior event rate ratio for IBD exacerbation, as determined by dividing the adjusted HR after NSAID exposure by the adjusted HR for pre-NSAID exposure, was 0.95 (95% CI, 0.89 – 1.01).
“A self-controlled case series analysis of 3,968 patients who had both an NSAID exposure and IBD exacerbation demonstrated similar exacerbation rates in the 1-year preceding exposure, 2-6 weeks post-exposure, and 6-weeks to 6-months post-exposure, but higher incidence 0-2 weeks post-exposure, suggesting potential confounding by reverse causality.” The self-controlled part of the study allowed patients to serve as their own controls which allowed adjustment for many factors that are difficult to control with retrospective studies.
75% of patients with IBD who were prescribed an NSAID did not have an IBD exacerbation during a mean of 5.9 years of follow-up
NSAIDs were commonly used: 36.5% of patients with IBD had received at least one NSAID prescription
NSAIDs use was prescribed more frequently in patients with immune targeted therapy (likely a marker for moderate to severe disease)
Discussion points:
The estimated prior event ratio of 0.95 suggests that the risk of IBD flares in NSAID-exposed patients preceded the use of NSAIDs. The risk of IBD exacerbation did not increase in the 2 weeks to 6 months after NSAID exposure.
The overall association of increased IBD flare is likely related to reverse causation. Patients may take NSAIDs due to arthropathy or other symptoms that may be an early manifestation of a flare.
My take: This study challenges the prevailing view that NSAID use worsen inflammatory bowel disease; it is more likely that IBD exacerbations are due to underlying risk from more severe disease and residual confounding/reverse causality. The study provides reassurance that short-duration use is likely to be well-tolerated in most patients with IBD.
No Exaggeration: Too Many Children Are Dying in the U.S. “The sad fact is that a child or adolescent in the United States is 57% more likely to die by the age of 19 years than those in other wealthy nations.” This is due mainly to more deaths from MVAs and from gun violence.
