I am a pediatric gastroenterologist at GI Care for Kids (previously called CCDHC) in Atlanta, Georgia. The goal of my blog is to share some of my reading in my field more broadly. In addition, I wanted to provide my voice to a wide range of topics that often have inaccurate or incomplete information.
Before starting this blog in 2011, I would tear out articles from journals and/or keep notes in a palm pilot. This blog helps provide an updated source of information that is easy to access and search, along with links to useful multimedia sources.
I was born and raised in Chattanooga. After graduating from the University of Virginia, I attended Baylor College of Medicine. I completed residency and fellowship training at the University of Cincinnati at the Children’s Hospital Medical Center. I received funding from the National Institutes of Health for molecular biology research of the gastrointestinal tract.
During my fellowship, I had the opportunity to work with some of the most amazing pediatric gastroenterologists and mentors. Some of these individuals included Mitchell Cohen, William Balistreri, James Heubi, Jorge Bezerra, Colin Rudolph, John Bucuvalas, and Michael Farrell. I am grateful for their teaching and their friendship. During my training with their help, I received a nationwide award for the best research by a GI fellow.
I have authored numerous publications/presentations including original research, case reports, review articles, and textbook chapters on various pediatric gastrointestinal problems. In addition, I have been recognized by Atlanta Magazine as a "Top Doctor" in my field multiple times.
Currently, I am the vice chair of the section of nutrition for the Georgia Chapter of the American Academy of Pediatrics. In addition, I am an adjunct Associate Clinical Professor of Pediatrics at Emory University School of Medicine. Other society memberships have included the North American Society for Pediatric Gastroenterology Hepatology and Nutrition (NASPGHAN), American Academy of Pediatrics, the Food Allergy Network, the American Gastroenterology Association, the American Association for the Study of Liver Diseases, and the Crohn’s and Colitis Foundation.
As part of a national pediatric GI organization called NASPGHAN (and its affiliated website GIKids), I have helped develop educational materials on a wide-range of gastrointestinal and liver diseases which are used across the country. Also, I have been an invited speaker for national campaigns to improve the evaluation and treatment of gastroesophageal reflux disease, celiac disease, eosinophilic esophagitis, hepatitis C, and inflammatory bowel disease (IBD). Some information on these topics has been posted at my work website, www.gicareforkids.com, which has links to multiple other useful resources.
I am fortunate to work at GI Care For Kids. Our group has 17 terrific physicians with a wide range of subspecialization, including liver diseases, feeding disorders, eosinophilic diseases, inflammatory bowel disease, cystic fibrosis, DiGeorge/22q, celiac disease, and motility disorders. Many of our physicians are recognized nationally for their achievements. Our group of physicians have worked closely together for many years. None of the physicians in our group have ever left to join other groups. I have also worked with the same nurse (Bernadette) since I moved to Atlanta in 1997.
For many families, more practical matters about our office include the following:
– 14 office/satellite locations
– physicians who speak Spanish
– cutting edge research
– on-site nutritionists
– on-site psychology support for abdominal pain and feeding disorders
– participation in ImproveCareNow to better the outcomes for children with inflammatory bowel disease
– office endoscopy suite (lower costs and easier scheduling)
– office infusion center (lower costs and easier for families)
– easy access to nursing advice (each physician has at least one nurse)
I am married and have two sons (both adults). I like to read, walk/hike, bike, swim, and play tennis with my free time.
I do not have any financial relationships with pharmaceutical companies or other financial relationships to disclose. I have helped enroll patients in industry-sponsored research studies.
Key points from this review of more than 200 relevant meta-analyses and individual studies:
“A weight-neutral approach to treating obesity-related health conditions may be as, or more, effective than a weight-loss-centered approach, and could avoid pitfalls associated with repeated weight loss failure… Epidemiological studies show that CRF (cardiorespiratory fitness) and PA (physical activity) significantly attenuate, and sometimes eliminate, the increased mortality risk associated with obesity. More importantly, increasing PA or CRF is consistently associated with greater reduction in risk of all-cause and CVD mortality than intentional weight loss.”
“The increased prevalence of weight loss attempts in the United States has coincided with the increased prevalence of obesity. Thus, a weight-centric approach to obesity treatment and prevention has been largely ineffective. It is unlikely that continued focus on weight loss as the primary metric for success will reverse the trends in obesity prevalence or result in sustainable weight loss. In fact, chronic weight cycling is the norm for millions of adults and is likely to remain so for as long as weight loss persists as the cornerstone of obesity treatment. Weight cycling is associated with health risks that are very similar to those associated with obesity, including higher all-cause mortality risk, and may contribute to weight gain.”
