I am a pediatric gastroenterologist at GI Care for Kids (previously called CCDHC) in Atlanta, Georgia. The goal of my blog is to share some of my reading in my field more broadly. In addition, I wanted to provide my voice to a wide range of topics that often have inaccurate or incomplete information.
Before starting this blog in 2011, I would tear out articles from journals and/or keep notes in a palm pilot. This blog helps provide an updated source of information that is easy to access and search, along with links to useful multimedia sources.
I was born and raised in Chattanooga. After graduating from the University of Virginia, I attended Baylor College of Medicine. I completed residency and fellowship training at the University of Cincinnati at the Children’s Hospital Medical Center. I received funding from the National Institutes of Health for molecular biology research of the gastrointestinal tract.
During my fellowship, I had the opportunity to work with some of the most amazing pediatric gastroenterologists and mentors. Some of these individuals included Mitchell Cohen, William Balistreri, James Heubi, Jorge Bezerra, Colin Rudolph, John Bucuvalas, and Michael Farrell. I am grateful for their teaching and their friendship. During my training with their help, I received a nationwide award for the best research by a GI fellow.
I have authored numerous publications/presentations including original research, case reports, review articles, and textbook chapters on various pediatric gastrointestinal problems. In addition, I have been recognized by Atlanta Magazine as a "Top Doctor" in my field multiple times.
Currently, I am the vice chair of the section of nutrition for the Georgia Chapter of the American Academy of Pediatrics. In addition, I am an adjunct Associate Clinical Professor of Pediatrics at Emory University School of Medicine. Other society memberships have included the North American Society for Pediatric Gastroenterology Hepatology and Nutrition (NASPGHAN), American Academy of Pediatrics, the Food Allergy Network, the American Gastroenterology Association, the American Association for the Study of Liver Diseases, and the Crohn’s and Colitis Foundation.
As part of a national pediatric GI organization called NASPGHAN (and its affiliated website GIKids), I have helped develop educational materials on a wide-range of gastrointestinal and liver diseases which are used across the country. Also, I have been an invited speaker for national campaigns to improve the evaluation and treatment of gastroesophageal reflux disease, celiac disease, eosinophilic esophagitis, hepatitis C, and inflammatory bowel disease (IBD). Some information on these topics has been posted at my work website, www.gicareforkids.com, which has links to multiple other useful resources.
I am fortunate to work at GI Care For Kids. Our group has 17 terrific physicians with a wide range of subspecialization, including liver diseases, feeding disorders, eosinophilic diseases, inflammatory bowel disease, cystic fibrosis, DiGeorge/22q, celiac disease, and motility disorders. Many of our physicians are recognized nationally for their achievements. Our group of physicians have worked closely together for many years. None of the physicians in our group have ever left to join other groups. I have also worked with the same nurse (Bernadette) since I moved to Atlanta in 1997.
For many families, more practical matters about our office include the following:
– 14 office/satellite locations
– physicians who speak Spanish
– cutting edge research
– on-site nutritionists
– on-site psychology support for abdominal pain and feeding disorders
– participation in ImproveCareNow to better the outcomes for children with inflammatory bowel disease
– office endoscopy suite (lower costs and easier scheduling)
– office infusion center (lower costs and easier for families)
– easy access to nursing advice (each physician has at least one nurse)
I am married and have two sons (both adults). I like to read, walk/hike, bike, swim, and play tennis with my free time.
I do not have any financial relationships with pharmaceutical companies or other financial relationships to disclose. I have helped enroll patients in industry-sponsored research studies.
