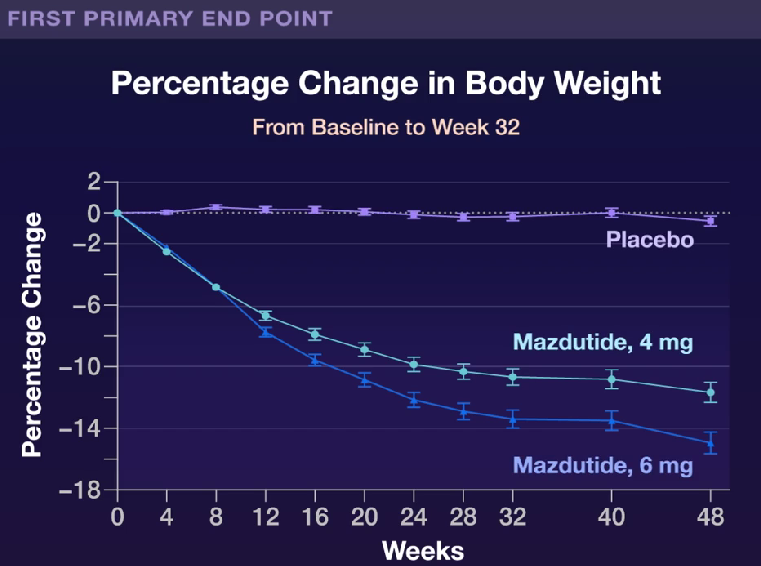
L Ji et al. NEJM 2025; 392: 2215-2225. Once-Weekly Mazdutide in Chinese Adults with Obesity or Overweight
This study from China enrolled young participants (mean age 34 yrs) and lower BMI (mean 31.1) than in similar studies of other GLP1 RAs and GLP 1 RA/GIP dual agonists. However, there was a high prevalence of dyslipidemia (62.3%), MAFLD (48.9%), hyperuricemia (40.2%), and hypertension (22.8%).
Key findings:
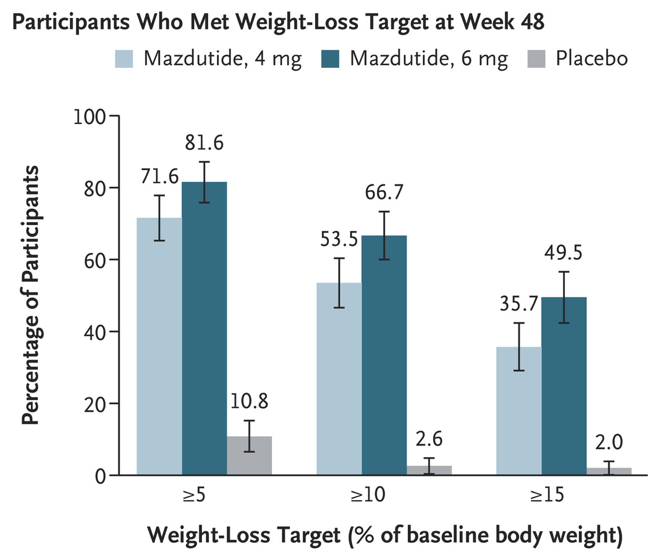
At week 48, the mean percentage change in body weight from baseline was –11.00% in the 4-mg mazdutide group, –14.01% in the 6-mg mazdutide group, and 0.30% in the placebo group
My take: Mazdutide resulted in significant weight loss along with improvements in cardiometabolic measures. This study shows beneficial effects in a younger cohort with significant cardiometabolic disease. Improvements in younger populations is likely to result in more substantial effects on outcomes than improvement in older cohorts.
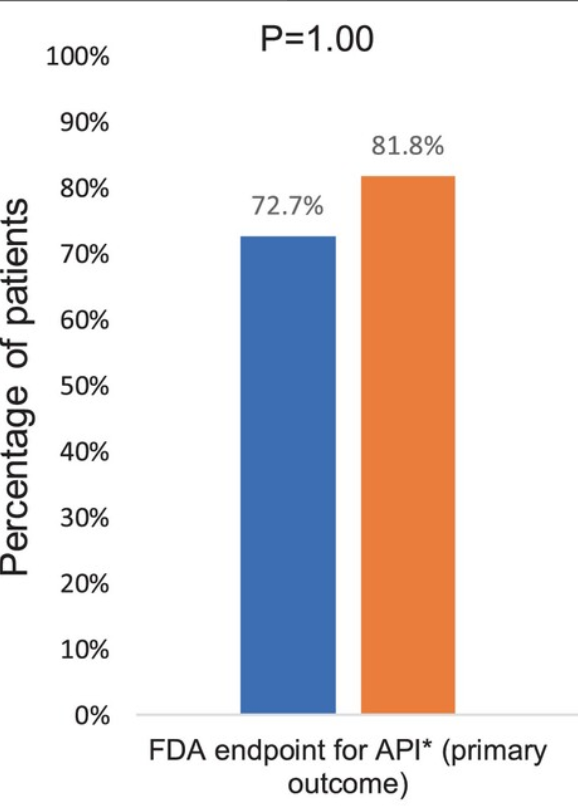
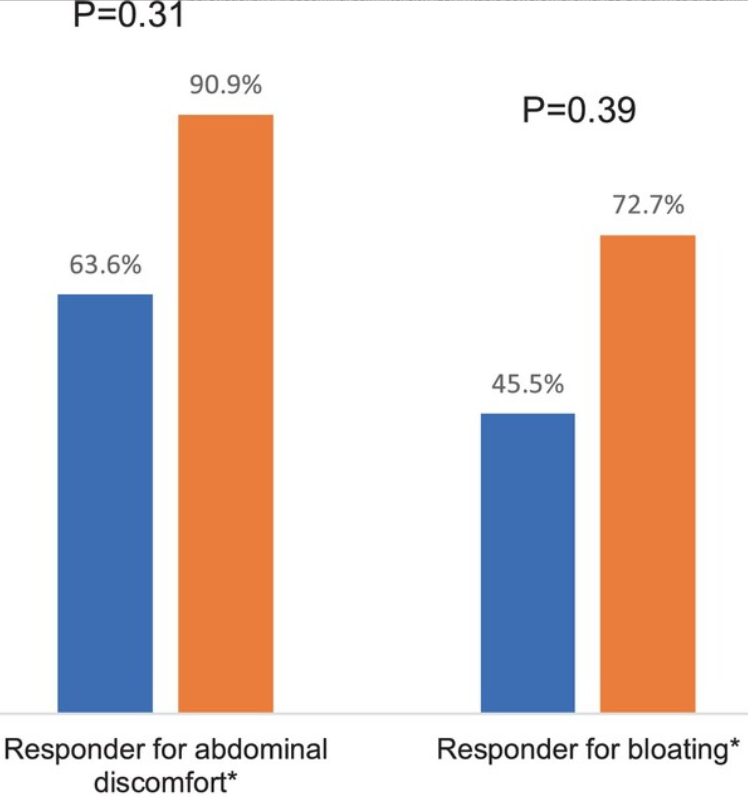
Methods: Patients were randomized controlled trial (RCT), adult patients with diarrhea-predominant IBS (IBS-D) or mixed bowel pattern (IBS-M) were randomized to Mediterranean diet (MD) versus a diet low in fermentable oligo-, di-, monosaccharides, and polyols (LFD) for 4 weeks. 10 patients completed the study in each group. The primary endpoint was the proportion of patients with ≥ 30% decrease in abdominal pain intensity (API) for ≥ 2/4 weeks. Daily variables included abdominal pain intensity (API) and bloating, while IBS symptom severity score (IBS-SSS) and IBS adequate relief (IBS-AR) were scored weekly
Key findings:
73% percent of the MD group met the primary endpoint compared to 81.8% of the LFD group (p = 1.0)
Although not statistically significant, a numerically higher proportion of the LFD group reported adequate relief and met the responder endpoint for IBS-SSS (50-point reduction) compared to the MD group (54.6% vs. 27.3% for IBS-AR and 81.8% vs. 45.5% for IBS-SSS, p = 0.39 and 0.18, respectively)
