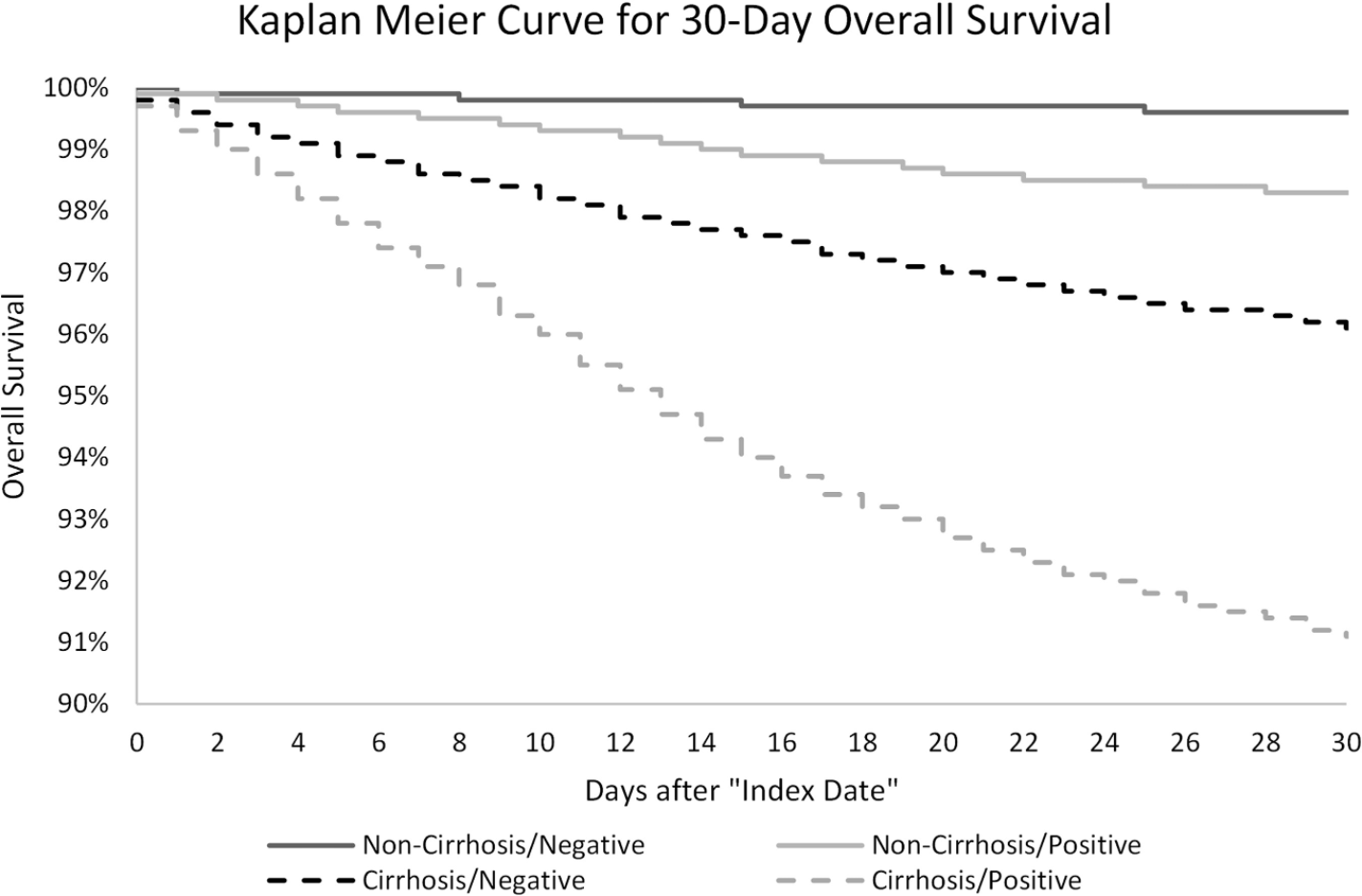
Key finding: “In this study of approximately 221,000 nationally representative, diverse, and sex-balanced patients with CLD; we found SARS-CoV-2 infection in patients with cirrhosis was associated with 2.38 times mortality hazard, and the presence of cirrhosis among patients with CLD infected with SARS-CoV-2 was associated with 3.31 times mortality hazard”
