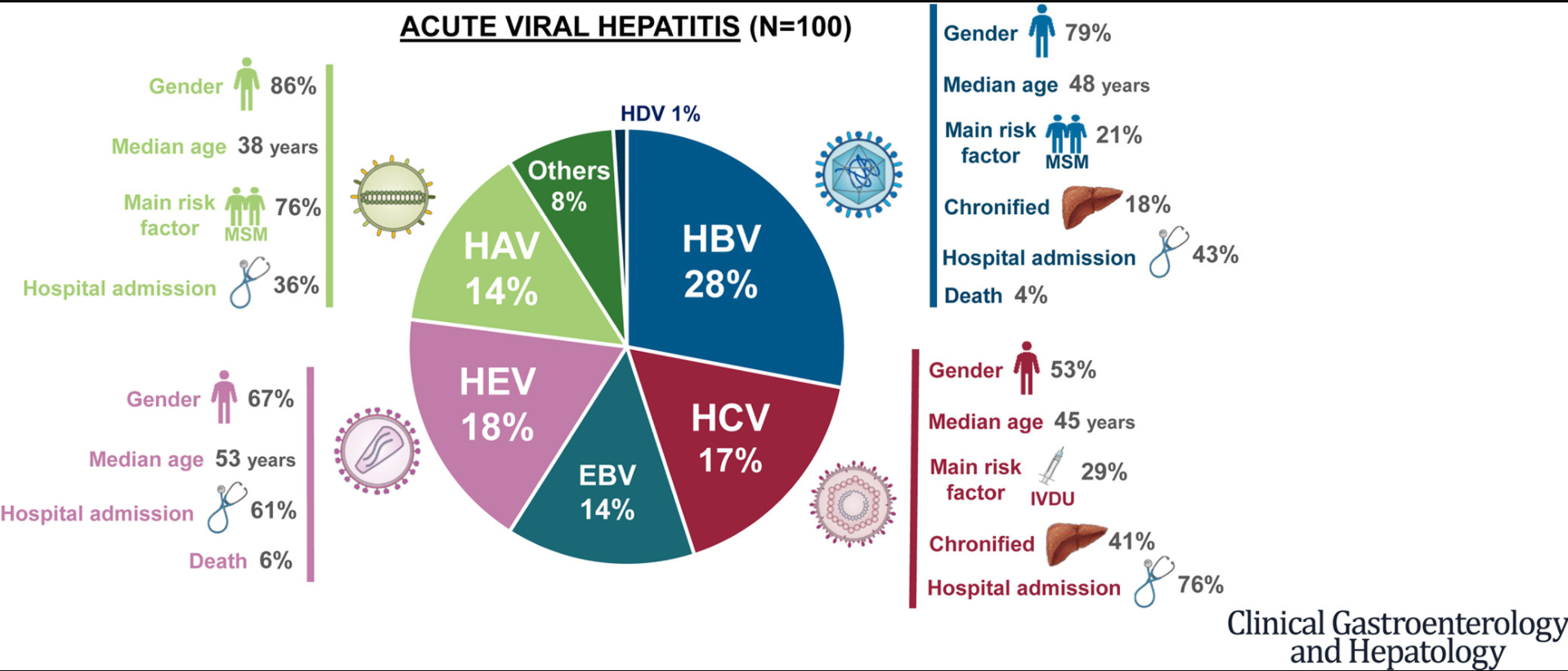
This prospective study of adults collected data from an emergency room of an academic hospital in Barcelona (2014-2018).
Key findings:
The most common etiologies of acute hepatitis were HBV infection (28%), HEV infection (18%), HCV infection (17%), and HAV infection (14%)
Approximately one-third of acute hepatitis cases were in immigrants
The main risk factors of the cohort were sexual risk contact and intravenous drug use; 79% of cases of HAV had sexual risk behavior
Chronic infections developed in 5/28 patients (18%) with acute HBV infection and 7/17 patients (41%) with acute HCV infection
The graphical abstract breaks down features for the most common etiologies: HBV (blue) 28%, HEV (purple-pink) 18%, HCV (maroon) 17%, and HAV (light green) 14%.
