ECF Brown. NEJM 2025; 393; 1-3. Defining Health Care “Corporatization”
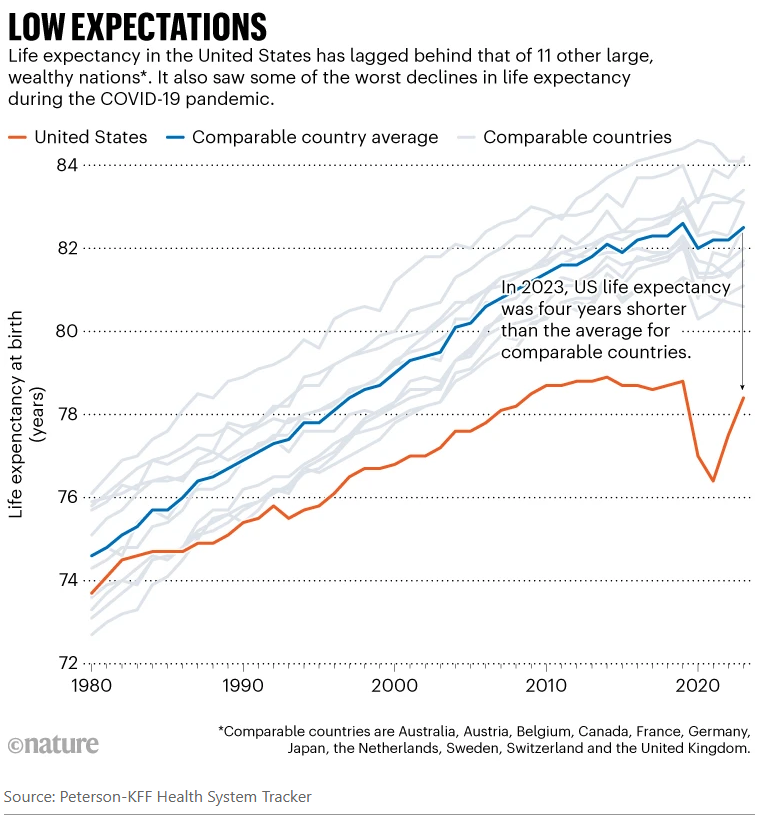
This blog has had many posts detailing the many flaws in the U.S. health care system. While the U.S. expends more per capita than any other country, our life expectancy is 4 years less than similar countries in Europe and Canada.
This article in the NEJM is the first of a series examining the ‘corporatization’ of health care and potential ways to improve health care delivery.
Excerpts:
The percentage of hospitals owned by companies controlling three or more hospitals increased from 11.6% in the 1980s to 56.1% today…and now nine megahospital chains own more than 50 hospitals each.
In the early 1980s, three quarters of U.S. physicians owned their practice, whereas in 2023 a similar proportion of physicians was employed by hospitals or corporate entities, including private equity funds.
Insurance conglomerates, such as UnitedHealthcare and CVS–Aetna, now control physicians, home care, pharmacies, and pharmacy benefit managers (PBMs). Horizontal hospital consolidation has been pursued for the promise of economies of scale and market power…
The term “corporatization” now refers to the general trend throughout the health care industry toward higher levels of integrated control by consolidated profit-seeking enterprises… First is the elevation of profit generation as the primary goal of the health care enterprise…the primary duty of the corporation is to maximize shareholder profits. Shareholder primacy subordinates the interests of other stakeholders, such as patients, the health care workforce, or the community…
Even nonprofit hospitals can become corporatized as they grow in size and organizational scale…powerful nonprofit health systems may come to prioritize revenue over patient and community welfare, evidenced by inflated prices, insurance network exclusions, medical debt–collection actions against patients, facility closures in low-income areas, and cuts to staffing levels and pay.
The second key element of corporatization is consolidation… Conglomerates’ market dominance, diversification across platforms, and change in locus of control insulate them from reputational or market discipline…
Corporatization has produced a system that is incredibly profitable for investors but increasingly unaffordable, inaccessible, and uncaring for everyone else — in other words, it has created a Gilded Age of medicine.5 …Corporate control over medical practices and the drive for profit have undermined many clinicians’ professionalism, autonomy, trust, and morale…
Traditional health policy interventions such as antitrust enforcement, tax subsidies and exemptions, prohibitions on the corporate practice of medicine, and payment reforms have not stopped the rise of the corporation in health care, owing to lax enforcement, political capture, and sophisticated regulatory workarounds…
Confronting corporatization may require a fundamental reorientation of the industrial organization of the health system… Future health policy efforts must confront the fundamental question of whom our health care system is meant to serve: corporate giants or the members of our society as a whole.
Related blog posts:
- “Commercial Insurance Isn’t in the Health Care Business. It’s in the Financial Business.”
- How Insurance Companies Save Millions in Denying Care
- Stopping Insurance Coverage in the Middle of Your Procedure
- Longevity Gap Present Even in Wealthy Americans
- Ten Americas: Examining Health Disparities and Life Expectancy
- The Guardian: UnitedHealth Secretly Paid Nursing Homes to Reduce Hospital Transfers
- “Proposed Medicaid Cuts Could Lead to Thousands of Preventable Deaths Annually” & Personal Message
- How Putting America First is Undermining Health Outcomes Here and Globally
- How to Successfully Appeal Health Insurance Denials
- “Denials, Dilly-dallying and Despair” This post has a lot of useful information on practical steps to appeal denials.
- NY Times: ‘What’s My Life Worth?’ The Big Business of Denying Medical Care
- High Rates of Denying Medical Care for Medicaid Patients Managed by Health Insurers
- Mark Cuban: Disrupting American Healthcare
- High Rates of Denying Medical Care for Medicaid Patients Managed by Health Insurers
- Another Health Insurance Predatory Practice and One Doctor’s Quest to Stop It
- How Insurance Companies Betray Their Policy Holders in Dealing with Out-of-Network Physicians
- Choosing Health Insurance -Humor
- “Health Insurance Is Broken” | gutsandgrowth
- Healthcare: “Where the Frauds Are Legal”
- No One Would Design U.S. Healthcare System This Way
- NY Times: America can afford a world-class health system. Why don’t we have one?
- We are Last in Health Care Among High Income Countries
- The Failing U.S. Health System