The LFD group also had a significantly greater reduction in IBS-SSS score over the 4-week treatment period compared to the MD group (−105.5 vs. −60, p = 0.02)
My take (borrowed from authors): A Mediterannean diet “improves abdominal symptoms in the majority of patients with IBS-D and IBS-M. Larger, adequately powered, real-world studies comparing the efficacy of a MD with LFD and NICE diet are needed to validate these preliminary findings and to help patients and providers to know if a MD should be added to the list of effective, evidence-based diet interventions for patients with IBS.”
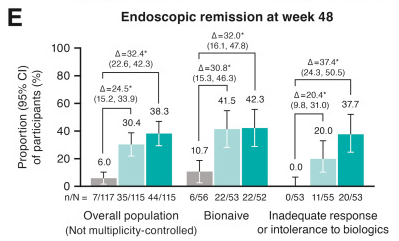
Background: “Guselkumab is a selective dual-acting IL-23p19 subunit inhibitor that potently neutralizes IL-23 by binding to the p19 subunit and to CD64, a receptor on cells that produce IL-23…In the double-blind Phase 2 GALAXI 1 study and the 2 identically designed double-blind Phase 3 GALAXI 2 and GALAXI 3 studies, guselkumab intravenous (IV) induction (200 mg at weeks 0, 4, and 8) followed by subcutaneous (SC) maintenance (200 mg every 4 weeks or 100 mg every 8 weeks) demonstrated efficacy compared with placebo… In addition, guselkumab demonstrated superiority to ustekinumab for multiple endoscopic-based endpoints at week 48 in pooled data from GALAXI 2 and GALAXI 3… The GRAVITI study…evaluated the efficacy and safety of guselkumab SC induction followed by SC maintenance in participants with moderately to severely active Crohn’s disease.
Methods: This was a Phase 3 double-blind, placebo-controlled, treat-through GRAVITI study randomized 347 participants 1:1:1 to guselkumab 400 mg SC every 4 weeks→100 mg SC every 8 weeks (n = 115), guselkumab 400 mg SC every 4 weeks→200 mg SC every 4 weeks (n = 115), or placebo (n = 117). Placebo participants meeting rescue criteria received guselkumab from week 16 onward.