Figure 2 from article: “Joint associations between cardiorespiratory fitness (CRF), body mass index (BMI), and all-cause (top) and cardiovascular disease (CVD) (bottom) mortality. Hazard ratios reflect the pooled data from the meta-analyses of Barry et al. for all-cause mortality (Barry et al., 2014) and cardiovascular disease mortality (Barry et al., 2018). For all-cause mortality, the meta-analysis included 6 cohorts of men only, 2 cohorts of women only, and 2 cohorts of both men (~80%) and women. For CVD mortality, the meta-analysis included 8 cohorts of men only and 1 cohort of both men (89%) and women”
“Gastric adenocarcinoma and proximal polyposis of the stomach (GAPPS) is a rare gastric polyposis syndrome defined by numerous polyps (>100) in the fundus and body of the stomach with sparing of the lesser curvature and antrum.” Case report in a 16 yo who ultimately underwent a total gastrectomy. The geneticist identified the APC gene mutation with the OncoGeneDx Colorectal Panel by GeneDx. The rationale for the selection of this gene panel was its ability to examine 20 different genes involved in hereditary colorectal cancer and other gastrointestinal cancers. This panel checks APC, POLE,PTEN, STK11, BMPR1A, SMAD4, ATM, AXIN2, CDH1, CHEK2, EPCAM, MLH1, MSH2, MSH6, MUTYH, NTHL1, PMS2, POLD1, SCG5/GREM1, and TP53 genes
ESPGHAN Juvenile Polyposis Syndrome Recommendations These recommendations are different in that they do not recommend EGD in the pediatric age group: “Surveillance of the upper GI tract in affected or at-risk JPS patients is not required in childhood or teenage years, unless there is unexplained anaemia or upper GI symptoms.”
Are You Familiar with CMMR-D? The term CMMR-D refers to constitutional mismatch repair deficiency. This occurs when an individual inherits two MMR gene defects (rather than one gene defect in Lynch syndrome); with CMMR-D screening recommendations include yearly endoscopic evaluation beginning at age 3 years or at diagnosis.
Key findings from this retrospective review (n=233):
TCAs were not started in only 1.7% (4/233) due to ECG results
Eight (3.4%) had a cardiology referral; one (0.4%) had a prolonged QTc interval
No deaths and no emergency department or hospital visits for arrhythmia or drug overdose occurred
The discussion lists a number of studies generally questioning the utility of pre-medication ECGs while at the same time acknowledging that guidelines in the GI and psychiatric literature support an ECG prior to TCA use. In a large study of sudden cardiac deaths in an adult population, there was no increased risk of death with TCA dosing less than 100 mg/day (Clin Pharmcol Ther 2004; 75: 234-41).
My take (borrowed in part from authors): While “the benefit of screening ECGs remains elusive,” it is still needed to try to avoid “extremely rare but catastrophic events.” The authors, however, recommend followup ECGs only on “patients on concomitant QT prolonging medications or increases to higher dosing ranges.”
There are over 130 different types of CDG with 41 that have liver involvement; 7 with a hepatopathy and 34 with in the context of multisystem disease.
Transferrin isoform analysis (Isoelectric focusing or high-performance liquid chromotography) detects about 50% of the CDGs; hence, genetic panel or exome sequencing is needed for diagnosis in many cases.
4 cases of MMF hepatoxicity are presented along with EM changes which revealed unequivocal mitochondrial abnormalities similar to those seen in primary and secondary mitochondrial disorders
MMF hepatotoxicity was confirmed in mouse study showing that MMF caused various stress changes in the mitochondria
Conclusion: Although MMF is safe for the majority of patients, MMF can cause mitochondrial stress, which may trigger more severe mitochondrial abnormalities in a small subset which can be evident with EM.