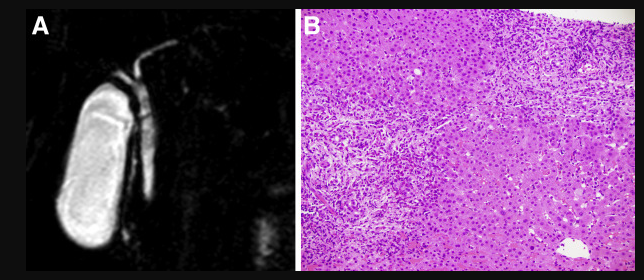
Methods: The authors would utilize livers from donors with hepatitis C if they had a “normal gross appearance or, in cases in which a liver biopsy was indicated, acceptable histology less than grade 2 inflammation and less than stage 2 fibrosis (Batts-Ludwig classification)”
Key findings:
292 patients, 61 rHCV− received DNAT+ livers (study group), and 231 rHCV− received DNAT− (aviremic donors [nuclear acid test‐negative donors]) (2018-2019)
1‐year post‐LT patient and graft survival were similar between groups
In the study group, 4 patients died, and 1 patient required retransplantation within the first year post‐LT (all unrelated to HCV)
51 patients completed DAA treatment, all achieving sustained virologic response for 12 or more weeks (SVR‐12) (one required re-treatment)
Given the limited organ availability, using livers from donors with hepatitis C has the potential to reduce waitlist times and waitlist mortality.
My take: Liver transplantation with hepatitis C has become bidirectional; livers are being received by those with liver failure due to hepatitis C and failed livers are being replaced by donors infected with hepatitis C.
It is well-recognized that obesity/overweight increases the risk of cancer (related blog post: Cancer due to Overweight/Obesity). Wang et al provide data regarding cancer risk due specifically to nonalcoholic fatty liver disease (NAFLD) from a large prospective adult cohort (n=54,187). Key findings:
Prevalence of NAFLD, based on ultrasonography, was 32.3%.
NAFLD was associated with increased risk of all cancers (hazard ratio [HR], 1.22; 95% CI, 1.10–1.36; P = .0001), thyroid cancer (HR, 2.79; 95% CI, 1.25–6.21; P = .01), and lung cancer (HR, 1.23; 95% CI, 1.02–1.49; P = .03).
Increased risk for colorectal cancer (HR, 1.96) and lung cancer (HR, 1.38) was demonstrated only in smokers. An association between NAFLD and kidney cancer (HR, 1.57; 95% CI, 1.03–2.40) was only observed in men without diabetes.
Risk of hepatocellular carcinoma was increased only in those with elevated ALT values of 80 U/L or more (HR 8.08)
My take: This study shows that NAFLD increases the risk of cancer; much of this risk may be due to obesity/metabolic syndrome and associated chronic inflammation. Overall, cardiovascular disease in patients with NAFLD represents a higher risk for morbidity and mortality.
Background: Nonanastomotic biliary strictures are a major complication after liver transplantation, and ischemia–reperfusion injury is a key mechanism in their development. Although static cold preservation provides some protection against injury, preclinical studies have shown that a short period of hypothermic oxygenated machine perfusion restores mitochondrial function and reduces damage.
Methods: In this multicenter, controlled trial, we randomly assigned patients who were undergoing transplantation of a liver obtained from a donor after circulatory death to receive that liver either after hypothermic oxygenated machine perfusion (machine-perfusion group) or after conventional static cold storage alone (control group). A total of 160 patients were enrolled, of whom 78 received a machine-perfused liver and 78 received a liver after static cold storage only (4 patients did not receive a liver in this trial).
Key points:
Nonanastomotic biliary strictures occurred in 6% of the patients in the machine-perfusion group and in 18% of those in the control group, risk ratio, 0.36
Postreperfusion syndrome occurred in 12% of the recipients of a machine-perfused liver and in 27% of those in the control group; risk ratio, 0.43
Early allograft dysfunction occurred in 26% of the machine-perfused livers, as compared with 40% of control livers; risk ratio, 0.61
My take: Hypothermic oxygenated machine perfusion led to lower risk of nonanastomotic biliary strictures
In his book, Critical path, Buckminster Fuller (Fuller 1981), American architect, systems theorist, author, designer, inventor, and futurist, created the ‘knowledge doubling curve’. He noticed that until 1900 human knowledge doubled approximately every century and by the end of World War II knowledge was doubling every 25 years (Knowledge is not everything, Paul Chamberlain). Now the doubling of knowledge, in the age of the internet and social media, has become even shorter, perhaps less than a year.
I was thinking about this knowledge doubling curve after reading two practice guidances in a recent issue of Hepatology:
The first guidance is mainly for reference as pediatric gastroenterologists do not focus on reproductive health. The authors do provide guidance on contraceptive options which is an important topic for adolescents. The main guidance is disease-specific information for pregnancy in the setting of underlying liver conditions including liver transplantation, cirrhosis, viral hepatitis, autoimmune hepatitis, PSC, PBC, Wilson’s disease, hepatitis C, nonalcoholic fatty liver disease, HELLP, acute fatty liver disease of pregnancy, Budd-Chiari, FNH, hepatocellular adenoma, and others. The guidance also provides recommendations for how to evaluate abnormal liver tests in pregnancy and reviews liver medications during pregnancy (Table 4).