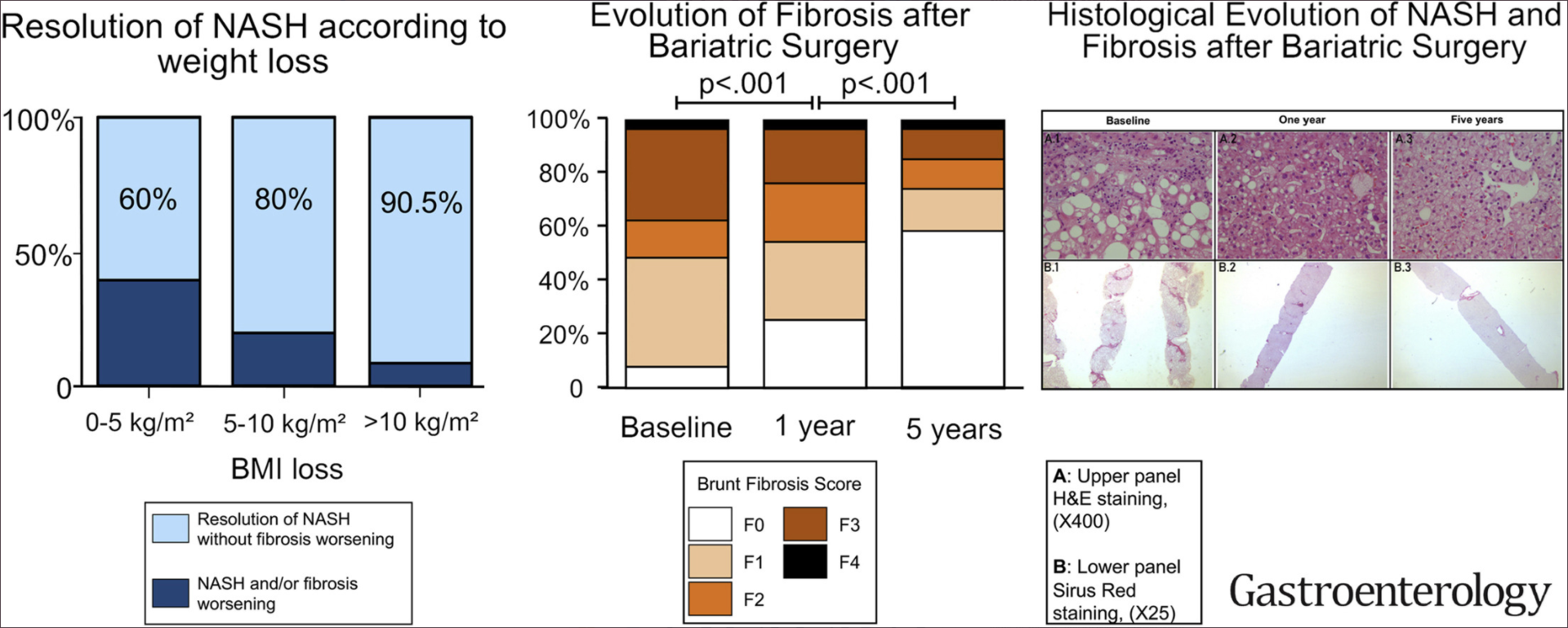
This was a prospective study of 180 severely obese patients with biopsy-proven NASH.
Key findings:
NASH: At 5 years after bariatric surgery, NASH was resolved, without worsening fibrosis, in samples from 84% of patients (n = 64; 95% confidence interval, 73.1%-92.2%).
Fibrosis: Fibrosis decreased, compared with baseline, in samples from 70.2% of patients (95% CI, 56.6%-81.6%). Fibrosis disappeared from samples from 56% of all patients (95% CI, 42.4%-69.3%) and from samples from 45.5% of patients with baseline bridging fibrosis.
Graphic Abstract
My take: This study showed that patients with NASH who underwent bariatric surgery had resolution of NASH in liver samples from 84% of patients 5 years later. The reduction of fibrosis was progressive, beginning during the first year and continuing through 5 years.
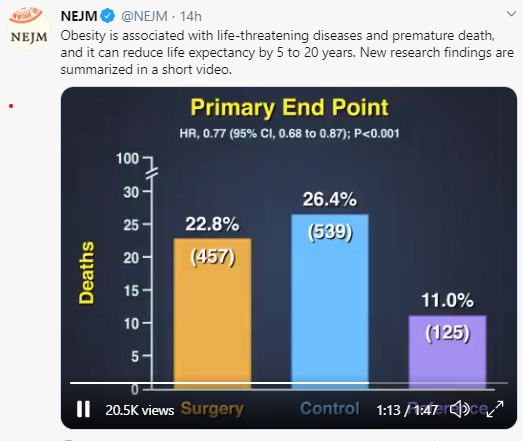
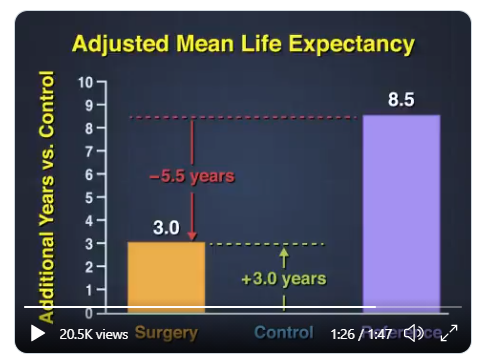
A recent study (LMS Carlsson et al. NEJM 2020; 383: 1535-43) was summarized in a quick take. Essentially, obese subjects who underwent bariatric surgery survived three years longer than a control group who had not undergone surgery but lived 5 years shorter than a reference group without obesity.