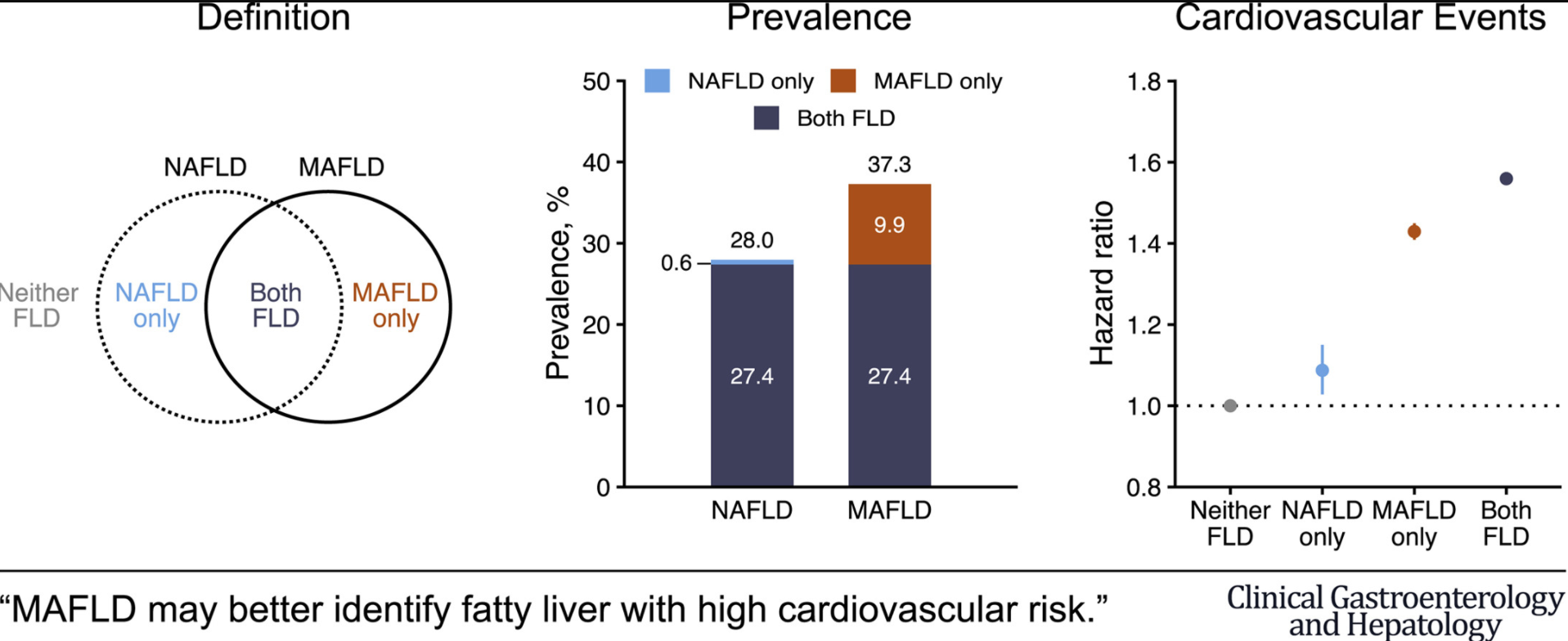
A recent study from South Korea with 9.5 million participants (followed for 10 years) shows that changing to metabolic dysfunction–associated fatty liver disease (MAFLD) as a name change from nonalcoholic fatty liver disease (NAFLD) changes the prevalence of at-risk individuals.
