This retrospective review of 24 children with tethered cord syndrome (TCS) (50% female) who had ARM testing (median age at ARM 6.0 years). 19 children had prior TCS repair.
Key findings:
No significant differences in ARM parameters were found between children who had detethering surgery before ARM and children with functional constipation (FC). The children with TCS did have lower resting pressures though this was attributed to most having their ARM while under GA for concurrent procedures. The resting pressures were still normal.
Among the 14 children who also had a colonic manometry (CM) performed (13/14 after detethering surgery), there were no significant differences in colonic motility were found between children with a history of TCS and children with FC.
My take: The vast majority of children with a history of TCS (following detethering) should be treated akin to children with functional constipation.
Impression, Sunrise by Claude Monet at National Gallery of Art (Washington, D.C.)
A D’Agrosa et al. J Pediatr 2024; 273; DOI: 10.1016/j.jpeds.2024.114129. Cefdinir Stool
This 5 month old infant was brought to ED due to diarrhea and dark stools for 2 weeks. She had completed cefdinir for a UTI.
Cefdinir may cause red or maroon stools when administered with iron or products that contain iron, such as infant formula. This typically occurs within two days of antibiotic administration.
My take: Familiarity with this reaction is helpful to avoid extensive evaluations. Also, it is worthwhile to keep in mind that false-positive testing with guaiac testing is common (up to 34% in healthy infants).
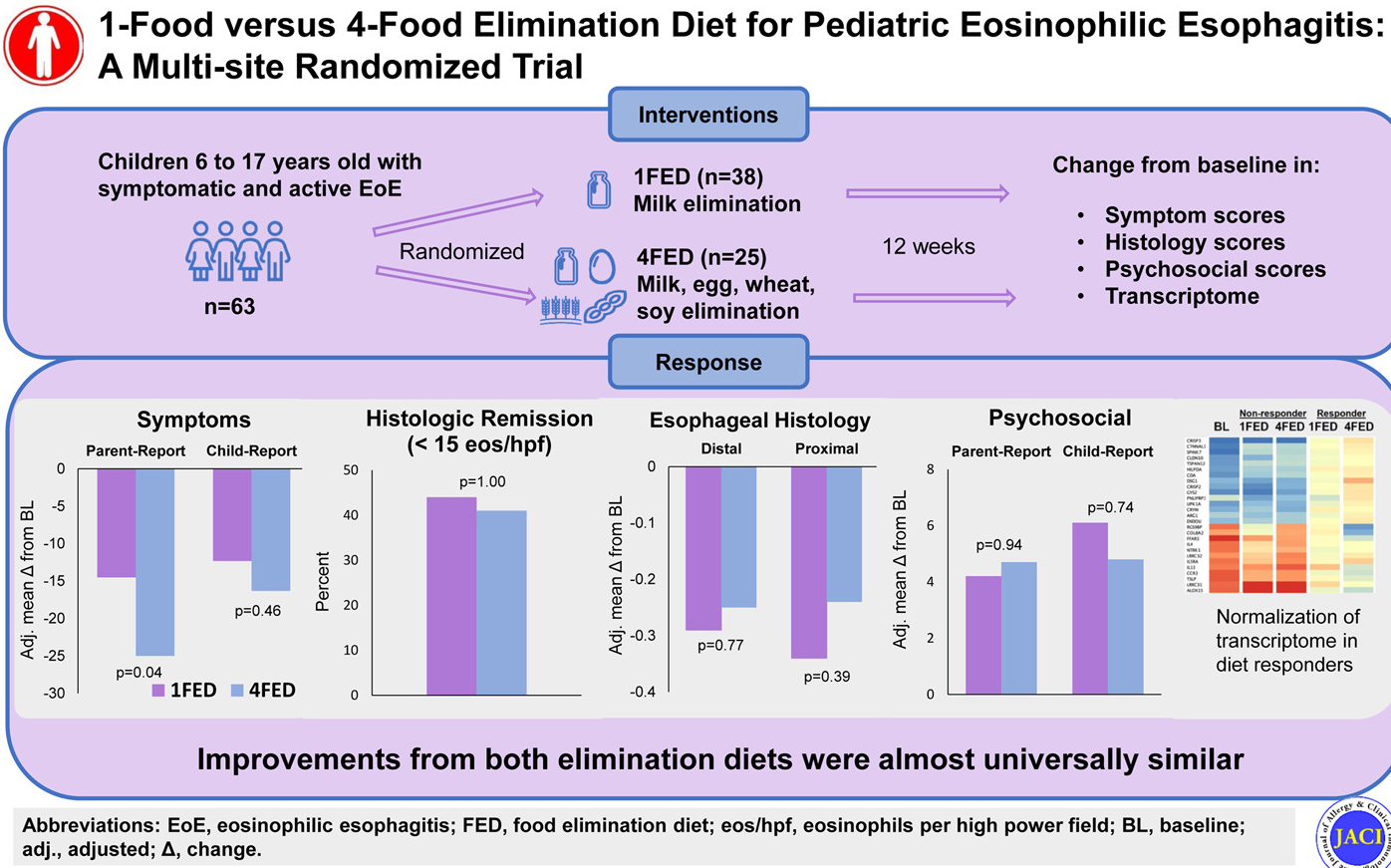
Methods: This was a multisite, randomized comparative efficacy trial of a 1-food (milk) elimination diet (1FED) versus 4-food (milk, egg, wheat, soy) elimination diet (4FED) in pediatric EoE. The 12-week study enrolled 63 patients (6-17 yrs). Primary end point was symptom improvement by Pediatric Eosinophilic Esophagitis Symptom Score (PEESS).