The authors speculate on the reasons why the bariatric subjects continued to have a lower life expectancy than controls after surgery:
Above-normal BMI even after surgery
Irreversible effects of obesity-related metabolic dysfunction
Surgical complications
Higher risk of alcohol abuse, suicide, and trauma (including fall-related); these factors were identified in the SOS study more often than in those who had not undergone bariatric surgery
Since there have been improvements in bariatric surgery since the time of this cohort underwent surgery (1987-2001), it is possible that the average gain in life expectancy would be greater.
Rock artThis tweet was posted on 10/21/20Ful Text Link: COVID-19 Mortality Risk in Down Syndrome: Results From a Cohort Study Of 8 Million Adults15 min video Link: How America Helped Defeat the Coronavirus* (not in U.S.). an excerpt: We’ve all heard how U.S. leadership failed its citizens with its pandemic response. We had the playbooks, we had the money, we had the experts. We just … didn’t use them. But it turns out, other countries did. Because U.S. public health leaders and scientists have been planning for a catastrophe just like Covid-19 for decades, and, in typical American fashion, we didn’t just write the pandemic playbook — we exported it around the world.
Diagnosis of constipation is primarily based on history and physical exam –not abdominal xray (AXR). In a recent quality improvement study (G Moriel et al. J Pediatr 2020; 225: 109-116. Reducing Abdominal Radiographs to Diagnose Constipation in the Pediatric Emergency Department), ED physicians were trying to improve adherence to evidence-based guidelines for diagnosis of constipation in otherwise healthy children. In this article, the authors note evidence “has shown abdominal radiographs to be unreliable in establishing an association between clinical symptoms of constipation and fecal load on abdominal radiographs.”
As part of the study, the researchers provided two 20-minute presentations to the pediatric emergency department providers and sent emails to them and to resident housestaff. The email for ED provider’s included the provider’s baseline abdominal radiograph frequency. After study was initiated, a followup email was sent with similar information with key information on the project along with individualized data.
Key findings:
After the QI interventions, the total percentage of abdominal radiograph decreased to 18% (from 36% at baseline). This 18% decrease was significant ( P < .001) and sustained over a 12-month follow-up period.
The average length of stay was 1.07 hours longer for children who had an abdominal radiograph.
Clinically important return visits to the emergency department were uncommon during the postintervention phase (125/1830 [6.8%]), and not associated with whether or not an abdominal radiograph was performed at the initial visit.
While the study focused on healthy children, the authors noted that the overall population (6 mo-18 years) experienced a decline in AXR usage, regardless of exclusion criteria. At baseline the rate of AXR was 39.5% (1550/3926) which decreased to 20.7% (478/2311).
One interesting piece of data was showing that this intervention resulted in a sustained reduction for 12 months after the intervention observation period, which mitigates the potential influence of the Hawthorne effect.
My take: In my view, the keys to this intervention was providing individualized metrics as well as having leadership in establishing this project. The individualized metrics help physicians recognize when they are outliers and to motivate them to address this.
A recent study (SE Tarbell et al J Pediatr 2020 225: 109-108. Children with Functional Nausea—Comorbidities outside the Gastrointestinal Tract) highlights the frequent comorbidities in children with functional nausea. The authors have combined prospective and retrospective elements with specific questionnaires and review of the electronic medical records.
Key points:
High rates of comorbidities were noted: Abdominal pain 94%, Headache 83%, Orthostatic Intolerance 81%, Fatigue 75%, Disturbed sleep 71%, Anxiety 59%, and Constipation 57%. Other frequent findings included vomiting in 51%, Allergies 54%, , Joint Pain 46%, Hypermobility in 37%.