Link (12-page) Le Bonheur Dysphagia -Thickeners The algorithms suggest starting with oatmeal and then rice cereal for thickening in infants. Recipes are available for how much cereal is needed for each formula based on desired consistency.
This guide reviews the common thickeners including SimplyThick, Nestle ThickenUp Clear, Hormel: Thick & Easy Clear, Gelmix (see below), Purathick, DysphagiAide, Thick-It, Gerber Rice Cereal, Beechnut Oatmeal Cereal
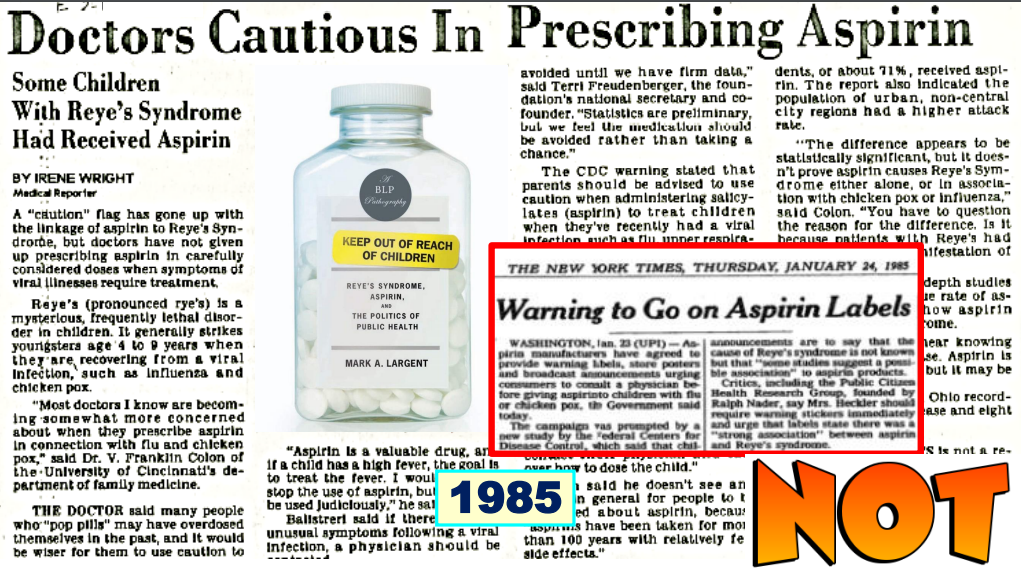
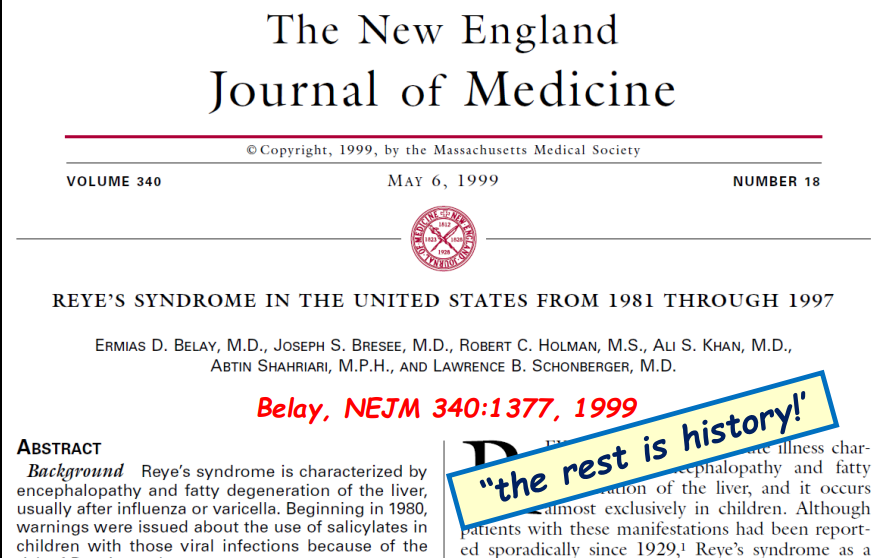
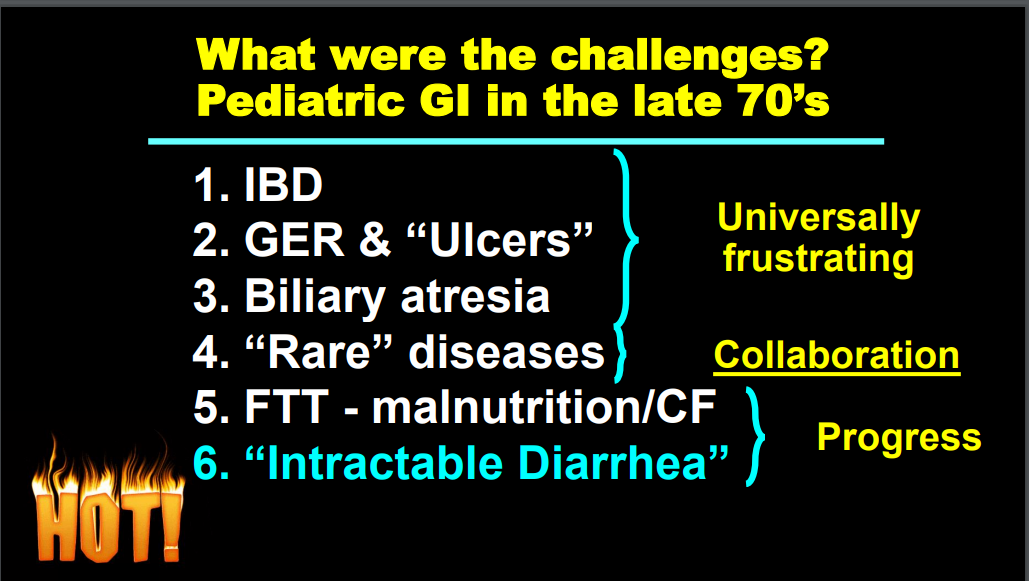
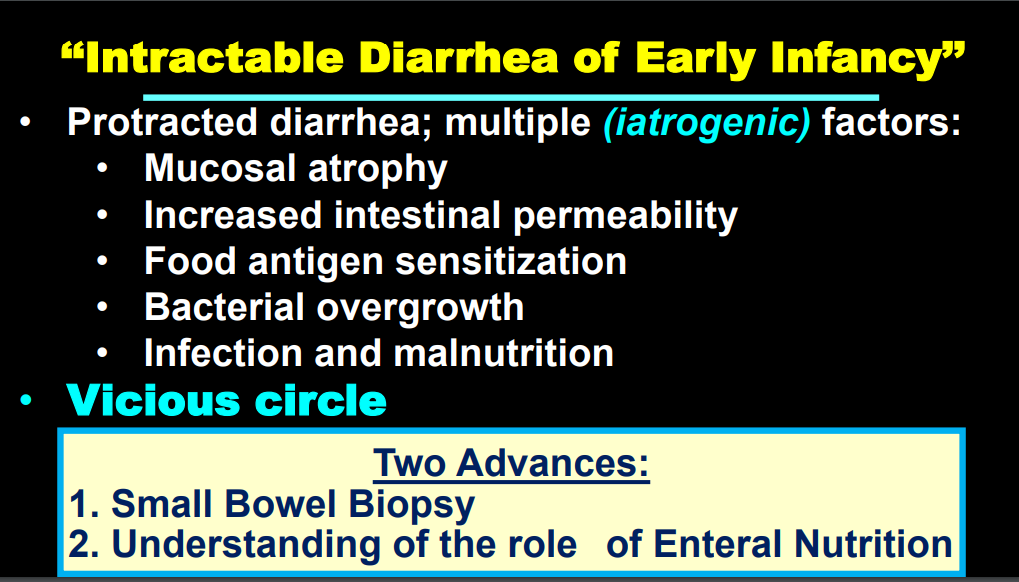
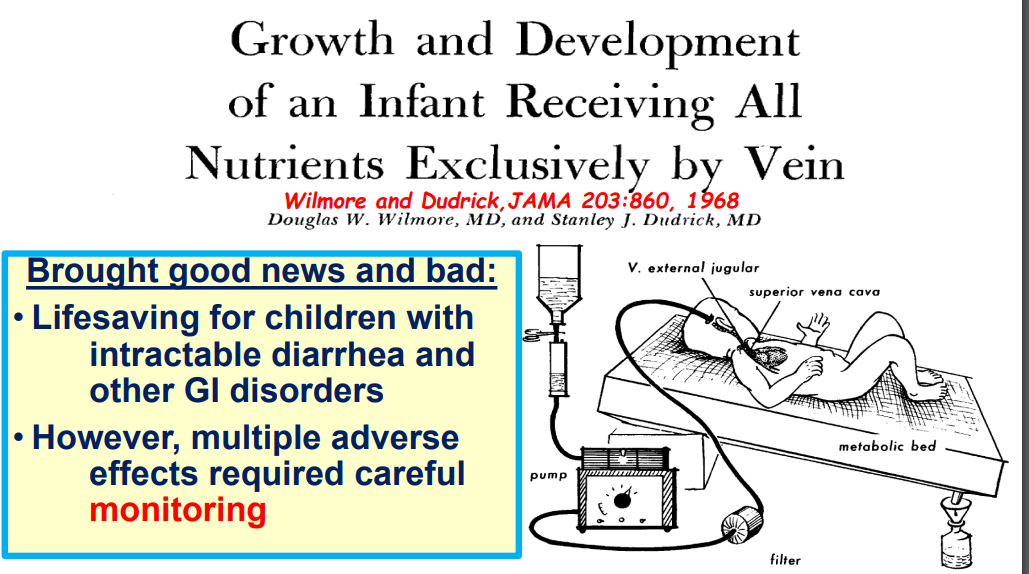
Shortly before attending medical school, I read a book by Lewis Thomas called The Youngest Science. The narrative explains the evolving of medicine into a sophisticated science. The recent Balistreri lecture (given by Dr. Balistreri himself) provides a similar narrative but focused on our specific subspecialty.