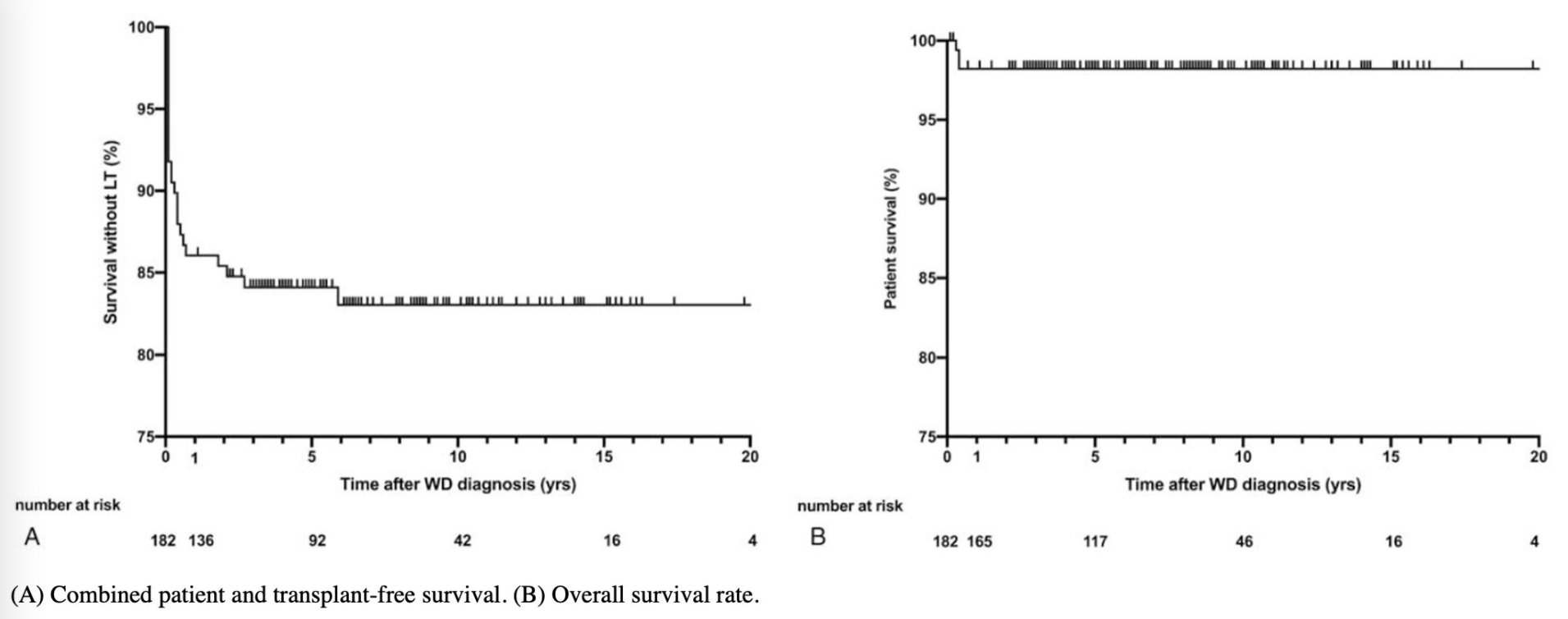
This study examined the clinical data from 182 pediatric patients. WD was diagnosed at a mean age of 10.7 years. Overall survival at 20 years of followup was 98% and patient and transplant-free survival was 84% at 20 years.
This good update provides a lot of useful information regarding fecal microbiota transplantation (FMT) and a word of caution regarding its future availability.
Key pointsregarding FMT:
Long-term safety remains unknown. FMT may lead to susceptibility to chronic inflammatory, allergic, and autoimmune diseases. “FMT has been associated with durable transmission of pro-carcinogenic bacteria from adult donors to pediatric recipients…although the long-term consequences…are unknown.”
Due to transfer of extended spectrum beta-lactamase (ESBL) E coli to 2 immunocompromised adult recipients, further screening of FMT was implemented.
Though there is no published evidence of SARS-CoV-2 fecal transmission, the FDA “advised additional precautions and testing in March 2020; “however, there are no molecular tests with stool…which have received emergency use authorization.” Hence, most FMT programs were on hold as of January 2021.
After 2021, OpenBiome, whose product was recently available again, is expected to stop distribution of FMT donor product due to increased costs of screening and the “promising biotherapeutics” that are in phase III trials.
Biotherapeutic is “loosely defined as drug therapy products where the active substance is extracted from a biological specimen.” The new products are likely to have “increased standardization, safety and practicality.”
The problem in pediatrics: none of these biotherapeutic products have started trials in children. This will lead to treatment problems. Even if one wanted to set up donor-directed FMT, it will be difficult to complete all of the screening recommended by the FDA. It could lead to self-administration by families with uncertain risks.
My take: My first reaction to this article: ‘Oh crap!’ It is sad and ironic that I will miss having available commercial stool for FMT.