Key findings:
Prevalence of NAFLD and MAFLD were 28.0% and 37.3%, respectively
NAFLD and MAFLD were each associated with significantly higher risk for CVD events: multivariable-adjusted hazard ratios (95% confidence interval) for CVD events were 1.09 (1.03-1.15) in the NAFLD-only group, 1.43 (1.41-1.45) in the MAFLD-only group, and 1.56 (1.54-1.58) in the Both-FLD group
In the same issue, a study from Hong Kong showed similar prevalence rates between MAFLD (25.9%) and NAFLD (25.7%) (Clin Gastroenterol Hepatol 2021; 19: 2161-2171). This study noted that many people with hepatic steatosis at baseline have less severe metabolic burden.
Also, in the same issue, using a well-define population of more than 13,000 from NHANES III, this retrospective study (Clin Gastroenterol Hepatol 2021; 19: 2172-2181) found that Non-NAFLD MAFLD patients had the highest all-cause and cardiovascular-cause related mortality. In addition, this group had the highest rate of advanced fibrosis >7% (compared to <2% in other groups.
My take (borrowed from authors of first study): “The change from NAFLD to MAFLD criteria may identify a greater number of individuals with metabolically complicated fatty liver and increased risk for CVD.”
MAFLD is diagnosed based on the presence of hepatic steatosis with one or more of the following:
diabetes mellitus
overweight/obesity (BMI >/= 23)
at least 2 metabolic abnormalities: a) Waist circumference ≥90 cm in men and 80 cm in women. b) Blood pressure ≥130/85 mmHg or under anti-hypertension therapy. c) High-density lipoprotein cholesterol (HDL-C) <40 mg/dL for males and <50 mg/dL for females. d) Triglyceride (TG) ≥150 mg/dL or specific drug treatment. e) fasting glucose ≥100 f) Homeostasis model assessment-insulin resistance (HOMA-IR) score ≥2.5; and g) Hypersensitive C-reactive protein (hs-CRP) level >2 mg/L.
NAFLD Criteria in this study:
The presence of hepatic steatosis without 1. excessive drinking ( ≥30 g/day in men, ≥20 g/day in women) and 2. concomitant liver diseases
“It was Feb. 1, 1960, when four black students sat down at Woolworth’s lunch counter in Greensboro, N.C., and ordered coffee” (Time: Why the Woolworth’s Sit-In Worked)
This lunch counter sit-in was a big step in the civil rights movement. The article cited above shows that there is still a lot of work to make sure black patients have equal access to the liver counter too.
Using two databases (CDC WONDER, and UNOS) for 2014-2018, the authors identified 135,367 patients who died of ESLD, 54,734 patients who were listed for transplant, and 26,571 who underwent transplant.
Key findings:
The national LDR (listing-to-death ratio) was 0.40, significantly lowest in Black patients (0.30), P < 0.001. The highest LDRs clustered in the Northeast and the lowest in the Southeast and Northwest
The national transplant to listing ratio was 0.48, highest in Black patients (0.53), P < 0.01
The national transplant to death ratio was 0.20, lowest in Black patients (0.16), P < 0.001
“The most desirable outcome is a high transplant to death ratio—which was present in states like Maryland as well as Georgia, Nebraska, and Wisconsin.” (State values are provided in Tables 1, 3, and 4). Overall, these data show low listing rates for black patients relative to deaths from ESLD. Due to the adoption of MELD score which has objective criteria, the lower transplant rates indicate that Black patients face a disparity in access to liver transplantation.
The authors point out potential roadblocks:
ESLD first needs to be identified and patient referred to a liver transplant center
Black patients “were much less likely to understand the LT process”
Timing is critical, “especially in patients with HCC, which presents a more advanced in Black patients”
Insurance: “Black patients are more likely to be uninsured or to have public insurance, which is associated with poor access to listing and LT”
My take: This study shows that Black patients face disparities prior to transplant listing. In order to improve outcomes, patients first need to get a seat at the table.
Carvedilol (not approved in children) is a NSBB that has additional α1 adrenergic blocking activity that enhances the portal pressure–reducing effect, compared to other NSBBs (eg. nadolol, propranolol).