The second guidance reviews the following:
An overview of the current understanding of bleeding and thrombosis in cirrhosis.
An evidence‐based justification for bleeding risk assessment in patients with cirrhosis before invasive procedures, including current concepts in preprocedural testing and laboratory analysis and their role in predicting bleeding complications.
An outline of established and recently identified risk factors for venous thrombosis in the portal and hepatic venous systems in both patients with and without cirrhosis along with thrombophilia testing recommendations.
A review of the strengths and weaknesses of the various classification systems for portal vein thrombosis and a proposal for standard nomenclature regarding characterization of portal vein thrombosis location, time course, and progression.
Useful points:
In patients with cirrhosis, there are “complex hemostatic changes that are not adequately captured by traditional laboratory measures of hemostasis, such as PT, aPTT, and platelet count.”
“Because of conflicting data in the literature, there is no data-driven specific INR or platelet cut-off in which procedural bleeding risk is reliable increased.” In some studies, the authors conclude that “that the low platelet count may have been merely a reflection of advanced portal hypertension and not a causative risk factor for bleeding.”
For Platelets in the setting of cirrhosis: “Given the low risk of bleeding of many common procedures, potential risks of platelet transfusion, lack of evidence that elevating the platelet count reduces bleeding risk, and ability to use effective interventions, including transfusion and hemostasis if bleeding occurs, it is reasonable to perform both low‐ and high‐risk procedures without prophylactically correcting the platelet count...An individualized approach to patients with severe thrombocytopenia before procedures is recommended because of the lack of definitive evidence for safety and efficacy of interventions intended to increase platelet counts in patients with cirrhosis.” The authors note in Table 4, that the AASLD does not have a specific threshold for platelets, whereas other societies have used values of >30 or >50.
For INR in setting of cirrhosis: “The INR should not be used to gauge procedural bleeding risk in patients with cirrhosis who are not taking vitamin K antagonists (VKAs)…Measures aimed at reducing the INR are not recommended before procedures in patients with cirrhosis who are not taking VKAs…FFP transfusion before procedures is associated with risks and no proven benefits.”
The guidance lists a step‐by‐step treatment and surveillance algorithm for portal vein thrombosis in patients with cirrhosis (and without cirrhosis).
The guidance provides updated diagnostic, treatment, and management recommendations for sinusoidal obstruction syndrome (formerly known as hepatic-veno-occlusive disease), hereditary hemorrhagic telangiectasia, and hepatic vein thrombosis (aka Budd-Chiari).
Classification and management recommendations for idiopathic noncirrhotic portal hypertension and the portosinusoidal vascular disorders.
Surveillance and evaluation recommendations for hepatic and splenic artery aneurysms.
A review of the management issues in vascular liver disorders specific to children and guidance on early intervention in extrahepatic portal vein obstruction in children.
My take: In essence, these two articles are condensed textbooks. The first on Liver Disease, Pregnancy and Reproductive Health. And the second on Bleeding in the Setting of Chronic Liver Disease and Vascular Liver Diseases.
Methods: This was a a 72-week, double-blind phase 2 trial involving patients with biopsy-confirmed NASH and liver fibrosis of stage F1, F2, or F3. Patients were randomly assigned, in a 3:3:3:1:1:1 ratio, to receive once-daily subcutaneous semaglutide at a dose of 0.1, 0.2, or 0.4 mg or corresponding placebo.
Key findings:
The percentage of patients in whom NASH resolution was achieved with no worsening of fibrosis was 40% in the 0.1-mg group, 36% in the 0.2-mg group, 59% in the 0.4-mg group, and 17% in the placebo group (P<0.001 for semaglutide 0.4 mg vs. placebo).
An improvement in fibrosis stage occurred in 43% of the patients in the 0.4-mg group and in 33% of the patients in the placebo group (P=0.48).
The mean percent weight loss was 13% in the 0.4-mg group and 1% in the placebo group.
Safety: Malignant neoplasms were reported in 3 patients who received semaglutide (1%) and in no patients who received placebo. Overall, neoplasms (benign, malignant, or unspecified) were reported in 15% of the patients in the semaglutide groups and in 8% in the placebo group
Clearly this study indicates that there may be safety concerns with semaglutide. In addition to the malignant neoplasms, there were 8 individuals with colonic polyps in the treatment groups and 7 with renal cysts in the treatment group. However, the authors note that in a recent meta-analysis with 55,921 patients, GLP-1 agonists were not associated with an increased risk of malignant neoplasms (Diabetes Obes Metab 2020; 22: 699-704).