To protect children from serious illness, long-term sequelae, hospitalization and death. USA Today recently estimated that less than 700 children have died from COVID-19 -which is still a lot of vaccine-preventable illness (yearly flu deaths in children are closer to about 100 per year). Link (10/8/21) How bad is COVID-19 in kids? See the latest data and charts on kids cases; hospitalizations; deaths
To protect everyone else (from Eric Topol twitter feed):
In this retrospective single-center cohort study with 40 patients (1992-2020), the authors describe the outcomes and heterogeneity of treatments for pedicatric collagenous gastritis (CG). The mean age at diagnosis was 11 years with mean followup of 2.9 years.
Key points:
Presenting symptoms: abdominal pain, vomiting, symptomatic anemia, and nausea. 25 of 40 had a colonoscopy at time of index EGD
75% had iron-deficiency anemia which responded well to iron supplementation
Comorbid conditions included autoimmune disorders in 12.5% and immunodeficiencies in 5%. 7 (17.5%) had excess collagen in duodenum, 3 (7.5%) had collagenous colitis, and 1 (2. 5%)had collagenous ileitis.
85% of diagnosis were made on initial review of biopsy slides; other cases were identified subsequently either due to repeat endoscopy or further slide review. CG is “known to be patchy
No treatments were clearly effective in improving histology. Treatments included PPI/H2RAs in 40%, laxatives in 20%, cyproheptadine in 12.5%, antiemetics in 12.5%, cafafate in 7.5%, budesonide in 7.5% and others less frequently
92% had persistent abnormal endoscopic findings and 73% had persistent thickened subepithelial collagen. In those without excess collagen deposition at last EGD, some of this could be related to patchy distribution as well as improvement
Though histology often did not improve, 87.5% had improvement or resolution of symptoms
Long-term outcomes remain unknown. While there is concern for possible malignant transformation, to date “no gastric epithelial or lymphoid malignancies have been…reported”
My take: Collagenous gastritis is poorly understood. Fortunately, most patients symptoms resolve/improve.
“Remarkably safe and highly effective mRNA COVID-19 vaccines are now available for widespread use and should be given to all adult patients with CLD and LT recipients. The online companion document located at https://www.aasld.org/about-aasld/covid-19-resources will be updated as additional data become available regarding the safety and efficacy of other COVID-19 vaccines in development.”
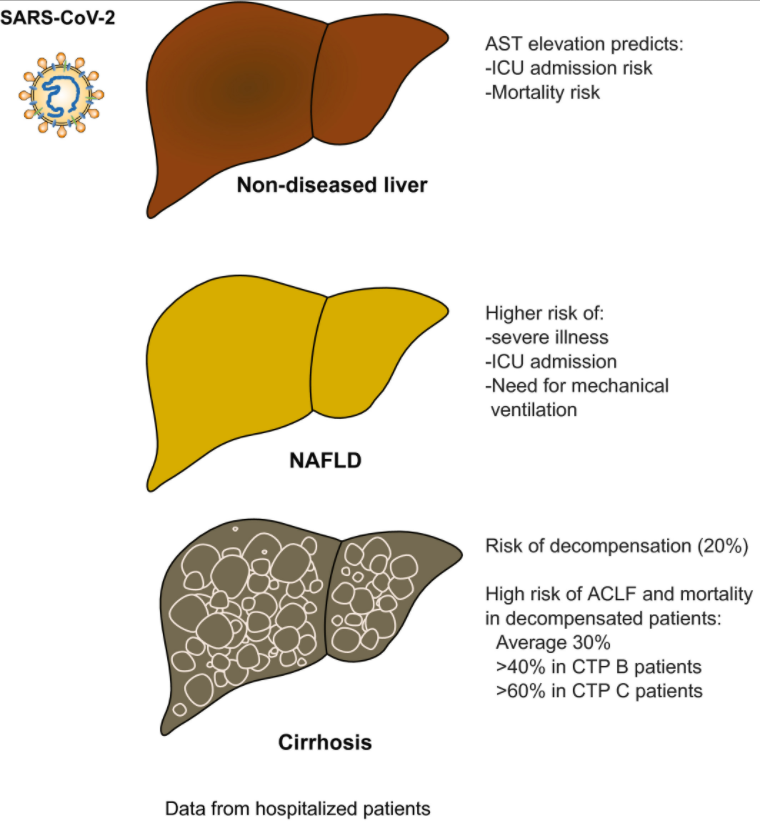
“The presence of liver injury is a surrogate marker for more severe disease and higher mortality in patients with COVID-19. An elevated AST level is the most robust predictor of poor outcome.”