Key findings:
1FED vs 4FED: The mean PEESS improved −25.0 versus −14.5 (P = .04), but remission rates (41% vs 44%; P = 1.00), histology scoring system (−0.25 vs −0.29; P = .77), endoscopic reference score (−1.10 vs −0.58; P = .47), and QoL scores were similar between groups.
The 4FED withdrawal rate (32%) exceeded that of 1FED (11%) (P = .0496).
My take: A 4FED diet is difficult to maintain. In this 12 week study, more than 30% of patients withdrew from the 4FED diet. In addition, dairy elimination alone resulted in similar response rates.
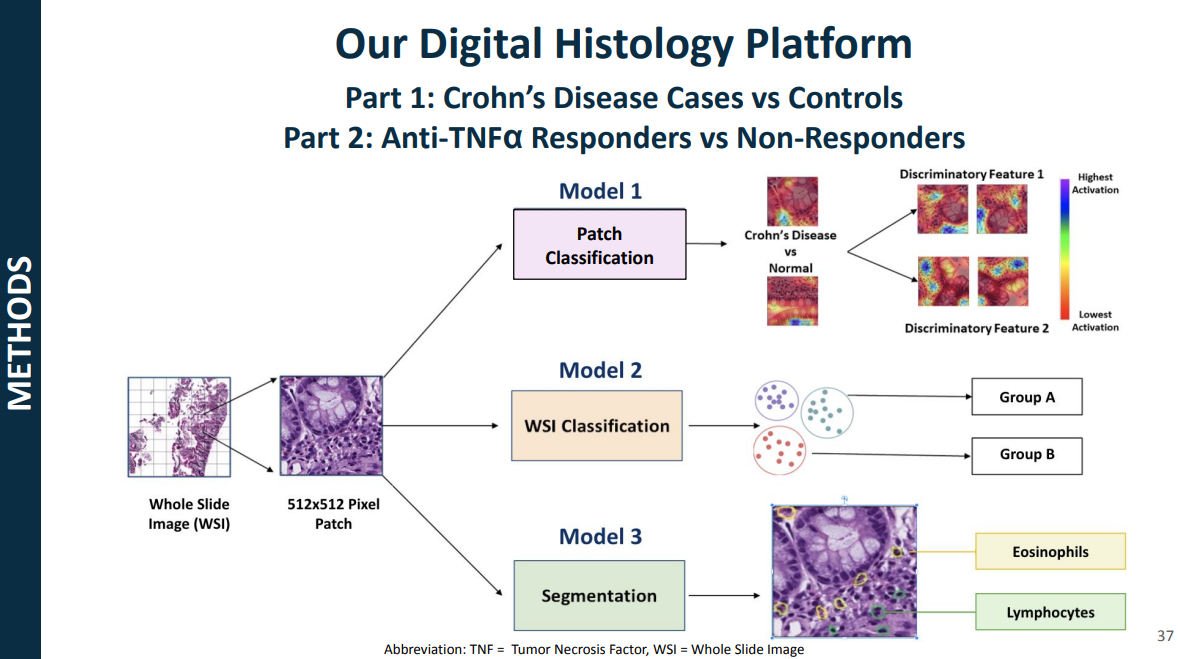
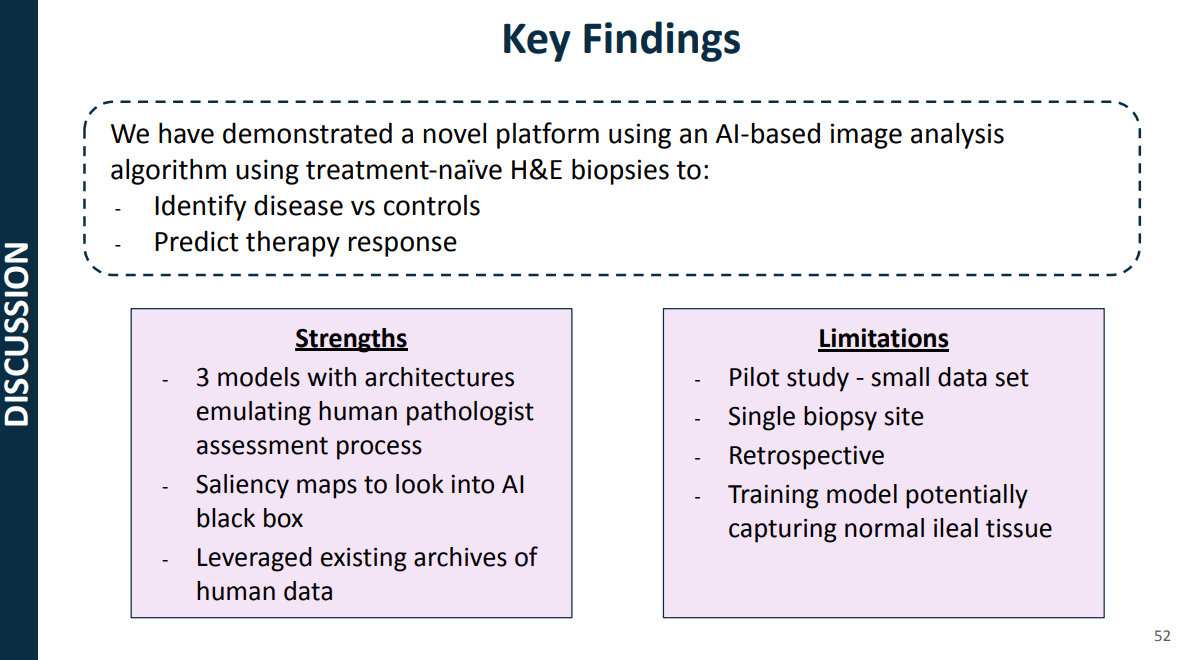
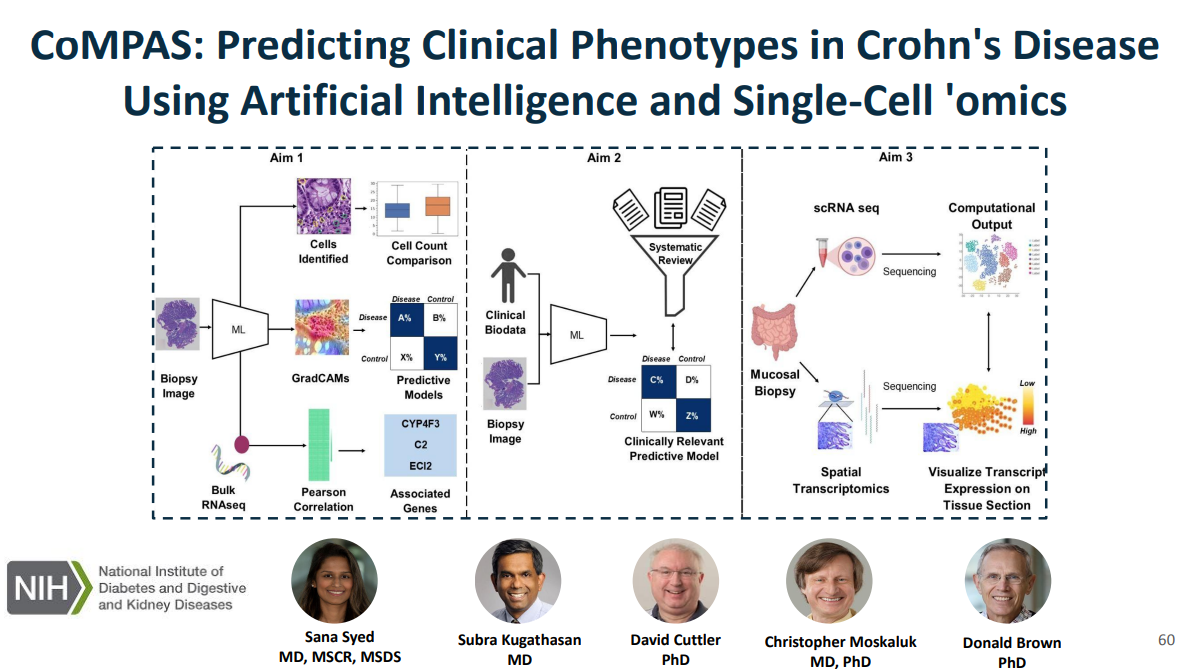
Recently, Dr. Sana Syed gave Children’s Healthcare of Atlanta Grand Rounds. She provided an excellent update on the development of artificial intelligence (AI) to select targeted therapies for pediatric gastroenterology diseases. My notes below may contain errors in transcription and in omission. Along with my notes, I have included many of her slides.
Key points:
One of the goals of using AI is to identify the right therapy at the time of diagnosis. Currently, diseases like eosinophilic esophagitis (EoE) and Crohn’s disease have multiple treatment options. However, many patients do not respond to first-line treatments; many develop complications due to not responding to treatment.