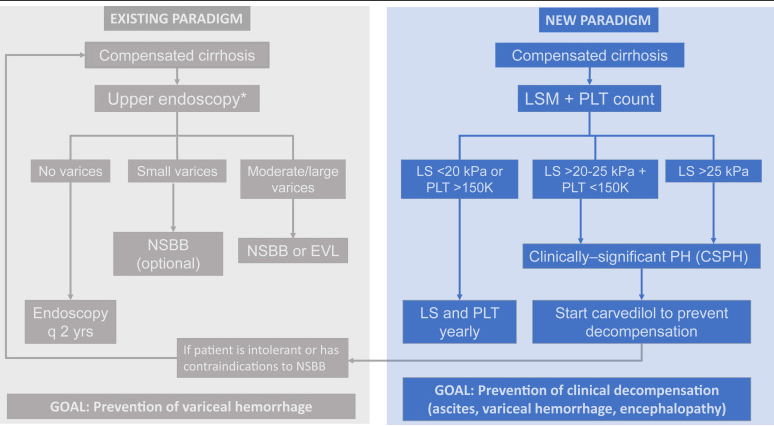
New paradigm focuses on “the most relevant end point in compensated cirrhosis…development of decompensation” (ascites, variceal hemorrhage, and/or hepatic encephalopathy).
In the PREDESCI study with 201 patients with compensated cirrhosis and CSPH, with no or small varices, to NSBBs or placebo…”clinical decompensation, was significantly lower in the NSBB arm than in the placebo arm (from 27% to 17% over a median follow-up of 37 months: HR 0.51, 95% CI 0.26–0.97)”
This model favors carvedilol over endoscopic variceal ligation; the “only RCT of carvedilol vs EVL in the prevention of first variceal hemorrhage showed a survival benefit of carvedilol over EVL.” Carvediol has been associated with improved survival in patients with cirrhosis (McDowell H.R. et al. Carvedilol is associated with improved survival in patients with cirrhosis: a long-term follow-up study. Aliment Pharmacol Ther. 2021; 5: 531-539)
This model “consists of identifying those with CSPH (by means of noninvasive methods) and treating them with carvedilol, with the goal of preventing any decompensating event (not only variceal hemorrhage).”
Screening endoscopy would still be recommended in newly-diagnosed decompensated cirrhosis and those intolerant to NSBBs.
My take: This new paradigm is one approach for portal hypertension in adults. More studies are needed in the pediatric age group to help determine whether medical therapy can obviate the need for EVL in most children with cirrhosis.
“Whereas the existing paradigm focuses on the use of NSBBs for the prevention of variceal bleeding, in the new paradigm the presence of CSPH [clinically significant portal hypertension ](determined noninvasively) establishes the indication for NSBBs with the goal of preventing cirrhosis decompensation. CSPH, clinically significant portal hypertension; EVL, endoscopic variceal ligation; NSBB, nonselective beta-blocker; LS, liver stiffness; PLT, platelet count. ∗Patients with LS <20 kPa and PLT >150,000/mm3 can circumvent endoscopy because the risk of having high-risk varices is minimal“
Related blog posts:
#NASPGHAN19 Liver Symposium (excellent presentation by Dr. Romero on varices in children and portal hypertension)
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
In this review, the authors propose expanding treatment indications for chronic hepatitis B virus (HBV).
The authors review current guidelines (Table 2 lists the major society recommendations). For example, the AASLD recommends HBV treatment for the following:
Antiviral treatment in all patients with cirrhosis and detectable viremia, independent of alanine aminotransferase (ALT) or HBV DNA levels
For patients without cirrhosis, all guidelines recommend treatment in patients with immune active disease; treatment is mainly with a NA (nucleos(t)ide analog) until 1 year after confirmed HBeAg seroconversion for patients who were HBeAg-positive and until HBsAg loss for patients who were HBeAg-negative at the start of treatment
AASLD cut-offs for distinguishing immune active disease: ALT ≥2× ULN or evidence of significant histologic disease and HBV DNA >20,000 IU/mL for HBeAg (+) and >2000 IU/mL for HBeAg (–)
Why Expand Treatment Indications?