“Liver injury and mortality in COVID-19 are likely multifactorial, driven by a sustained and excessive systemic release of proinflammatory and prothrombotic cytokines following SARS-CoV-2 infection, iatrogenic injury caused by DILI, hemodynamic changes associated with mechanical ventilation or vasopressor use, and worsening of underlying liver injury in those with CLD.”
“Risk of de novo liver injury appears limited in patients without CLD, and only rare cases of COVID-19–related ACLF [acute-on-chronic liver failure] were observed.”
“COVID-19–related liver injury and mortality in patients who were hospitalized with and without chronic liver disease (CLD). Patients without CLD usually present with AST elevation, which correlates with ICU admission and mortality. Among patients with CLD, NAFLD has the highest risk of severe illness, ICU admission, and need for mechanical ventilation. Patients with cirrhosis are at risk for decompensation, and patients who are decompensated have a high risk of acute-on-chronic liver failure (ACLF) and mortality.”–Abbreviations: CTP, Child-Turcotte-Pugh; ICU, intensive care unit.
“We are caring for young people with soaring rates of depression, anxiety, trauma, loneliness, and suicidality that will have lasting impacts on them, their families, their communities, and all of our futures,” said AACAP President Gabrielle A. Carlson, M.D. “We cannot sit idly by. This is a national emergency, and the time for swift and deliberate action is now.”
These organizations make several recommendations to policy makers including more access for mental health services. (I worry that we do not have sufficient numbers of qualified mental health practitioners to meet the challenge.)
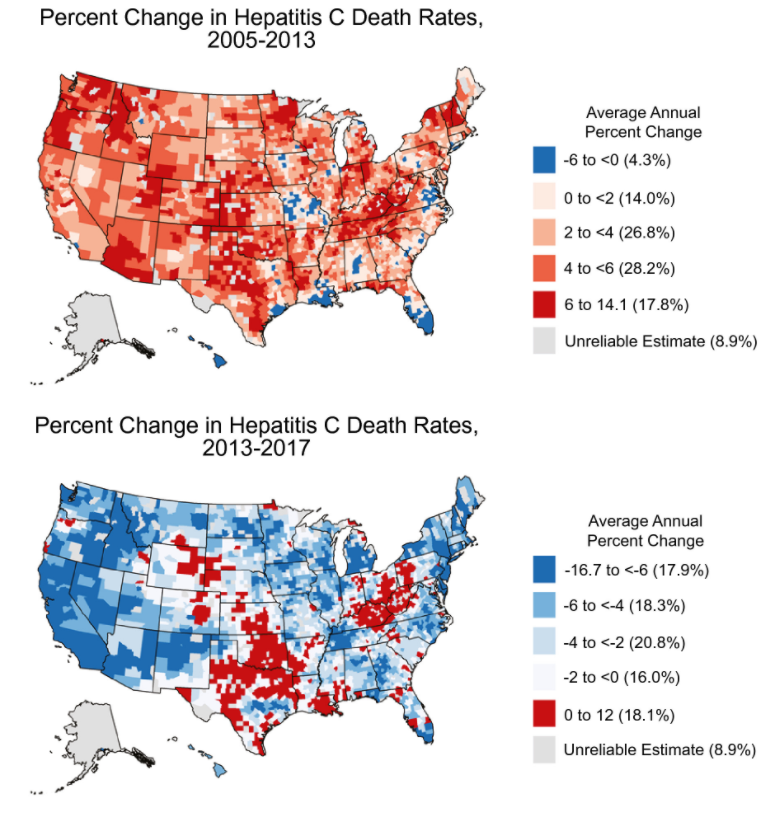
The authors used county-level HCV death rates and assessed trends in HCV mortality from 2005 to 2013 and from 2013 to 2017; the study is derived from mortality data from the National Vital Statistics System.
Key Findings:
Nationally, the age-adjusted HCV death rate peaked in 2013 at 5.20 HCV deaths per 100,000 persons and decreasing to 4.34 per 100,000 persons in 2017
There was heterogeneity in HCV mortality with the highest rates being concentrated in the West, Southwest, Appalachia, and northern Florida. 80% of counties had improvement in HCV mortality
My take: This study showed widespread improvement trends in HCV death rates from 2013 to 2017 and provides benchmarks for further progress. However, other studies have shown increasing rates of HCV tied to opioid crisis which could impact long-term outcomes as well.