Key Findings:
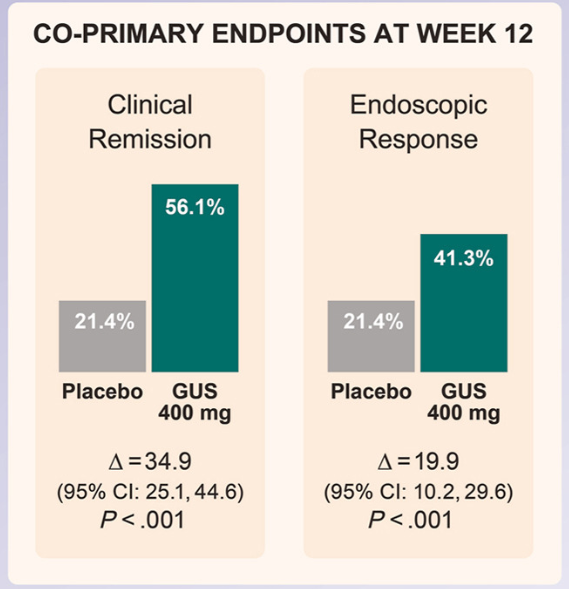
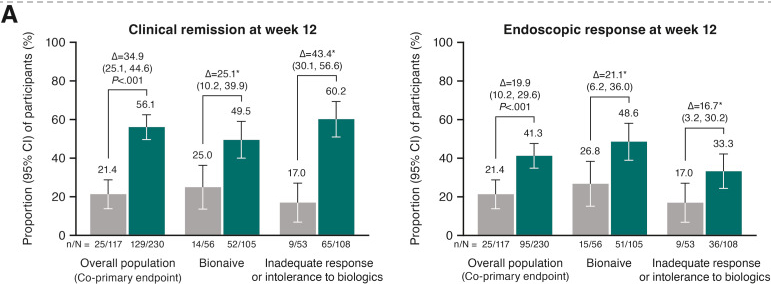
At week 12, significantly greater proportions of participants receiving guselkumab 400 mg achieved clinical remission vs placebo (56.1% vs 21.4%; P < .001), and endoscopic response vs placebo (41.3% vs 21.4%; P < .001)
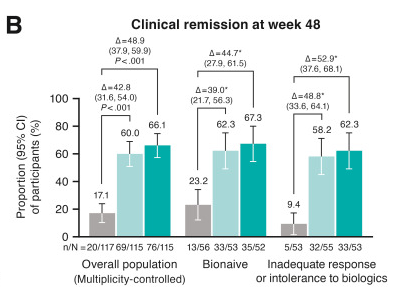
At week 48, significantly greater proportions of participants in both guselkumab groups (100 mg SC every 8 weeks: 60.0%; 200 mg SC every 4 weeks: 66.1%) achieved clinical remission vs placebo (17.1%; P < .001 each) and endoscopic response (44.3%; 51.3%; vs placebo 6.8%; P < .001 each)
Immunogenicity: “Antibodies to guselkumab were detected in 24 (8.8%) of the 274 guselkumab-treated participants through week 48. Only 3 of 274 participants (1.1% of the total population) were positive for neutralizing antibodies. Through week 48, no impact of antibodies to guselkumab on serum guselkumab concentrations, efficacy, or injection-site reactions was observed”
At week 12: Compared to placebo, patients receiving Guselkumab had improved clinical remission and endoscopic response. Being naive to previous biologics was associated with a higher endoscopic response but with a lower clinical remission rate.At week 48: Being naive to previous biologics was associated with a higher clinical remission At week 48: Being naive to previous biologics was associated with a higher endoscopic remission
Discussion: “The results presented here from GRAVITI were consistent with those reported in the double-blind, treat-through GALAXI trials in which guselkumab induction was administered IV in participants with moderately to severely active Crohn’s disease. For example, 41.3% of participants in the GRAVITI study achieved endoscopic response 12 weeks … whereas 36.9% of participants in the pooled GALAXI studies achieved endoscopic response 12 weeks after guselkumab… IV induction (placebo: 12.2%).”
My take: This study shows that Guselkumab with a SC induction is safe and effective in participants with moderately to severely active Crohn’s disease. IV induction does not appear to be needed. Though IL-23 agents have been important advances, there are still a large number of patients without a good response.
Background: “Unlike diagnostic radiology, GI endoscopy requires the concerted efforts of a proceduralist, anesthesiologist, nurse, and technician. Moreover, several of these individuals are often performing tasks that do not involve looking at a monitor. The advent of laparoscopic surgery presented surgeons with similar lighting challenges. In response to this problem, some operating rooms have been equipped with green lights to achieve high contrast and low glare on monitors while still allowing for the safe and efficient practice of other tasks in the operating room. The choice of green light is based on the fact that the human eye is most sensitive to light with a wavelength around 555 nm, in the green portion of the visible spectrum. This wavelength provides optimal contrast and sharpness under low-light conditions.”
Methods: The authors “conducted a single-center cross-over study comparing image classification on video monitors and the performance of multiple nonmonitored based physical tasks in the endoscopy suite using green light and dim light.”
Key findings:
Performance of physical tasks was significantly faster with green light, including endoscopy setup (43.1 vs. 62.1 s), biopsy sample time (35.8 s vs. 80.1 s), and feeding wire (34.3 vs. 99.1 s)
There was no difference in polyp detection rate under the 2 light conditions. However, color detection of anesthesia medication tapes and endoscopic tools was better with dim light.
Eye strain score was significantly better with green light compared with dim light (10.3 vs. 4.1)
My take: Use of green light in endoscopy suites is likely beneficial particularly in more technically-demanding procedures. It makes common tasks easier/quicker and with less eye strain.
(A) Endoscopy suite under green light. (B) Endoscopy suite under low light.