69.5% of subjects missed more than 10 days of school due to their symptoms.
There was extensive testing in this cohort (n=63), including 96 endoscopies, and 199 radiologic tests. In addition, 4 patients had cholecystectomies.
Among 64 EGDs, 28 were considered abnormal. The authors claim that 6 had specific findings: H pylori (n=2), polyps (n=2), celiac disease (n=1), and lactase deficiency (n=1).
It is likely that H pylori and celiac disease could have been identified/suspected by non-invasive testing; these two findings may make a diagnosis of functional nausea more tricky.
Lactase deficiency could be considered a normal finding.
The authors state that 32 of 59 AXRs had “moderate to severe constipation” based on stool burden
Overall, this article makes some useful points about the high rate of comorbidities with functional nausea but I disagree with some of the other discussion points.
The authors claim that “negative tests can reassure families of the absence of a more serious underlying condition.” This assertion has been disputed in other studies. In one study (A Rolfe et al. JAMA Intern Med. 2013;173(6):407-416 Full text: Reassurance After Diagnostic Testing With a Low Pretest Probability of Serious Disease), the authors conclude that ‘diagnostic tests for symptoms with a low risk of serious illness do little to reassure patients, decrease their anxiety, or resolve their symptoms, although the tests may reduce further primary care visits.’
The authors also have a permissive attitude regarding AXRs saying “a radiograph may validate a diagnosis of constipation.” Yet the preponderance of evidence indicates that AXRs are not needed or recommended for the diagnosis of constipation. The juxtaposition of this statement on page 107 of this issue with the next article on page 109 which details a quality improvement process of reducing abdominal radiographs to diagnose constipation in the ED is interesting. The ED physicians in the next article are trying to adhere to evidence-based guidelines; in this article, the authors correctly note that evidence “has shown abdominal radiographs to be unreliable in establishing an association between clinical symptoms of constipation and fecal load on abdominal radiographs.”
My take: Tarbell et al show that in patients with functional nausea, nausea is the tip of the symptom iceberg. Generally, radiographic and endoscopic diagnostic studies have very low yield and should be discouraged.
A recent study (AG Feldman et al. J Pediatr 2020; 225: 252-258. Subacute Liver Failure Following Gene Replacement Therapy for Spinal Muscular Atrophy Type 1) describes two children who developed subacute liver failure after treatment with onasemnogene (AVXS-101). This gene therapy was approved by the FDA in 2019 and more than 335 children have been treated. Both children presented about 3-8 weeks after their AVXS-101 infusion (despite steroid therapy), at 6 months of age and 20 months of age respectively, with ALT values above 1600 and INR of at least 1.5 (despite Vitamin K). Both had liver biospies and then were treated with methylprednisolone, starting at 20 mg/kg/day.
Key points:
The authors speculate that subacute liver failure was due to a systemic hyperinflammatory reaction
The authors recommend screening prior to AVXS-101 therapy with LFTs, GGT, and INR; if baseline labs are elevated, further workup is recommended (eg. A1AT, HBV, HCV, ANA, anti-SMA, anti-LKM, and ultraound)
While this reaction has been with AVXS-101, there are other gene therapies with adenovirus-vector which could trigger similar reactions
The authors note that the “package insert for onasemnogene recommends prednisolone (1 mg/kg/day) should be given in the 24 hours before infusion and should be continued for 30 days after infusion.”
After infusion, it is “necessary to monitor liver tests frequently in the first 2 months”
My take: This new therapy’s risks are substantial; however, the benefits from treatment can be life-altering as well.