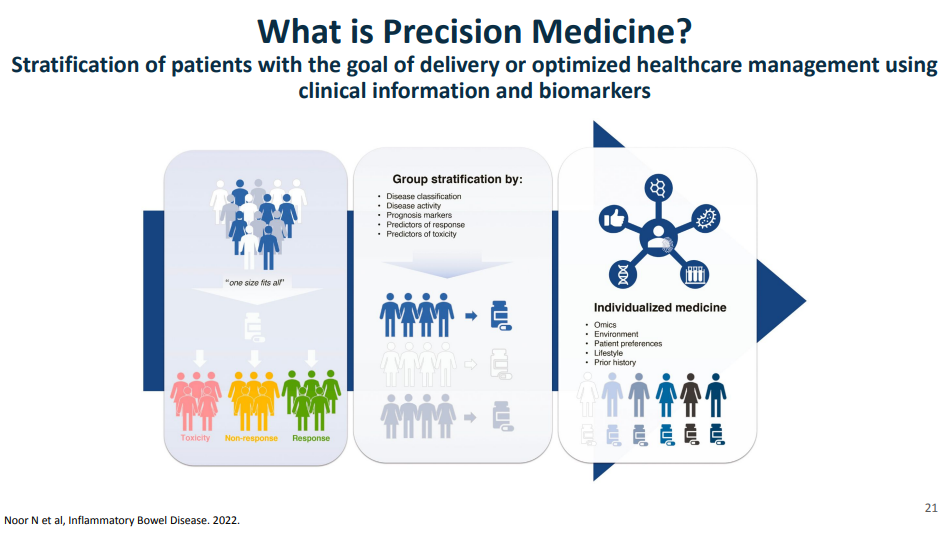
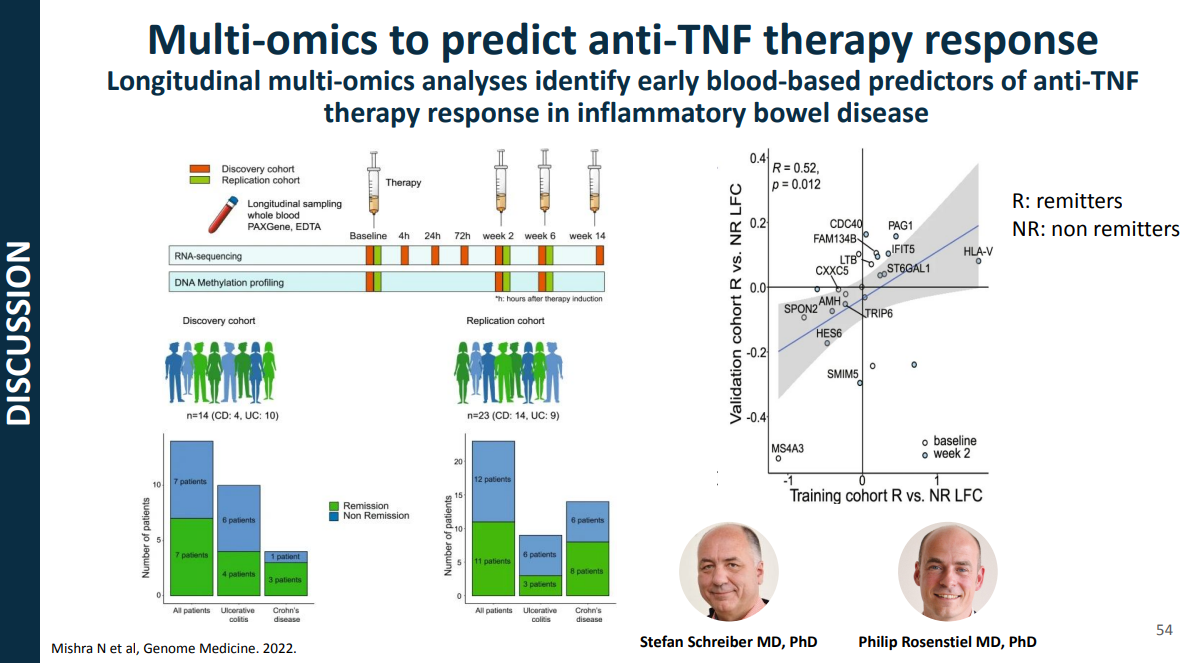
Currently we are lacking adequate biomarkers for individualized therapy. AI has the potential to sort through massive amounts of data (histologic, genetic, pharmacokinetics, transcriptome, metabolomics, etc) to allow for precision therapy.
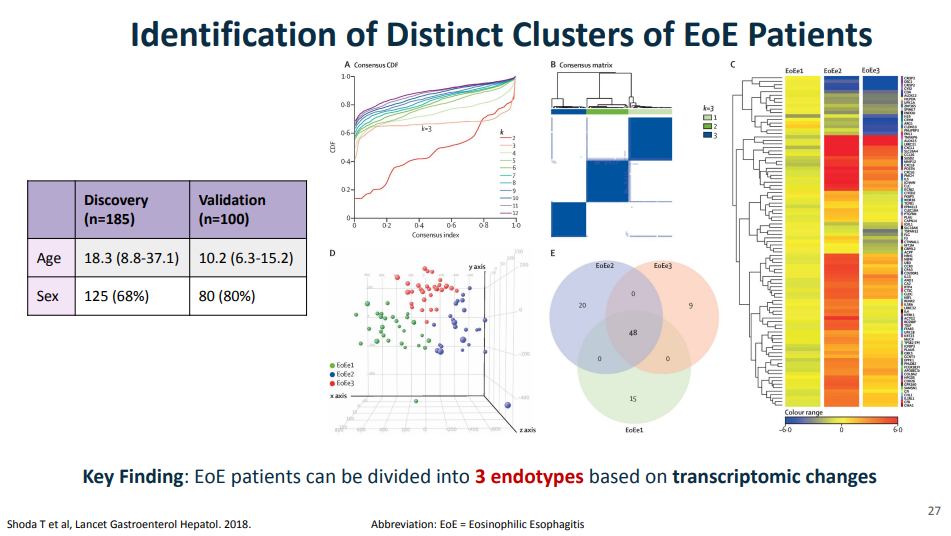
For EoE, machine-learning has already identified three subtypes that may affect clinical management. EoE1 is associated with a normal-appearing esophagus. EoE2 is associated with being steroid refractory. EoE3, when compared to the other two endotypes, is associated with adult-onset and narrow-caliber esophagus or stricturing.