The main reason for advocating treatment of patients in the immune tolerant phase is the mounting evidence that persistently high viremia and persistent presence of HBeAg are associated with increased risk of cirrhosis, HCC, and liver-related mortality…In one study of 438 HBeAg-positive patients, the 15-year cumulative risk of cirrhosis and HCC increased from 3.7% and 2.1% in patients who seroconverted before age 30 to 12.9% and 3.2% in those who seroconverted between ages 30 and 40 and 42.9% and 7.7% in those who did so after age 40
Why Not Treat All Patients with Chronic Hepatitis B?
“An important reason for deferring treatment of patients in the immune tolerant phase is that spontaneous HBeAg and HBsAg clearance with remission of liver disease can occur.” This happens in 80% or more over 10-20 years.
Who Else Should Receive Treatment (Beyond Guidelines)?
“Available data support expanding treatment to immune tolerant patients and patients in the grey zones who have evidence of active/advanced liver disease based on liver biopsy or non-invasive tests and those who remain in the immune tolerant phase after age 40. Evidence supporting treatment expansion to confirmed inactive carriers and other immune tolerant patients is lacking.” “Grey zones” indicate that “the course of chronic HBV infection is characterized by fluctuations in HBV DNA and ALT levels, and many patients will be in the grey zone at some point.”
My take: Given the safety/tolerability of newer HBV treatments, these recommendations make sense. If/when HBV treatments improve further (higher loss of HBsAg or HBV DNA), then even more widespread use of HBV treatments would be worthwhile.
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
“Remarkably safe and highly effective mRNA COVID-19 vaccines are now available for widespread use and should be given to all adult patients with CLD and LT recipients. The online companion document located at https://www.aasld.org/about-aasld/covid-19-resources will be updated as additional data become available regarding the safety and efficacy of other COVID-19 vaccines in development.”
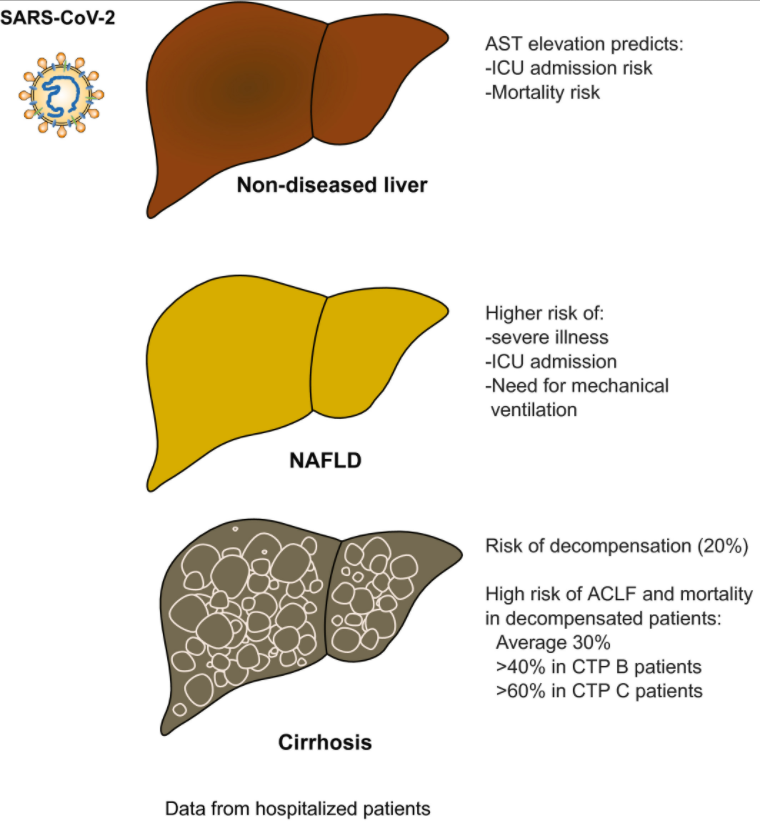
“The presence of liver injury is a surrogate marker for more severe disease and higher mortality in patients with COVID-19. An elevated AST level is the most robust predictor of poor outcome.”