Methods: U-ACTIVATE is an ongoing, 288-week, phase 3, long-term extension study that enrolled patients (n=369) aged 16–75 years with a confirmed diagnosis of moderately to severely active ulcerative colitis; patients who had a clinical response in the induction studies were eligible to enter the U-ACHIEVE maintenance study. Patients not in clinical remission originally randomly assigned to upadacitinib 15 mg were eligible to escalate to upadacitinib 30 mg, those originally randomly assigned to upadacitinib 30 mg continued on upadacitinib 30 mg, and those originally assigned to placebo were eligible to escalate to upadacitinib 15 mg in a masked way
Key findings:
In the as-observed population, 84 (71%) of 118 patients receiving upadacitinib 15 mg were in clinical remission at week 48, as were 130 (67%) of 193 receiving upadacitinib 30 mg
By week 96, 69 (76%) of 91 patients receiving upadacitinib 15 mg and 104 (74%) of 141 of those receiving upadacitinib 30 mg were in clinical remission
The most common adverse events of special interest were hepatic disorder, lymphopenia, creatine phosphokinase elevation, serious infection, neutropenia, and herpes zoster
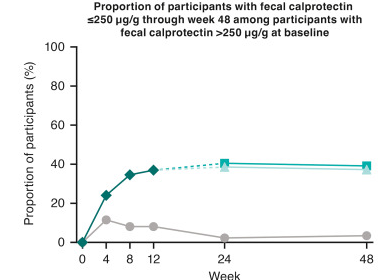
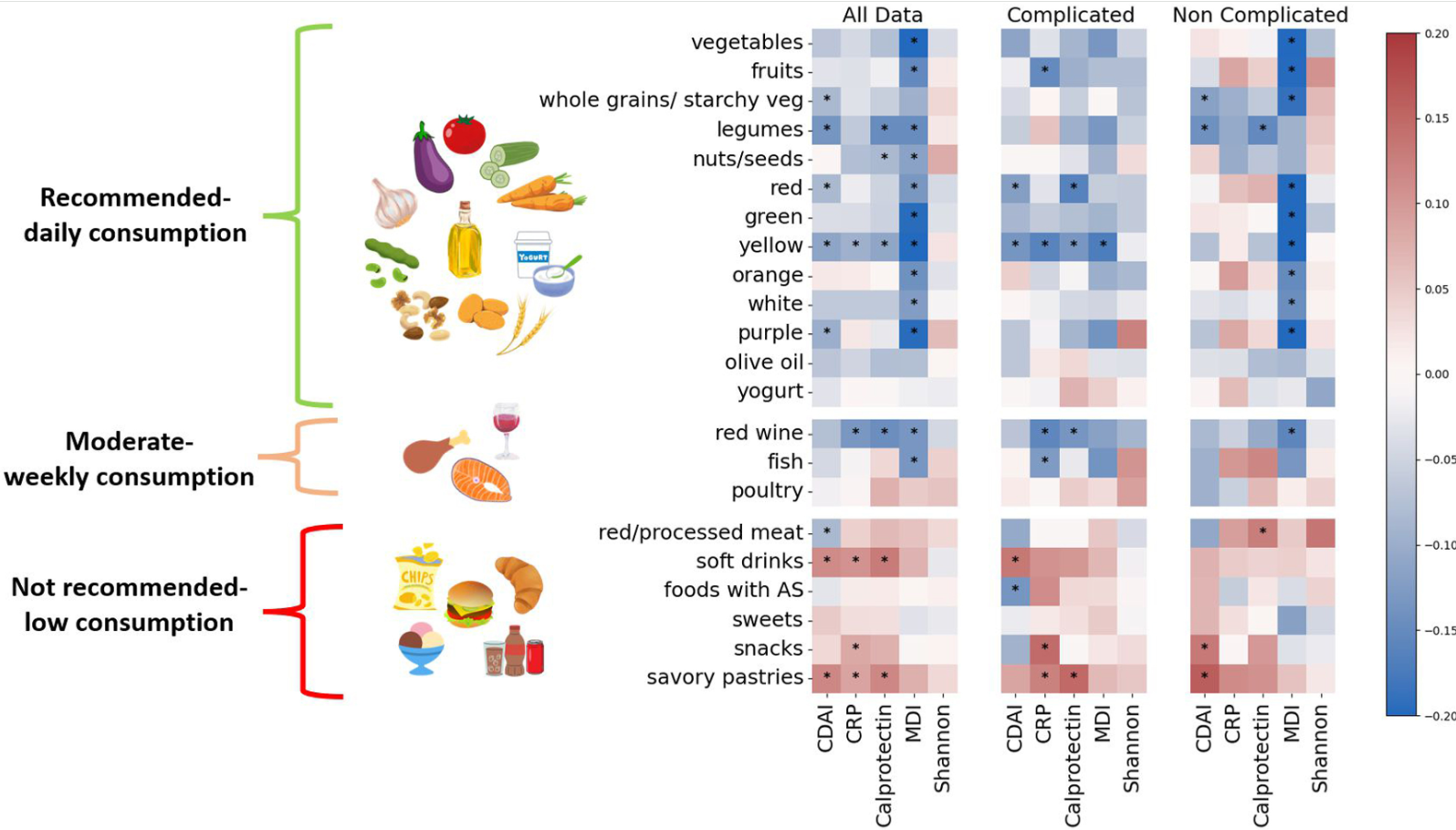
Methods: In this prospective cohort study, consecutive adults (n=271) from 2 large IBD centers in Israel with newly diagnosed CD were recruited and followed prospectively. MED adherence was assessed by repeated food frequency questionnaires (FFQs) using a predefined inflammatory bowel disease Mediterranean diet score (IBDMED score), alongside validated MED adherence screeners. Crohn’s disease activity index (CDAI), C-reactive protein, fecal calprotectin, and microbial composition (16S-ribosomal RNA sequencing) were assessed each visit. Baseline serum and fecal samples were analyzed for targeted quantitative metabolomics.
Demographic/Clinical data indicate 68% received biologics and 40% receiving immunomodulators. 32% received 5-ASA medications (despite lack of proven efficacy)
Key findings:
Adherence to MED was associated with a noncomplicated CD course, and inversely correlated with CDAI, fecal calprotectin, C-reactive protein, and microbial dysbiosis index (all P < .05)
Increasing adherence to MED over time correlated with reduced CDAI and inflammatory markers (P < .05)
Adherence to MED correlated with a beneficial microbial cluster of commensals and short-chain fatty acid producers including Faecalibacterium, and with plant metabolites, vitamin derivatives, and amino acids
Adherence to MED in the cohort group was comparable to the general non-IBD population in Israel
Limitations: This was an observational study rather than an interventional study with a control group. Thus, the results could be influenced by reverse causality
In the associated commentary by Abreu et al, it is noted that in Israel, “MED is more commonplace than in the US and other Western countries…Godny et al found that IBD patients had an average MED adherence score of 7.8, which is similar to that of the general non-IBD population in Israel; in contrast, the average MED adherence score in the US is 4–5.Godny et al’s CD patients consumed an average of 21 g of fiber per day; in a study we just completed, American CD patients consumed less than half that amount.13 Indeed, the baseline diets of American IBD patients are characterized by high amounts of saturated animal fat and almost no fresh fruits and vegetables…Another difference between the Israeli population and the typical American population is body mass index (BMI). The average BMI of patients in this study was 21.9 kg/m2 (interquartile range 20–25.3 kg/m2). This contrasts with the average BMI of the general US population of 30 kg/m2.”