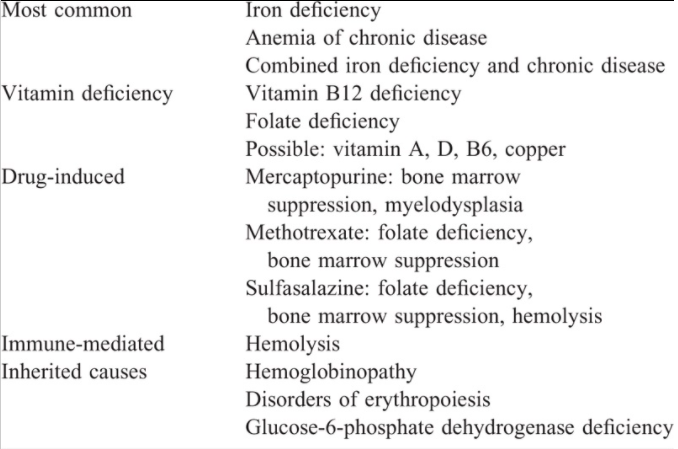
Main Types of Anemia in Inflammatory Bowel Disease:
“IDA is the most common cause of anemia in children with IBD. True iron deficiency results from a number of factors, including chronic blood loss secondary to gastrointestinal bleeding, decreased iron absorption because of tissue or systemic inflammation and from reduced absorptive surface area. “
“Functional iron deficiency (FID) results from high levels of circulating hepcidin, which binds to and disables the iron transporter, ferroportin. Under the influence of hepcidin, ferroportin-mediated export of intracellular iron is stalled, leaving the iron trapped within the enterocytes and macrophages… the underlying inflammation, which induces hepcidin production can result in anemia secondary to FID.”
Anemia of chronic disease (ACD) “occurs from various downstream pathways secondary to inflammation.”
Table 4:
Recommended Testing
Screening Tests: “initially a complete blood count (CBC), CRP, and ferritin levels should be performed. If a patient is found to be anemic, then testing should include CBC with differential, including mean corpuscular volume (MCV), mean corpuscular Hgb concentration (MCHC), red cell distribution width (RDW), reticulocyte count, CRP, serum ferritin, and transferrin saturation (TSAT)”
Serum iron level … is … unreliable in the assessment of iron deficiency as the level fluctuates with several variables.
Transferrin saturation (TSAT) is a measure of the iron content in the circulating transferrin and reflects the availability of utilizable iron
Treatment of Anemia
In mild anemia (Hgb ≥10 g/dL) and/or quiescent disease, oral iron should be tried first.
Parenteral iron is indicated when oral iron is ineffective or poorly tolerated, in patients with moderate-severe anemia and/or with active inflammation.
According to ECCO guidelines, an IV replacement goal of achieving of ferritin level of up to 400 μg/L is more likely to prevent recurrence of anemia…a transferrin saturation of 50% and serum ferritin of 800 μg/L should not be exceeded
Regarding iron effects on microbiome: studies indicate that dysbiosis at baseline worsens the unfavorable shifts in microbiome with oral iron therapy…Our position, however, is that further studies are required in humans before any reliable conclusions can be drawn. [My question: have the effects of oral iron supplementation on the microbiome been compared to IV iron supplementation on the microbiome?]
Table 6 lists various iron products including costs and dosing.
The hypersensitivity reactions to parenteral iron are mostly secondary to iron nanoparticles that trigger complement activation-related pseudo-allergy (CARPA)….It is important that parenteral iron be administered by trained personnel. Emergency medications and resuscitative equipment should be available during these infusions.
My take: This is a useful resource for a very common problem.
