D van den Nieuwenhof, . et al. The Journal of Pediatrics, Volume 288, 114807. Open Access! Long-Term Outcomes of Surgical Drooling Treatment in Individuals with Neurodevelopmental Disabilities: A Retrospective Cohort Study
Background: “Long-term relief of drooling remains a challenge due to the side effects of anticholinergics,13 and botulinum neurotoxin type A injections provide only a temporary relief of drooling with potential loss of effect after repeated injections.15…Surgery for drooling is often considered if moderate to severe drooling persists in children after the age of 12 years.”
Submandibular duct relocation (SMDR) “is currently considered the first choice among these surgical procedures and involves the relocation of the submandibular duct papillae to the base of the tongue, allowing saliva to flow posteriorly into the oropharynx and trigger the swallowing reflex…Since the saliva is rerouted to the oropharynx, an adequate pharyngeal swallowing phase is a prerequisite for this surgery to prevent saliva aspiration and choking. Thus, SMDR is contraindicated in patients at risk of aspiration… In these cases, SMGE [submandibular gland excision] or SDL [submandibular duct ligation] can be considered.19“
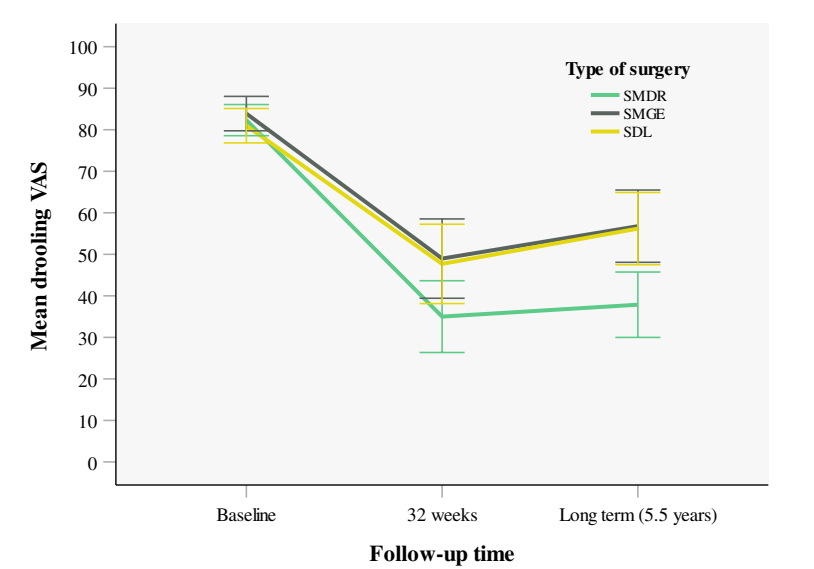
Methods: This was a retrospective cohort study with 255 patients. The authors used the visual analog scale (VAS) for drooling as the primary outcome to compare the long-term treatment outcomes of submandibular duct relocation (SMDR), submandibular gland excision (SMGE), and submandibular duct ligation (SDL) for the treatment of anterior drooling in individuals with neurodevelopmental disabilities.
Key findings:
- A mean reduction in VAS was observed of 44.9 points for SMDR (P < .001), 27.2 for SMGE (P < .001), and 25.4 for SDL (P < .001).
- A significant degree of drooling recurrence was observed after SDL and SMGE at long-term follow-up
Discussion points:
- “SMDR is an invasive treatment requiring a night of postsurgical intubation and observation in intensive care. In specifically vulnerable children, less invasive alternatives such as SDL might therefore be preferential.”
- “Since drooling is predominantly caused by insufficient swallowing, maintaining a balance between saliva production and clearance through swallowing is essential. SMGE and SDL inhibit saliva secretion from the submandibular glands, thereby reducing the overall volume of saliva produced.19,20 However, these procedures do not actively influence the swallowing process…A durable effect after SMGE and SDL is therefore achievable only if the reduction in saliva production reaches a threshold where the volume of saliva produced matches or falls below the individual’s capacity to swallow it effectively. On the other hand, after SMDR, the swallowing frequency itself probably increases.”
- Selection bias: “SMDR was contraindicated for patients with inadequate swallowing… leads to a selection of less vulnerable patients with more favorable characteristics to undergo the SMDR procedure.” Thus, the improved results from SMDR over the other techniques is likely related to selection bias, though the authors adjusted the analysis “for differences in cognitive and oral motor functioning.”
My take: Excessive drooling is a common problem in children with neurodevelopmental disabilities. This study provides useful data on surgical management.