My take: This study shows an association between MED diet and better outcomes/less complications in adults with Crohn’s disease. Eating a good diet is an important part of treatment.
Additional notes on dietary scores: “The IBDMED screener positively scored high consumption of MED-recommended dietary components such as fruits, vegetables, olive oil, legumes, nuts and seeds, and fish. It also positively scored low consumption of MED non-recommended dietary components such as red and processed meat, soft drinks, and sweets. To this we added several dietary features based on previous data associated with microbial composition and function. These included a positive score for plant diversity27 by scoring for different colors in the diet, consumption of fermented foods28 (specifically yogurt), and inclusion of starchy vegetables like potato in the whole grain category to promote diversity in the carbohydrate-rich food group, as well as support butyrate producers as we had previously shown.29 In addition, we aimed to positively score for relatively low UPF intake. To this end, we evaluated the average intake of sweets, snacks, sweet and savory pastries, soft drinks, and foods and drinks containing artificial sweeteners.”
Also, from Kim Beall, Cofounder and Managing Director of Nutritional Therapy for IBD:
“If you haven’t been to the website recently, we have expanded the recipe database to over 1,000 recipes with many filterable aspects and we’ve just released a new nutrition tool, the IBD Nutrition Navigator to facilitate nutrition conversations between providers and patients to find the right nutritional starting point. This is a project led by Dr. Ananthakrishnan and a dedicated team of pediatric and adult medical advisors in a two year long development process. Many have told us this is a useful tool particularly for those less familiar with nutrition in IBD. We’re excited about it’s potential to integrate nutrition in practice, with “an option for every patient”. We appreciate your support in sharing our information, tools, and resources to advance IBD nutrition care.” Here’s the link to their website:
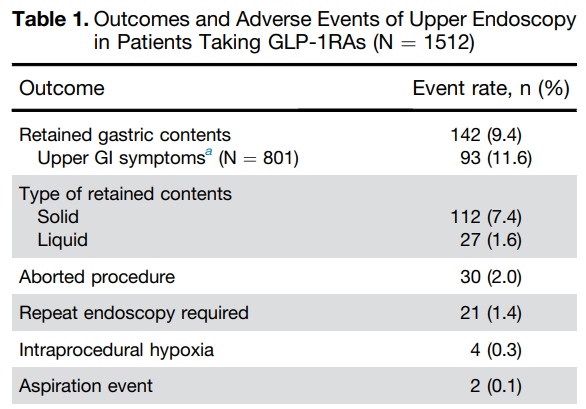
This is one of three articles discussing the issue of GLP-1RAs and potential complications with upper endoscopy. Faccisourruso et al performed a meta-analysis that included 13 studies (of 177 studies) involving a total of 84,065 patients.
Rates of aborted and repeated procedures were higher in the GLP-1RA user group. The absolute risk of aborted procedure was 1% in GLP-1RA users compared to 0.3% in non-users. The absolute risk of a repeated procedure was 2% vs 1% respectively.
No significant differences were found in AE and aspiration rates between the 2 groups (OR, 4.04 and OR, 1.75 respectively). The absolute risk of aspiration was 0.3% in GLP1-RA users compared to 0.2% in non-GLP1-RA group
Adverse events were higher in GLP-1RA users (0.3%) compared to non-users (0.1%)
In their discussion, the authors note that an “individualized approach based on the indication of GLP-1RA use (withholding the drug in patients with diabetes could lead to more harm)…a potential stragegy could be to place patients on a liquid diet the day before endoscopy, thus prolonging the duration of fasting for solid for at least 12 hours.”
My take: The totality of these studies confirms the increased risk of retained gastric contents in patients receiving GLP-1RAs. This in turn increases the need to abort/reschedule cases and may result in very a low increased risk of aspiration. To mitigate this risk, it may be sufficient to implement a liquid diet the day before endoscopy (avoiding solid foods for at least 12 hours prior to endoscopy). This is in agreement with the recent AGA Rapid Clinical Practice Update (see post below).
“Like millions of others, I was caught between what the food industry has done to make the American diet unhealthy and addictive and what my metabolism could accommodate.
We may now be at the brink of reclaiming our health. New and highly effective anti-obesity medications known as GLP-1s have revolutionized our understanding of weight loss and of obesity itself. These drugs alone are not a panacea for the obesity crisis that has engulfed the nation, and we should not mistake them for one. But their effectiveness underscores the fact that being overweight or obese was never the result of a lack of willpower…
GLP-1s are revolutionary drugs that can drastically reduce caloric intake and improve health in a way I didn’t expect I would ever see. Now we need to complete that revolution by taking on the food industry and its engineered foods that are contributing to some of the most harmful health issues America faces today.”