Related article: JPH Wilding et al. NEJM 2021; 384: 989-1002. Once-Weekly Semaglutide in Adults with Overweight or ObesityKey finding: The mean change in body weight from baseline to week 68 was −14.9% in the semaglutide group as compared with −2.4% with placebo. This study indicates potential for GLP-1 Agonist class for pharmacologic treatment of obesity.
My take: The improvement in NASH with semaglutide is encouraging and perhaps improvement in fibrosis will occur with more time. Yet, more time is also needed to determine if this agent is truly safe in this population. In patients receiving other GLP analogues, vigilance for adverse events is needed as well.
This was a population-based prospective study from Canterbury, New Zealand
Key findings:
Overall incidence rates were 1.93 per 100,000 for AIH (95% CI, 1.58–2.34), 0.51 per 100,000 for PBC (95% CI, 0.33–0.73), and 0.92 per 100,000 for PSC (95% CI, 0.68–1.21).
The incidence rateof AIH was significantly higher during the period of 2014–2016 (2.39 per 100,000; 95% CI, 1.76–3.23) than during the period of 2008–2010 (1.37 per 100,000; 95% CI, 0.91– 2.06) (P < .05). Incidences of PBC and PSC did not change significantly.
In 2016, prevalence values were 27.4 per 100,000 for AIH (95% CI, 23.58–32.0), 9.33 per 100,000 for PBC (95% CI, 7.13–12.05), and 13.17 per 100,000 for PSC (95% CI, 10.56–16.42).
My take: This study indicates that autoimmune hepatitis has been increasing in incidence.
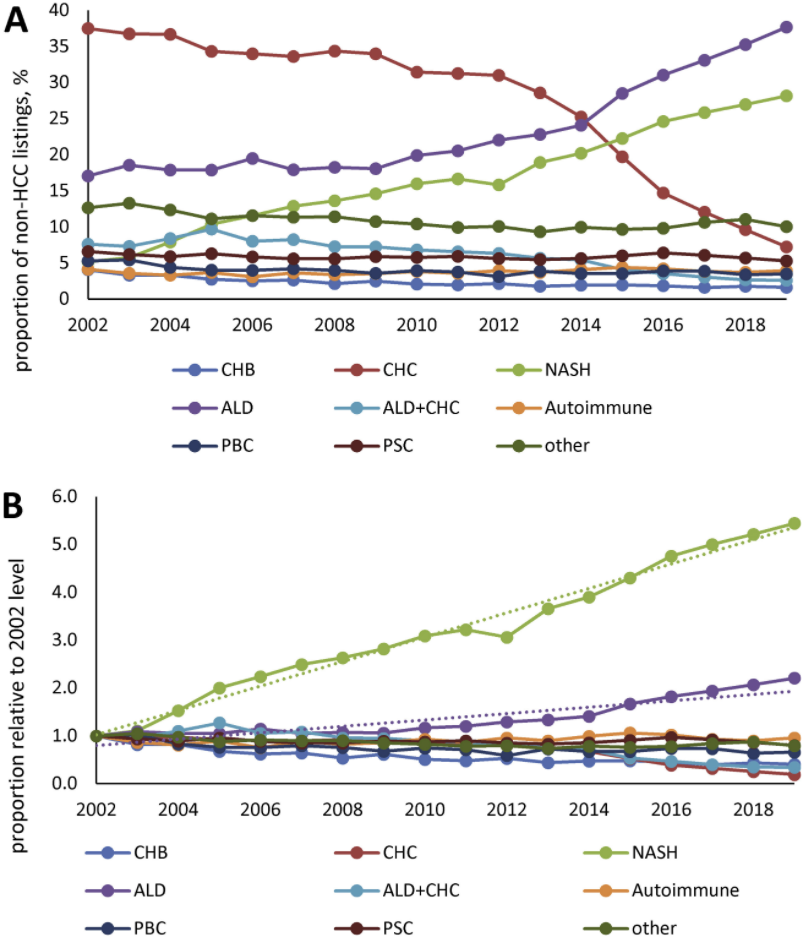
This study was an analysis of data from the Scientific Registry of Transplant Recipients (2002 through 2019).