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition
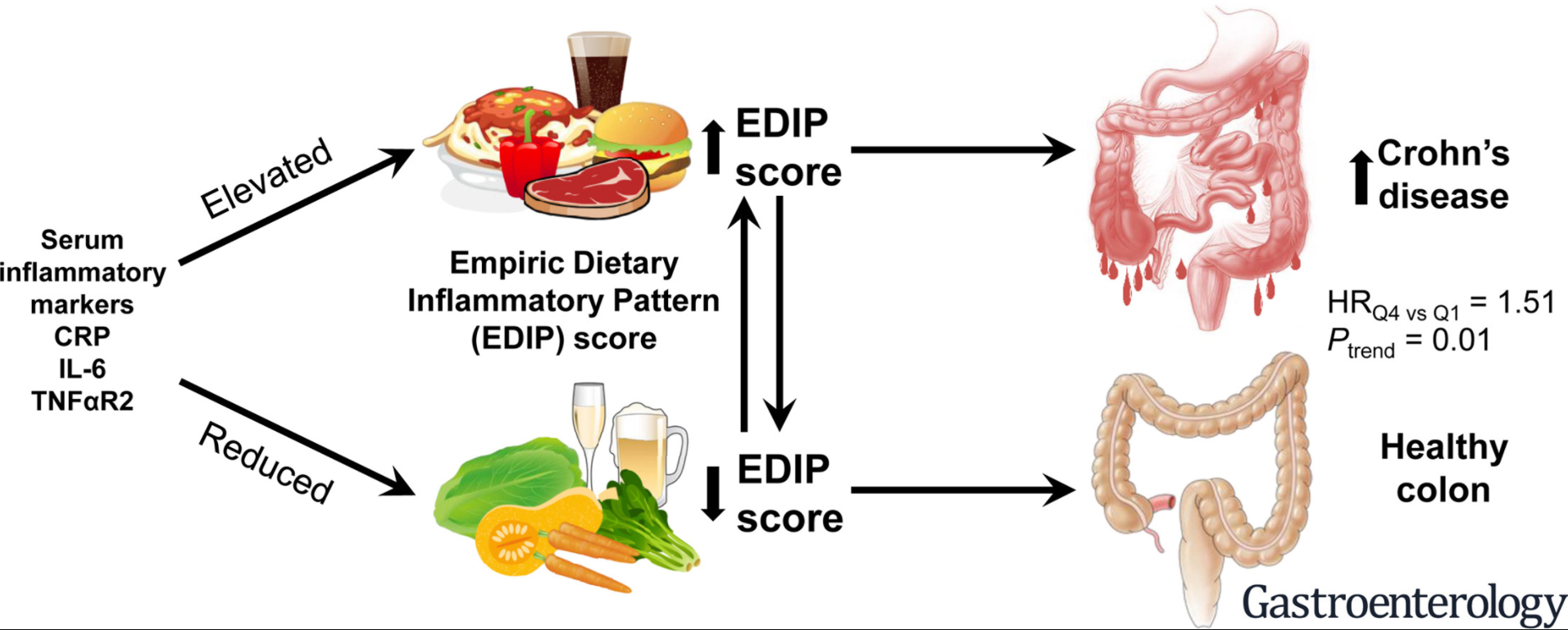
The authors used Empirical dietary inflammatory pattern (EDIP) scores which were calculated based on the weighted sums of 18 food groups obtained via food frequency questionnaires. n=166,903 women and 41,931 men
Key findings:
“In an analysis of 3 large prospective cohorts, we found dietary patterns with high inflammatory potential to be associated with increased risk of CD but not UC.”
Compared with participants in the lowest quartile of cumulative average EDIP score, those in the highest quartile (highest dietary inflammatory potential) had a 51% higher risk of CD (HR 1.51; 95% CI 1.10–2.07; Ptrend = .01).
There were 328 cases of CD and 428 cases of UC over 4,949,938 person-years of follow-up. The median age at IBD diagnosis was 55 years (range 29–85 years)
Discussion points:
Food groups that are associated with unfavorable EDIP scores “are characterized by calorie-dense foods high in animal proteins, saturated fats, and glycemic carbohydrates, such as red meat, refined grain, and high-energy soft drinks.”
“Dietary patterns resembling the Western diet, characterized by higher intake of red meat, high-fat dairy, and refined grains, have been proposed to trigger the onset of intestinal inflammation by inducing changes in gut microbiome, altering host homeostasis, and regulating T-cell immune response.”
“In contrast, diets rich in fruit, vegetables, legumes, whole grains, fish, and poultry, resembling a more prudent and Mediterranean dietary pattern with high fiber and marine ω-3 content, may have anti-inflammatory effects.”
VDZ was initiated at median age of 16 years [IQR 15–18], 69% were male, 65% had large duct involvement, 19% had (Metavir F3/F4) fibrosis and 59% had ulcerative colitis.
Key findings:
Overall, there was a mild increase in median GGT after initiation of VDZ. Of 32 patients with abnormal GGT at baseline, 22% had a liver biochemical response (defined as GGT <50 or at least a 75% decline) after 9 to 12 months
For IBD, 32% achieved remission, 30% had a clinical response, and 38% had no response
In the discussion, the authors note that their findings are in agreement with three retrospective studies in adults which have shown that VDZ is not effective for PSC in patients with IBD.
My take: This study indicates that VDZ is not likely to help with PSC, though 62% of IBD patients had improvement in their GI disease.