“Liver injury and mortality in COVID-19 are likely multifactorial, driven by a sustained and excessive systemic release of proinflammatory and prothrombotic cytokines following SARS-CoV-2 infection, iatrogenic injury caused by DILI, hemodynamic changes associated with mechanical ventilation or vasopressor use, and worsening of underlying liver injury in those with CLD.”
“Risk of de novo liver injury appears limited in patients without CLD, and only rare cases of COVID-19–related ACLF [acute-on-chronic liver failure] were observed.”
“COVID-19–related liver injury and mortality in patients who were hospitalized with and without chronic liver disease (CLD). Patients without CLD usually present with AST elevation, which correlates with ICU admission and mortality. Among patients with CLD, NAFLD has the highest risk of severe illness, ICU admission, and need for mechanical ventilation. Patients with cirrhosis are at risk for decompensation, and patients who are decompensated have a high risk of acute-on-chronic liver failure (ACLF) and mortality.”–Abbreviations: CTP, Child-Turcotte-Pugh; ICU, intensive care unit.
“We are caring for young people with soaring rates of depression, anxiety, trauma, loneliness, and suicidality that will have lasting impacts on them, their families, their communities, and all of our futures,” said AACAP President Gabrielle A. Carlson, M.D. “We cannot sit idly by. This is a national emergency, and the time for swift and deliberate action is now.”
These organizations make several recommendations to policy makers including more access for mental health services. (I worry that we do not have sufficient numbers of qualified mental health practitioners to meet the challenge.)
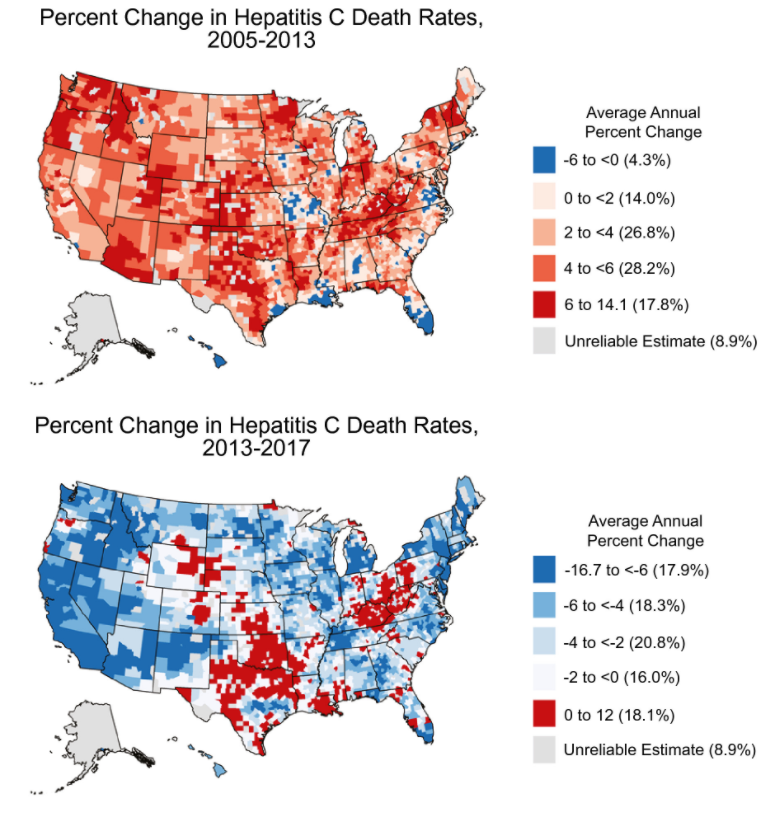
The authors used county-level HCV death rates and assessed trends in HCV mortality from 2005 to 2013 and from 2013 to 2017; the study is derived from mortality data from the National Vital Statistics System.