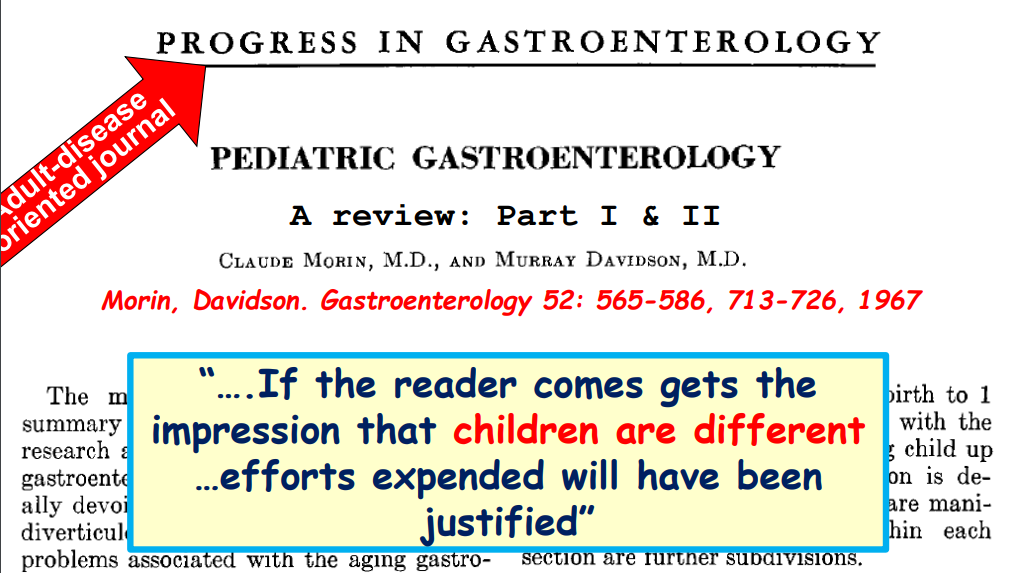
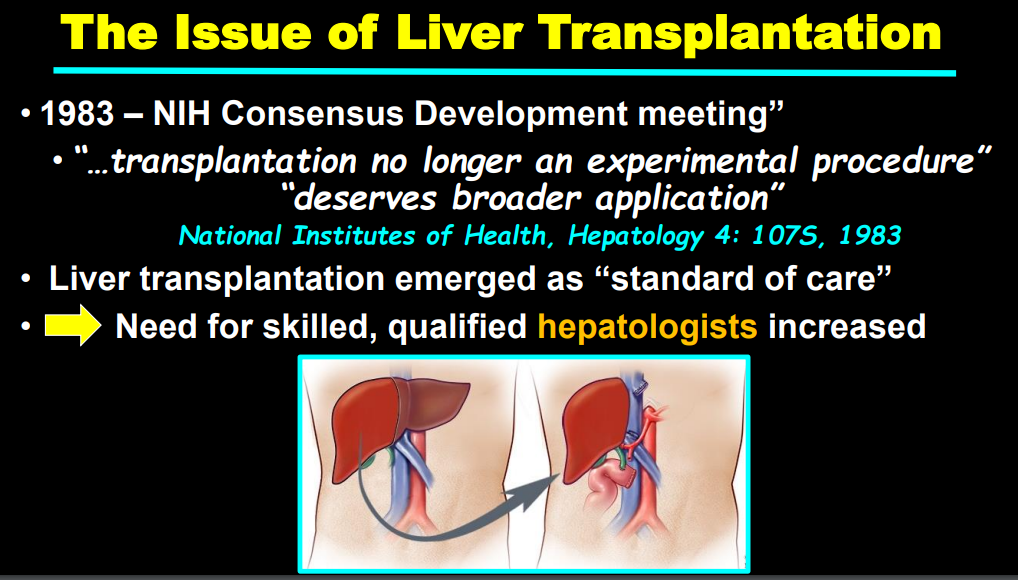
Here are some of the slides:
It was not until 1982 that the role of H pylori was recognized as a causative agent for peptic ulcer disease
Methods: This was “a randomised, double-blind, parallel-group, active-comparator, phase 3b trial (SEAVUE) at 121 hospitals or private practices in 18 countries. We included biologic-naive patients aged 18 years or older with moderately to severely active Crohn’s…Eligible patients were randomly assigned (1:1; via an interactive web response system) to receive ustekinumab (approximately 6 mg/kg intravenously on day 0, then 90 mg subcutaneously once every 8 weeks) or adalimumab (160 mg on day 0, 80 mg at 2 weeks, then 40 mg once every 2 weeks, subcutaneously) through week 56. Study treatments were administered as monotherapy and without dose modifications.”
386 patients were enrolled.
Key findings:
29 (15%) of 191 patients in the ustekinumab group and 46 (24%) of 195 in the adalimumab group discontinued study treatment before week 52
At week 52, 124 (65%) of 191 patients in the ustekinumab group versus 119 (61%) of 195 in the adalimumab group were in clinical remission (CDAI <150)
Endoscopic remission at week 52: ustekinumab 29% and for adalimumab 29%
Endoscopic response at week 52: ustekinumab 42%and for adalimumab 37%
Rapid onset of clinical response was seen with both therapies with improvement noted as early as week 2 assessment
Antidrug antibodies were less frequent with ustekinumab compared to adalimumab: 2% vs 74%.
Infections were reported in 65 (34%) of ustekinumab group compared to 79 (41%) of adalimumab group. Serious infections were reported in four (2%) of 191 patients in the ustekinumab group and five (3%) of 195 in the adalimumab group.
No deaths occurred through week 52 of the study.
My take:
Both medications had a high similar response rate. Ustekinumab had fewer patients discontinue medication and lower immunogenicity which could improve efficacy/duration of response in an extended study.