For Crohn’s disease, research has shown that younger age has been associated with an increased risk of not responding to anti-TNF therapy
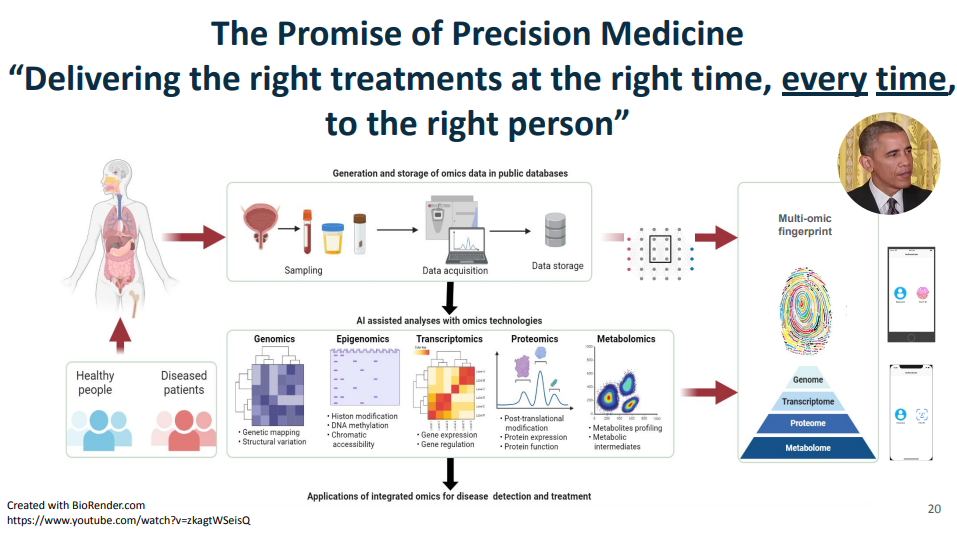
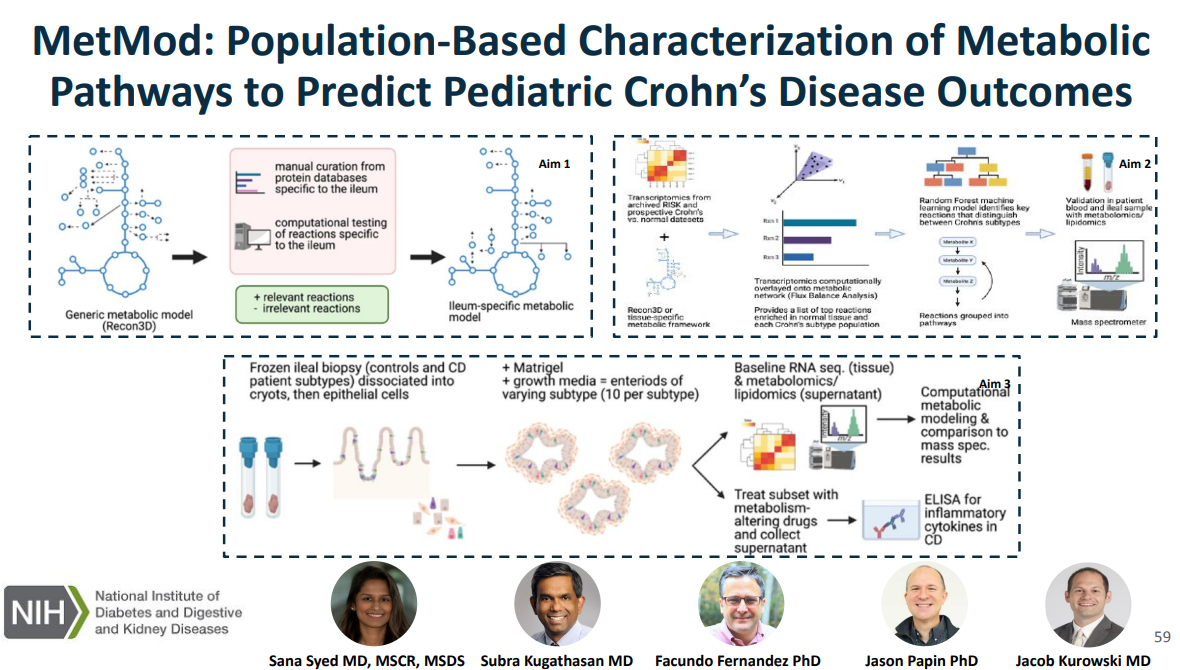
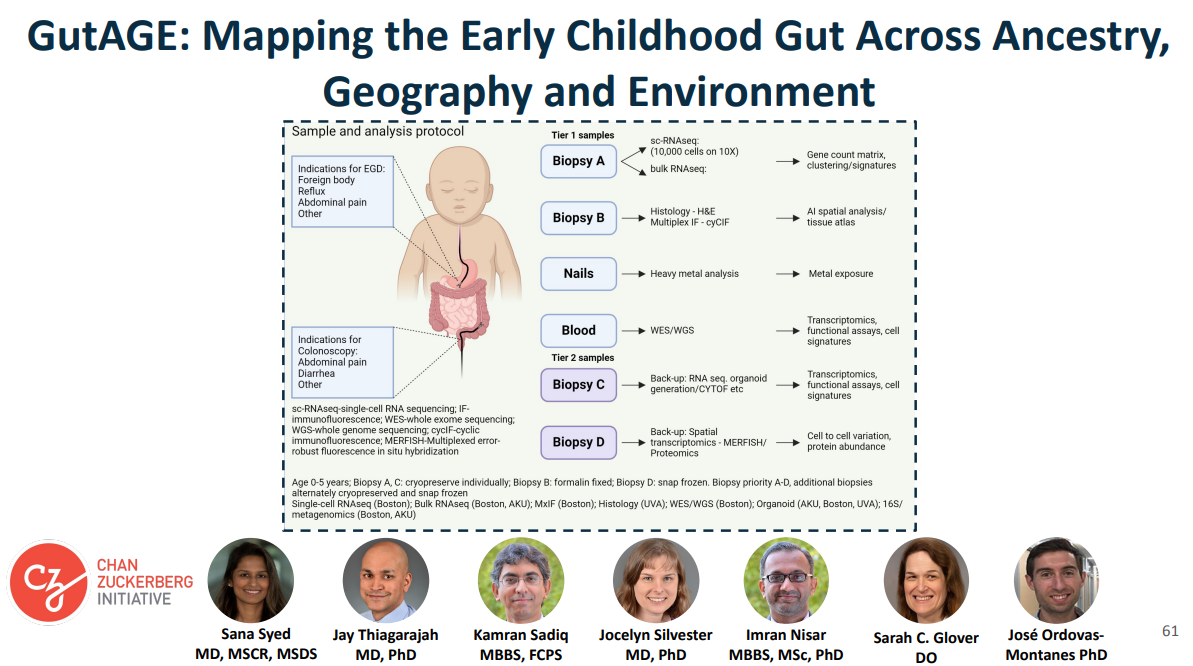
This is a quote from President Obama when his administration announced massive funding toward precision medicine in January of 2015, that the promise of precision medicine is ”delivering the right treatments at the right time, every time to the right person.” This figure illustrates some of the kinds of data that Dr. Syed had access to as faculty at UVA, including genomics, epigenome, transcriptomics, proteomics, metabolomics, etc.Shoda and colleagues, used a combination of histology data, endoscopic features, histologic and endoscopic scoring indices, and transcripts that make up the eosinophilic esophagitis diagnostic panel, a quantitative PCR assay with 96 EoE representative genes. The key message from all of those visualizations is that they found that EoE can be divided into three distinct endotypes after analyzing transcriptomics changes via partition-around-medoid clustering, a machine-learning method.In this project, the researcher intend to curate a novel metabolic network specific to the ileum, which is relevant to Crohn’s disease, link metabolic processes with Crohn’s disease phenotypes using in silico metabolic network modeling and ‘omics and characterize and target metabolic pathways in an organoid model generated from patient-derived Crohn’s disease tissue.In CoMPAS, the researchers aim to leverage artificial intelligence methods (AI) methods to build predictive models for CD using histology slides and single-cell RNA sequencing, allowing for risk stratification of B1 patients who will respond to anti-TNF therapyThe goal of our project is to create a multi-omics reference dataset with scRNA-seq data coupled with contextual data on tissue morphology, ancestry, social determinants of health, and the environment. The cohort for this study is enrolling patients who have clinical indications for endoscopy like foreign body removal, reflux, abdominal pain
My take: This work is necessary to identify the right treatments for each patient and will lead to better outcomes. We are already seeing the early stages of machine-learning’s impact on clinical care. In many other fields, AI work is much further along (especially in oncology). A recent study in Nature identified JAK inhibitors as potential life-saving therapy with toxic epidermal necrolysis (TEN).