Key Findings:
Nationally, the age-adjusted HCV death rate peaked in 2013 at 5.20 HCV deaths per 100,000 persons and decreasing to 4.34 per 100,000 persons in 2017
There was heterogeneity in HCV mortality with the highest rates being concentrated in the West, Southwest, Appalachia, and northern Florida. 80% of counties had improvement in HCV mortality
My take: This study showed widespread improvement trends in HCV death rates from 2013 to 2017 and provides benchmarks for further progress. However, other studies have shown increasing rates of HCV tied to opioid crisis which could impact long-term outcomes as well.
This huge collaborative study with 130 patients provides a great deal of information about familial intrahepatic cholestasis type 1 (FIC1). Key findings:
Survival analysis showed an overall native liver survival (NLS) of 44% at age 18 years. NLS was comparable among FIC1-A, FIC1-B, and FIC1-C (% NLS at age 10 years: 67%, 41%, and 59%, respectively; P = 0.12)
The number of predicted protein truncating mutations did not correlate with natural history or prognosis
In this study, the researchers 834 patients with CHB previously treated with TDF for ≥12 months who were switched to TAF in routine practice at 13 US and Asian center. Key findings:
“Overall, we observed continued improvement in virologic response, ALT normalization, and no significant changes in eGFR following switch to TAF from TDF.”
HBV DNA suppression increased from 88% to 92% at 48 weeks post-switch, and then 95% at 96 weeks postswitch
Improved renal function: “By week 96, 21% (55/267) of patients with CKD stage 2 at switch improved to stage 1 and 35% (30/85) of CKD stage 3-5 patients improved to stage 2 and 1.2% (1/85) to stage 1.”
This practice guidance (with 276 references) is an update from similar guidelines published in 2012.
Key Points For Children:
Children with cirrhosis and ascites should be referred for evaluation for LT
Children undergoing LVP should receive 25% albumin infusion of 0.5-1.0 g/kg, or 6-8 g per liter of ascites removed.
Diagnostic paracentesis should be performed in children with ascites and fever, abdominal pain, or clinical deterioration. The risks and benefits of this procedure for use in all children with new ascites but without these symptoms have not been defined.
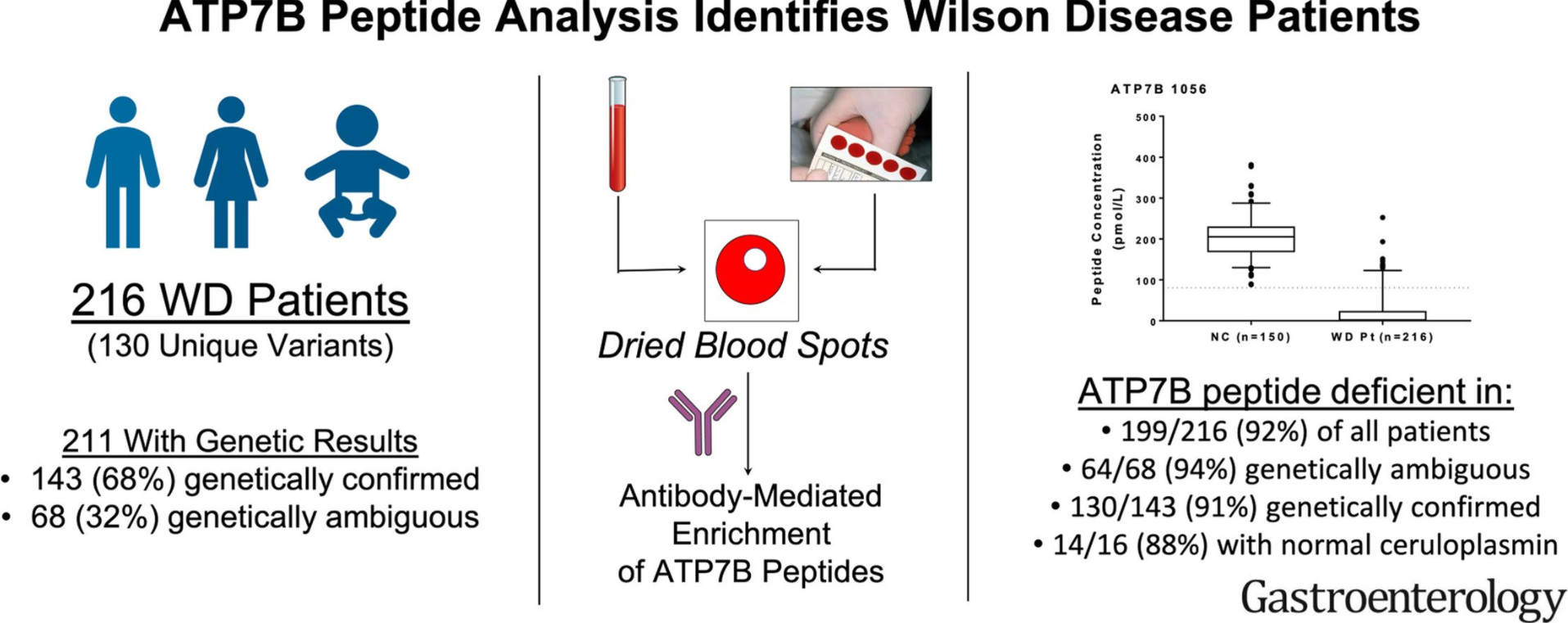
There continues to be challenges in the diagnosis of Wilson’s disease (WD). Genetic testing, per the authors and Vasrome (varsome.com), have found more than 649 pathogenic mutations and another 692 mutations that are VUS. Definitive diagnosis with genetic testing requires 2 known pathogenic variants. Other features, including Kayser-Fleischer rings and ceruloplasmin, have limited sensitivity and/or specificity.