It is good to see a well-designed head-to-head study rather than a placebo-control arm. Placebo-based studies are hard to justify given the availability of multiple effective agents.
“The majority opinion in Bruen, written by Justice Clarence Thomas, will have a devastating impact on efforts to mitigate gun violence and address racial disparities, but the reasoning used in the decision could cause even more havoc moving forward.”
“Allowing more guns in public does nothing to address the real drivers of criminal behavior, which include social determinants such as poverty, neighborhood violence, poor education, and substandard housing.2 Instead, an increased presence of firearms in public is likely to escalate confrontations, with data suggesting either that people who act aggressively are more likely to arm themselves or that people who are armed are more likely to act aggressively — or perhaps both.1“
“No right is absolute, and the government is able — if not obligated — to prevent harm to the broader public even in the exercise of constitutional rights. Such authority holds for the speech and religious practices covered by the First Amendment, and the Second Amendment should be no different. But the Court’s new theory of the Second Amendment compels lower courts to ignore public health research, empirical evidence, the current gun-violence epidemic, and other rights and liberties of the broader public.”
“Pregnancy is associated with both the initiation of IPV [intimate partner violence] and an increase in IPV severity, making it a particularly dangerous time.3 Homicide is the leading cause of pregnancy-associated death in the United States; pregnant and postpartum women are more than twice as likely to die from homicide as from either hemorrhage or hypertensive disorders.3 …Studies show that abortion access plays an important role in reducing IPV.4 “
“In his dissent in Bruen, Justice Stephen Breyer noted that U.S. women are five times as likely to be killed by an intimate partner if the partner has access to a gun…In expanding the right to carry firearms, the Bruen decision exacerbates safety concerns for people actively trying to escape abusive relationships.”