Reference: Nordmann, T.M., Anderton, H., Hasegawa, A. et al. Spatial proteomics identifies JAKi as treatment for a lethal skin disease. Nature (2024). https://doi.org/10.1038/s41586-024-08061-0
Summary from Eric Topol (Ground Truths) focusing on spatial omics: Thierry Nordmann, Matthias Mann and their international consortium, used deep visual proteomics from 3μm PPFE sections of skin biopsies in patients affected by TEN…
More than 5,000 proteins were quantified from single cells—keratinocyte and immune cells—using mass spec, for the 4 different skin conditions (proteome cluster in Figure below, left panel). This led to the finding that the TEN patients had marked increased in Type 1 and 2 interferon signaling and activation of phosphorylated STAT1, which invoked the janus kinase (JAK/STAT) pathway. Subsequent steps were to test JAK inhibitors in cell culture (with live cell imaging) and in two different mouse models, all showing highly potent, dose-dependent impact on inhibition of the intense inflammatory process and disease severity…
They went on to treat seven patients at Fuian Medical University, the course of one patient shown below, treated with a JAKi on day 4 after diagnosis, and manifesting a marked response starting within 48 hours. All 7 patients fully resolved, with no side effects…
For spatial medicine, there are multiple analytical challenges that invoke the need for machine learning and A.I., including segmentation of cell types, automated capture of cells of microdissection, extracting useful information from the >5,000 proteins quantified per cell, and ultimately, as we’ll see more in the future, A.I. powering the construction of high-resolution 3D maps.
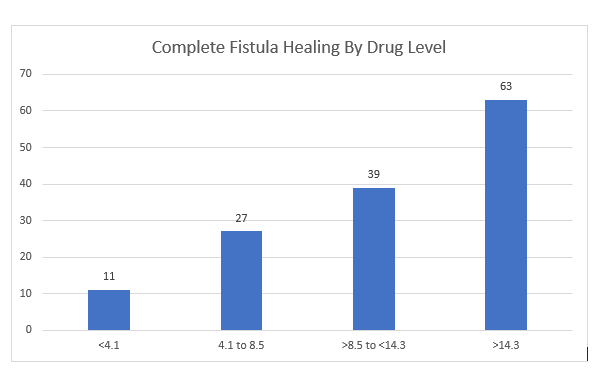
In this multicenter retrospective review with 183 patients, the adalimumab (ADM) levels were examined with respect to healing of perianal fistulas. Most patients (82%) had complex perianal fistulizing CD.
Key findings:
87 patients (48%) received intensified dosing at the time of therapeutic drug monitoring (TDM)
Patients with complete fistula healing (CFH) had higher median ADM levels: 12.9 compared to 6.1 for those witout CFH
“Optimal ADM concentration associated with CFH was 12.2 mcg/mL” which had positive predictive value of 64% and negative predictive value of 80%. Among those with ADM >12.1, CFH was achieved in 64% compared to 20.5% in those with concentrations <12.1 (Odds ratio, 5.7). “Even higher drug levels may be needed.”
There were 46 patients in each drug level category
My take: There is a lot of data supporting TDM, including proactive TDM, with anti-TNF agents like adalimumab and infliximab. This study shows that with fistulizing disease higher drug levels are needed to achieve better outcomes.
From Caitlyn Rivers Newsletter, Force of Infection 11/4/24:
Norovirus is high and increasing right now. Nationally, test positivity is at nearly 12%. To put this in context, the peak last year was 13.6%. Rates are particularly high in the Southern region.
A reminder as cases increase: norovirus causes stomach pains, diarrhea, and vomiting. It is extremely transmissible via bodily fluids and through contaminated surfaces, food, and water.
To reduce your odds of getting sick, remember to wash your hands frequently with soap and water for at least 30 seconds (norovirus is able to withstand hand sanitizer).
If you or someone in your household becomes sick, wash hard surfaces with soap and water or a diluted bleach mixture, and wash soiled clothing and linens in hot water and then dry on high heat.
Norovirus is still highly transmissible for several days after symptoms improve or go away. As such, insofar as is possible, avoid preparing food for others for at least 72 hours after symptoms end. Longer is better: it can spread up to two weeks after symptoms end, though it is most transmissible during those first few days of illness and after symptoms resolve.
In this observational prospective cohort with 114 children (after excluding 6), outcomes following the first episode of acute pancreatitis (AP) were determined. In addition, pancreatitis risk genes (CASR, CEL, CFTR, CLDN2, CPA1, CTRC, PRSS1, SBDS, SPINK1, and UBR1) were sequenced. A genetic risk score was derived from all genes with univariable P < .15.
Pre-DM was defined as follows: fasting blood glucose ≥100 mg/dL and <126 mg/dL, or hemoglobin A1C ≥5.7% and <6.5%
Key findings:
95/114 (83%) remained normoglycemic and 19/114 (17%) developed endocrine insufficiency (4 DM, 15 pre-DM) 12 months after the first episode of AP
Sixty-three subjects (52.5%) had at least 1 reportable variant identified
Severe AP (58% vs 20%; P = .001) and at least 1 gene affected (79% vs 47%; P = .01) were enriched among the endocrine-insufficient group
CFTR (53%), SPINK1 (13%), PRSS1 (10%), and UBR1 (9%) accounted for the majority of variants identified
My take: 3.5% of this cohort developed diabetes and 13% developed prediabetes. The risk is increased in those with severe acute pancreatitis and underlying genetic variants. As noted recently with Dr. Freeman’s lecture (summarized on prior blog posts), it is worthwhile for patients to follow-up after an episode of acute pancreatitis.