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
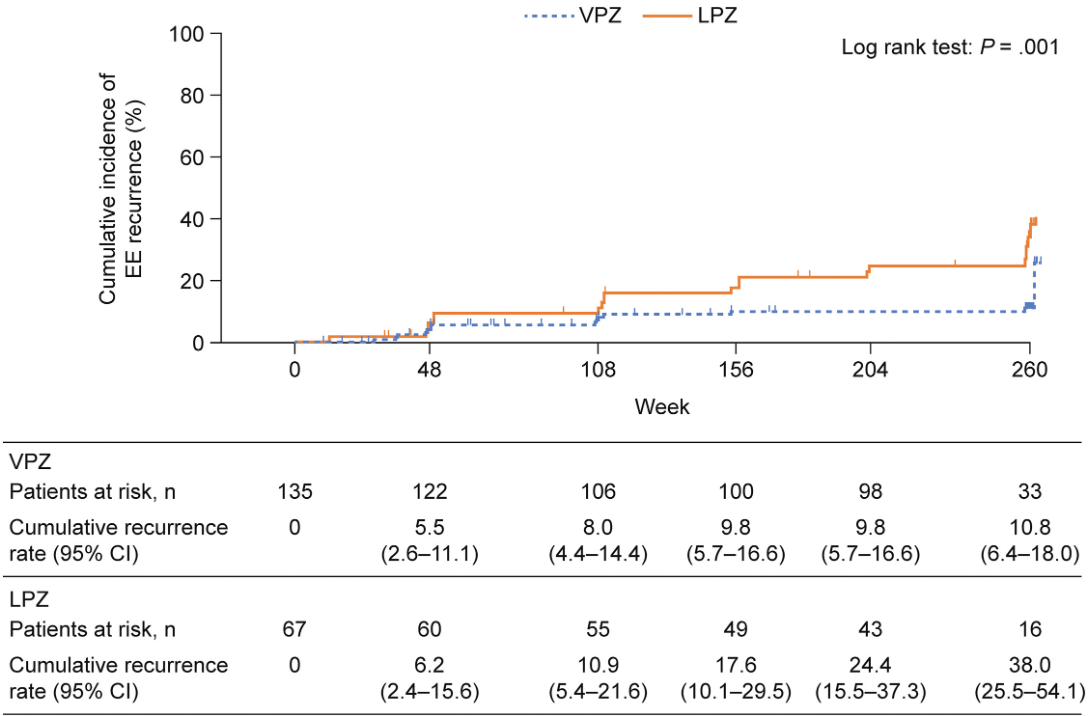
Background: Potassium-competitive acid blockers, such as vonoprazan, provide more potent gastric acid suppression than proton pump inhibitors. However, long-term safety data are lacking for vonoprazan in patients with healed erosive esophagitis. This study with 208 patients provides long-term data on the use of a vonoprazan.
Methods: Open-label study. Patients with erosive esophagitis (EE) received induction therapy (once daily vonoprazan 20 mg or lansoprazole 30 mg; ≤8 weeks). Those with healed EE received maintenance therapy (once daily vonoprazan 10 mg or lansoprazole 15 mg) for 260 weeks (2:1).
Key findings–Adverse effects:
No malignant alterations or gastric neuroendocrine tumors (NETs) were observed; there was 1 adenoma in each group
At week 260, significantly more patients taking vonoprazan vs lansoprazole had parietal cell hyperplasia (97.1% vs 86.5%) and foveolar hyperplasia (14.7% vs 1.9%)
proportions of patients with ECL cell hyperplasia (4.9% vs 7.7%) and G-cell hyperplasia (85.3% vs 76.9%) were similar
Median serum gastrin levels were higher with vonoprazan treatment vs lansoprazole (625 pg/mL vs 200 pg/mL)
Key finding –Efficacy:
Overall, the cumulative EE recurrence over 260 weeks was lower in the vonoprazan group (10.8% ) vs the lansoprazole group (38.0%) (P = .001)
Discussion Points:
“Annual endoscopies and biopsies performed in the VISION study are considered objective approaches for detecting upper gastrointestinal diseases and variable lesions, as well as gastric mucosa morphological changes in areas without endoscopically apparent lesions…Although the proportions of patients with parietal cell protrusion and foveolar hyperplasia were higher in the vonoprazan group than in the lansoprazole group over 5 years, the clinical significance of these findings is unclear.”
“The safety profiles of vonoprazan and lansoprazole were also comparable, suggesting that long-term use of vonoprazan is as safe as PPIs.”