Methods: Two hundred and sixty-four samples from biorepositories at 3 international and 2 domestic academic centers and 150 normal controls were used.
Key findings:
Two ATP7B peptides were found to have a sensitivity of 91.2%, specificity of 98.1%, positive predictive value of 98.0%, and a negative predictive value of 91.5%.
In patients with normal ceruloplasmin concentrations (>20 mg/dL), 14 of 16 (87.5%) were ATP7B-deficient. In patients without clear genetic results, 94% were ATP7B-deficient.
Discussion: As with other tests, ATPB7 peptide testing has limitations. Most patients with WD have pathogenic mutations that often result in protein misfolding, absence of decay of messenger RNA and enhanced degradation; hence, low ATPB7 levels; however, disease-causing mutations that affect protein activity but not protein concentration will generate false-negative results.
My take: “ATP7B peptide analysis identified WD patients in a large majority of cases and reduced ambiguities resulting from genetic analysis and Cp (ceruloplasmin) levels. This noninvasive assay can serve as an adjunctive test for the diagnosis of WD and is expected to fundamentally advance the use of proteomic technology for a rapid screening tool.
Data pooled from 27 studies showed the prevalence of NAFLD among IBD patients was 32% (substantial heterogeneity); this is “statistically significantly higher than the prevalence of NAFLD in the general population (25.2%; P < 0.001)”
A total of 93 studies were identified, comprising 16,064 IBD patients with co-occurring IMIDs and 3,451,414 IBD patients without IMIDs. IMIDs included the following:
Unspecified autoimmune disease
Diabetes type 1
Asthma
Grave disease
Spondyloarthropathy
Ankylosing spondylitis
Iridocyclitis
Uveitis
Rheumatoid arthritis
Polymyalgia rheumatica
Psoriasis/psoriatic arthritis
Primary Sclerosing Cholangitis
Celiac disease
Pyoderma gangrenosum
Pernicious anemia
Autoimmune hepatitis
Sarcoidosis
Giant cell arteritis
Primary biliary cholangitis
Hashimoto thyroiditis
Episcleritis
Sjogren syndrome
Key findings: Patients with IBD and co-occurring IMIDs were at increased risk of having extensive colitis or pancolitis (risk ratio, 1.38; 95% Cl, 1.25–1.52; P < 0.01, I2 = 86%) and receiving IBD-related surgeries (risk ratio, 1.17; 95% Cl, 1.01–1.36; P = 0.03; I2 = 85%) compared with patients without IMIDs