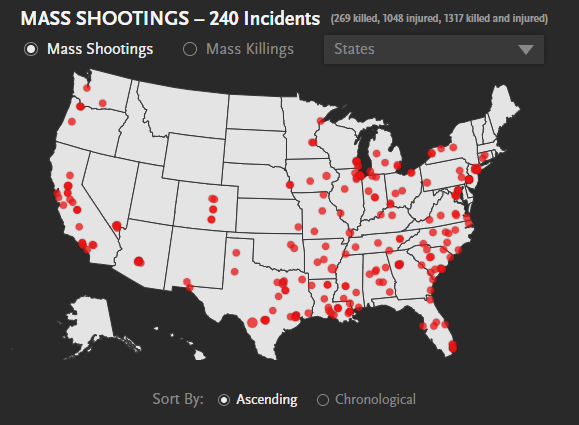
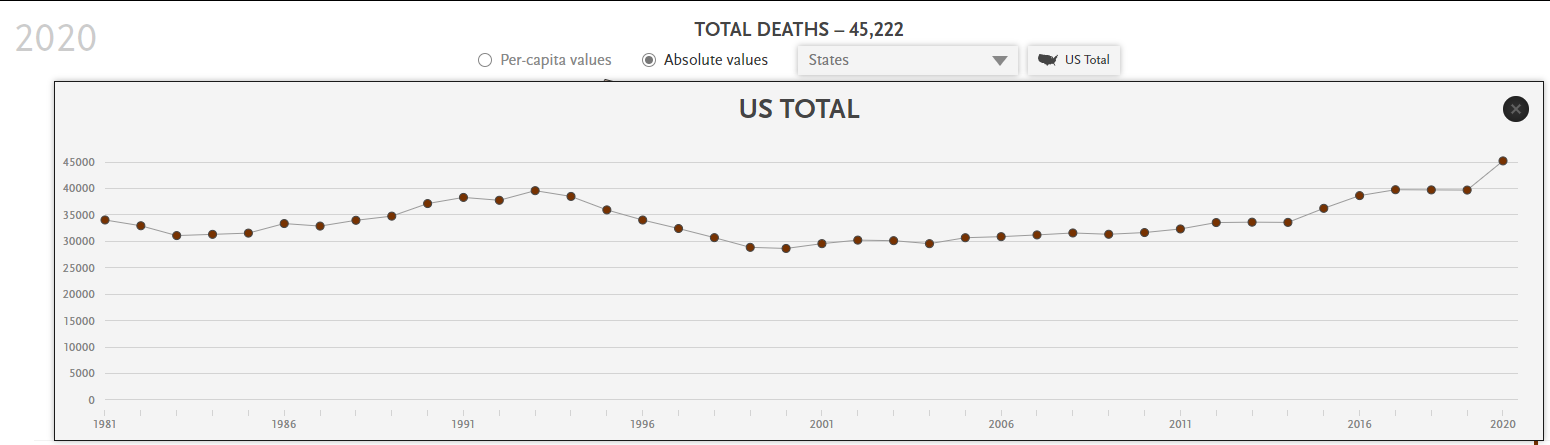
2022: 240 Mass Shootings in U.S as of 6/3022 Gun Deaths have been increasing with more than 45,00 in 2020. Per capita deaths in 2020 -Wyoming and Mississippi have mortality rates
No Exaggeration: Too Many Children Are Dying in the U.S. “The sad fact is that a child or adolescent in the United States is 57% more likely to die by the age of 19 years than those in other wealthy nations.” This is due mainly to more deaths from MVAs and from gun violence.