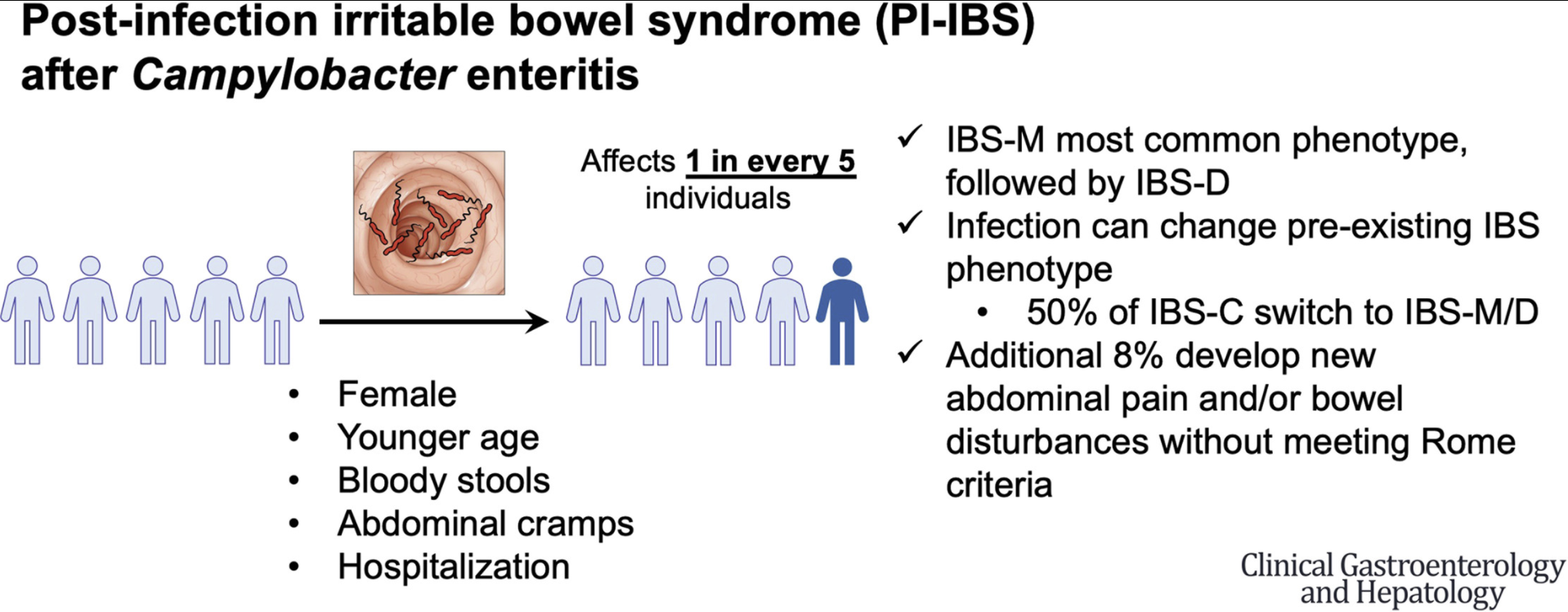
The Minnesota Department of Health collects data on symptoms and exposures upon notification of Campylobacter cases. In this 6-9 month followup survey of 1667 (2011-2019) out of a total of 3586 patients, the authors identified 1418 without preexisting IBS.
Key findings:
301 (21%) subsequently developed IBS. Most of these individuals had IBS-mixed (54%), followed by IBS-diarrhea (38%), and IBS-constipation (6%)
Additionally, the authors note that 121 patients (8.5%) had new GI problems after infection that did not meet thresholds set by Rome criteria
Among patients with IBS-mixed or IBS-diarrhea before infection, 78% retained their subtypes after infection. In contrast, only 50% of patients with IBS-constipation retained that subtype after infection;40% transitioned to IBS-mixed
Of patients with pre-existing IBS, 38% had increased frequency of abdominal pain after Campylobacter infection
One limitation of the study is ‘responder bias.’ There may be a lower rate of IBS/GI symptoms in the subset of patients who did not respond to survey.
My take: A lot of people develop IBS and other GI symptoms after Campylobacter infection; those with IBS often have intensification of their symptoms.
Related study: Am J Gastroenterol 2012 Jun;107(6):891-9. “Norovirus GE leads to the development of PI-IBS in a substantial proportion of patients (13%), similar to that reported after bacterial GE.”