Key findings:
In 2002, the most common etiologies of non-acute liver failure on the liver transplant waitlist (in patients without HCC)
In 2019, among patients without HCC, NASH was the second leading indication for liver transplantation (28% of patients), after ALD (38% of patients). were chronic HCV infection (37%) and ALD (16%), whereas only 5% had NASH
HCC accounted for 27,799 patients (16.5%) and was commonly due to chronic HCV throughout study period
My take: Demand for liver transplantation has NOT improved despite curative therapy for chronic hepatitis C. This is due to increased liver failure related to fatty liver disease and alcoholic liver disease.
Figure 1 Prevalence of the most common CLD etiologies in waitlisted liver transplant candidates without HCC. (A) Proportion of all non-HCC listings with known etiology; (B) the proportion relative to that seen in 2002.
K Gottlieb, J Requa et al. Gastroenterol 2021; 160: 710-719. Central Reading of Ulcerative Colitis Clinical Trial Videos Using Neural NetworksKey finding: A deep learning algorithm can be trained to predict levels of UC severity from full-length endoscopy videos with excellent agreement with human central readers; endoscopic healing accuracy was 97% for UC endoscopic index of severity (UCEIS) and 95.5% for endoscopic Mayo score.
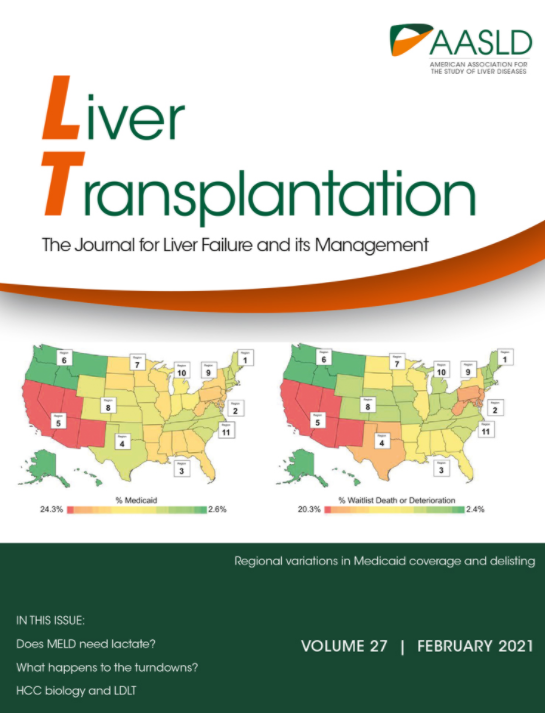
This was a retrospective study which relied on large national databases.
The 1‐year cumulative incidence of delisting was 9.0% (95% confidence interval [CI], 8.3%‐9.8%) for patients with private insurance, 10.7% (95% CI, 9.9%‐11.6%) for Medicare, and 10.7% (95% CI, 9.8%‐11.6%) for Medicaid
Medicare (HR, 1.20; 95% CI, 1.17‐1.24; P < 0.001) and Medicaid (HR, 1.20; 95% CI, 1.16‐1.24; P < 0.001) were independently associated with an increased hazard of death or deterioration compared with private insurance.
The article highlights regional variation in payor coverage and change in watilist death or deterioration from 2002-2018 (Figure 1)
Higher levels of education and employment were protective against waitlist mortality and deterioration
Female sex was a risk factor for delisting which may be in part to body size as women are more likely to have an organ declined as a result of small stature
“In patients hospitalized with decompensated cirrhosis, [daily] albumin infusions to increase the albumin level to a target of 30 g per liter or more was not more beneficial than the current standard care.” The standard of care included giving albumin under specific circumstances: large volume paracentesis, spontaneous bacterial peritonitis, or hepatorenal syndrome. Infusions (20% albumin) were infused at a rate of 100 mL/hr. In addition, the albumin group, which received 10 times as much albumin as the standard group, had more severe or life-threatening adverse events, especially pulmonary edema or fluid overload.
F Wong et al. NEJM 2021; 384: 818-828. Terlipressin plus Albumin for the Treatment of Type 1 Hepatorenal Syndrome In this multicenter, randomized controlled study, terlipressin was associated with improved renal function -reversal of HRS occurred in 32% compared to 17% in placebo group; however, it was associated with increased serious adverse events (eg. respiratory failure) and increased death (51% vs 45% in placebo group).
ER Perito et al. JPGN 2021; 72: 417-424.A Learning Health System for Pediatric Liver Transplant: The Starzl Network for Excellence in Pediatric Transplantation The Starzl Network for Excellence in Pediatric Transplantation (SNEPT) is the first multicenter effort by pediatric liver transplant teams. Its goal is to establish and share evidence-based care to improve liver transplantation outcomes. If successful, SNEPT should be to liver transplantation as ImproveCareNow network is for pediatric inflammatory bowel disease.