My take: This study provides some reassurance regarding the risk of using vonoprazan & other potassium-competitive acid blockers. The benefits of controlling erosive esophagitis may outweigh potential safety risks of long-term use. Nevertheless, it will be a while before this class of medications is used extensively in the pediatric age group.
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
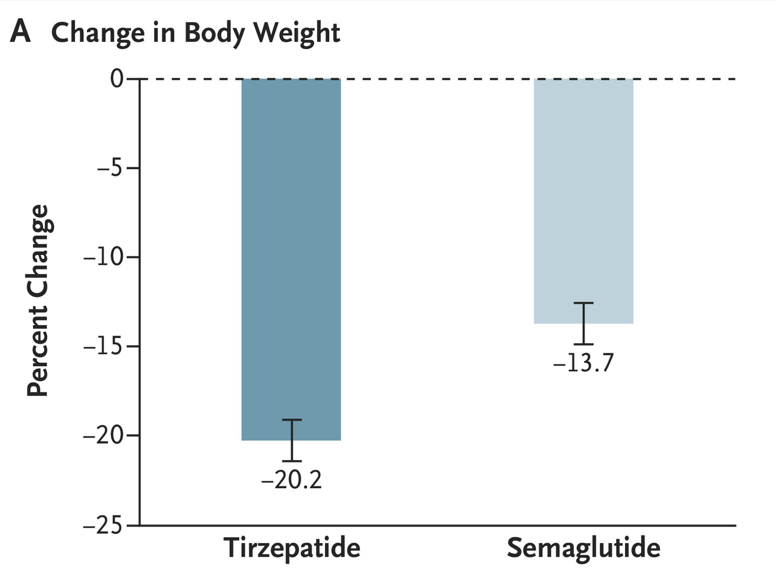
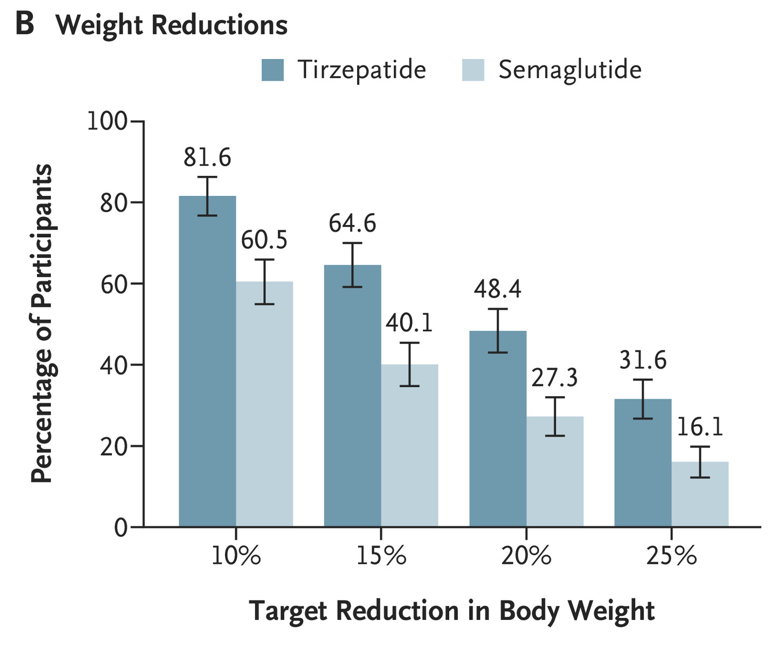
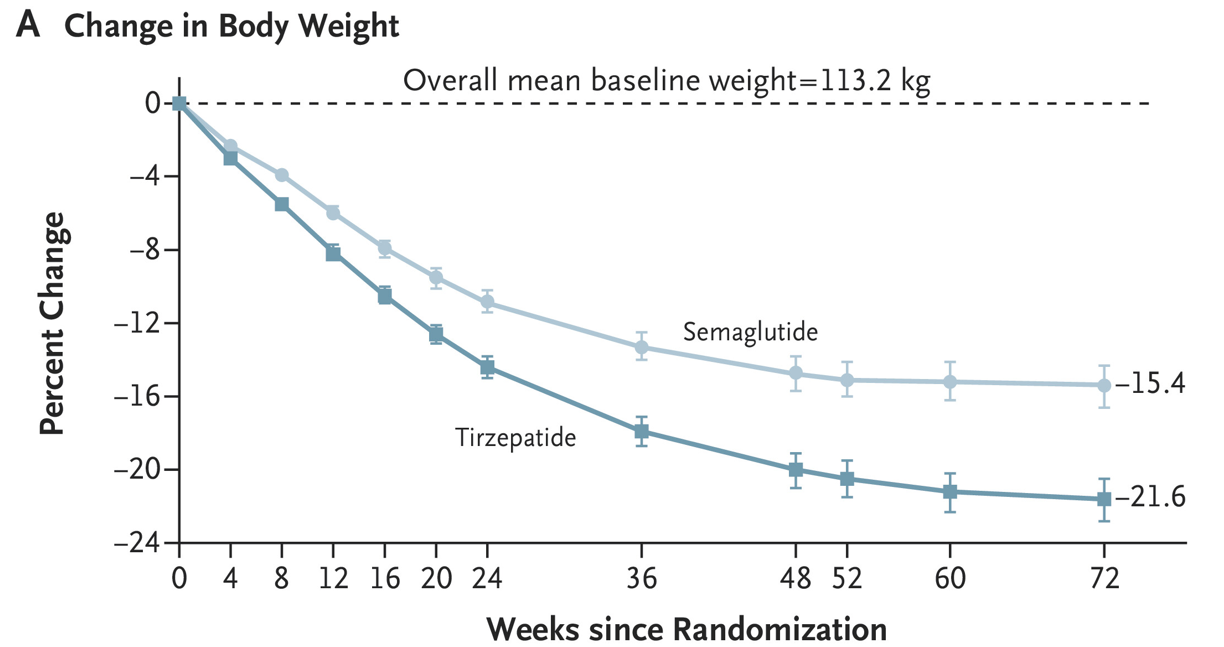
LA Aronne et al. NEJM 2025; DOI: 10.1056/NEJMoa2416394. Tirzepatide as Compared with Semaglutide for the Treatment of Obesity
Methods: In this phase 3b, open-label, controlled “SURMOUNT-5” trial, adult participants (n=751) with obesity but without type 2 diabetes were randomly assigned in a 1:1 ratio to receive the maximum tolerated dose of tirzepatide (10 mg or 15 mg) or the maximum tolerated dose of semaglutide (1.7 mg or 2.4 mg) subcutaneously once weekly for 72 weeks
Key findings:
Discussion Points:
“With both treatments in our trial, as weight reduction increased, greater improvements occurred in cardiometabolic risk factors, including blood pressure, glycemia, and lipid levels, which is consistent with the findings in previous reports.17 The mean differences between tirzepatide and semaglutide in the cardiometabolic risk factors may be clinically relevant considering that reductions in systolic blood pressure of 2 to 5 mm Hg have been shown to reduce the risk of cardiovascular events.”
” As typically observed with incretin-based therapies, gastrointestinal adverse events were predominantly mild to moderate in severity, occurred mostly during dose escalation, and led to treatment discontinuation more often with semaglutide than with tirzepatide.”
My take (borrowed from the authors): “Treatment with tirzepatide, a dual GIP and GLP-1 receptor agonist, was superior to treatment with semaglutide, a selective GLP-1 receptor agonist, with respect to reduction in body weight and waist circumference.”
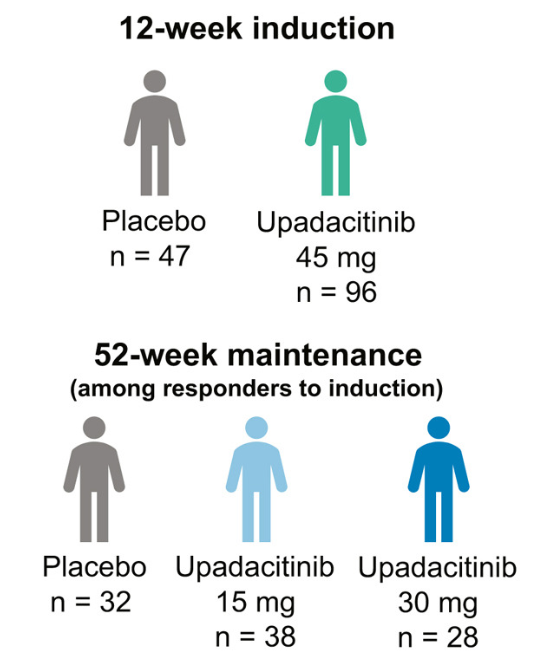
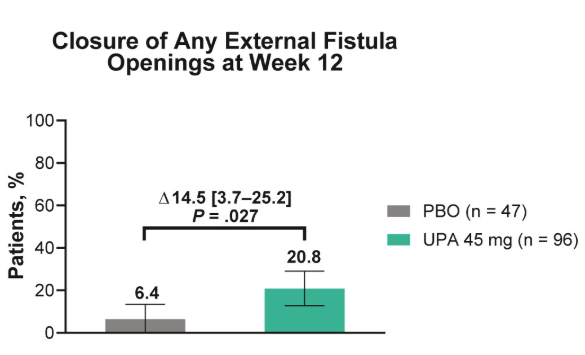
Methods: This post hoc analysis evaluated upadacitinib outcomes in patients with fistulizing disease in the following studies: phase 3 induction (U-EXCEL, U-EXCEED) and maintenance (U-ENDURE) trials. It was noted that there were 1021 patients in U-EXCEL and U-EXCEED; 143 (14.0%) had any fistulas at baseline (66 draining). Most (n = 128) had perianal fistulas (56 draining).
Key findings:
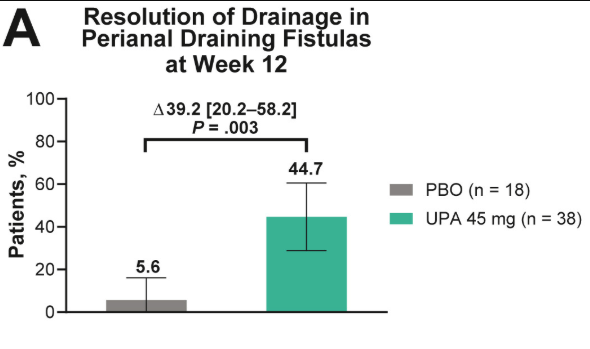
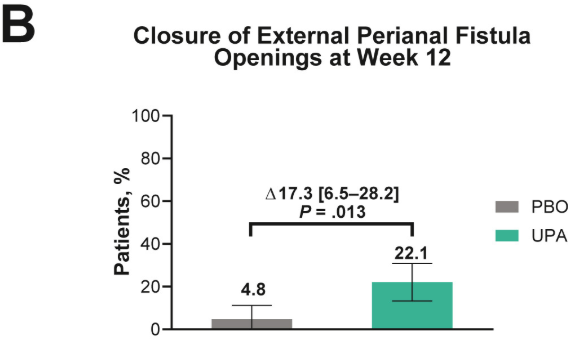
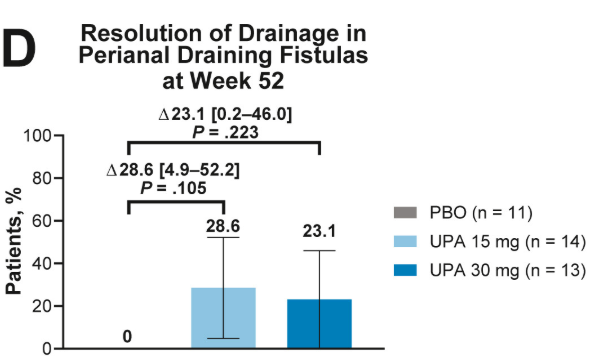
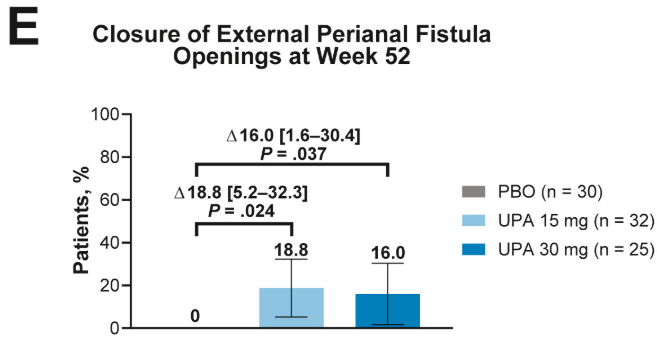
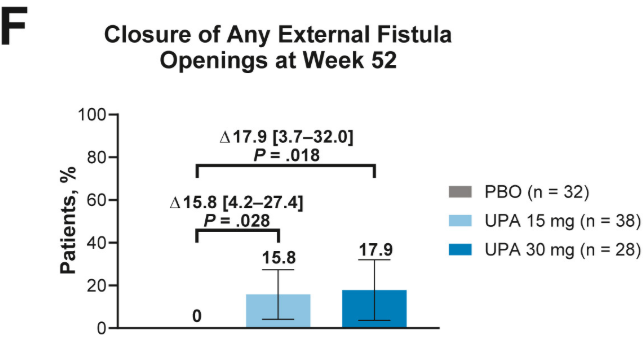
Fistulizing disease (primarily perianal) treated with upadacitinib achieved higher rates of resolution of drainage, closure of external openings, clinical remission, and endoscopic response vs placebo
These slides from Figure 1 show the resolution of drainage in perianal draining fistulas, closure of external perianal fistula openings, and closure of external openings for any fistula at week 12 of the induction trials and week 52 of the maintenance trial.
Discussion points:
Patients with draining fistulas often experience higher disease burden
Most patients in U-EXCEL and U-EXCEED had failed at least 2 prior biologic treatments (which often included anti-TNF therapy), reflecting a more refractory and difficult-to-treat population in CD
Despite the presence of perianal disease, patients with fistulizing CD treated with upadacitinib showed concurrent improvements in CD symptoms (CDAI, SF, and APS), luminal disease (endoscopic response and SES-CD), and markers of inflammation
My take: This study shows that upadacitinib is more effective than placebo; however, the majority of patients continued with ongoing perianal disease.