“A new report by the Commonwealth Fund finds some US states have firearm death rates comparable to countries in conflict…For instance, Mississippi’s rate of firearm-related violence (28.5 per 100,000 people) was nearly double that of Haiti (15.1 per 100,000) in 2021…
Rhode Island, which has the lowest firearm death rate in the US (three per 100,000) is still 23 times higher than the United Kingdom (0.13 per 100,000) and nearly 1.3 times higher than France (2.3 per 100,000).
The US overall is in the 93rd percentile of all countries and territories for overall firearm mortality, at 13.5 deaths per 100,000 people…
In another example, Mississippi, Louisiana, Alabama and New Mexico all have higher firearm mortality rates than Mexico, where decades of violence between state forces and rival drug cartels has caused hundreds of thousands of deaths and left more than 115,000 people missing…
More than half of all firearm-related deaths (56.1%) in 2022 were from suicide…the rate of firearm deaths among American children is 72 times higher in the US than in the UK (36.4 deaths per million versus 0.5 deaths per million)
My take: The fact that the U.S firearm mortality rates can be compared unfavorably to places with violent reputations like Haiti and Mexico is awful. What’s worse is the capitulation by most to not even try to improve the situation.
No Exaggeration: Too Many Children Are Dying in the U.S. (2019) “The sad fact is that a child or adolescent in the United States is 57% more likely to die by the age of 19 years than those in other wealthy nations.” This is due mainly to more deaths from MVAs and from gun violence.
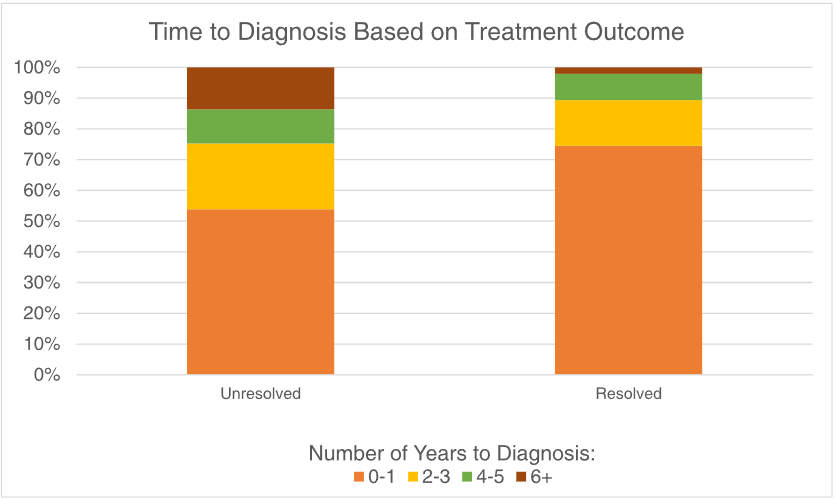
MR Jia et al. J Pediatr Gastroenterol Nutr. 2024;79:850–854. Delay in diagnosis is associated with decreased treatment effectiveness in children with rumination syndrome
In this retrospective single-center study with 247 patients, the authors evaluated whether the time from symptom onset to diagnosis over time and whether it was associated with symptom resolution.
Key findings:
The median age at symptom onset was 11 years and median age at diagnosis was13 years
Among the 164 children with outcome data, 47 (29%) met criteria for symptom resolution after treatment
A longer time to diagnosis was associated with a lower likelihood of symptom resolution after treatment (p = 0.01)
In the discussion, the authors note that “we suspect that one contributing factor to worse outcomes associated with diagnostic delays is the excessive testing leading to over‐medicalization of DGBIs…Our findings are the first to show that diagnostic delay contributes to poorer outcomes in children with RS, which highlights the importance of a timely diagnosis.” In fairness to the authors, other parts of the manuscript state that the delay in diagnosis is associated with worse outcomes but does not attribute causality.
Limitations:
The patient cohort is derived from a specialized referral center (Nationwide Children’s)
Recall bias
My take:
While I concur that a timely diagnosis of rumination syndrome is useful, it is unproven that a delayed diagnosis contributes to a worse outcome. The outcome differences could more easily be explained by a selection bias. Patients who never recovered from rumination symptoms previously may be less likely to respond to treatment regardless of when treatment is instituted. Perhaps attributing poor outcomes to delayed diagnosis, rather than a selection bias, is due to a confirmation bias.
Another important finding is that the more than 70% of patients did NOT have resolution of their symptoms. Realizing that many patients have some symptoms after treatment helps gastroenterologists set reasonable goals.
Methods: Two randomized, placebo-controlled, double-blind studies were conducted in patients with moderately to severely active CD or UC and inadequate response or intolerance to corticosteroids and immunomodulators. All patients received open-label CT-P13 IV 5 mg/kg at weeks 0, 2, and 6. At week 10, clinical responders were randomized (2:1) to CT-P13 SC 120 mg or placebo every 2 weeks until week 54 (maintenance phase) using prefilled syringes.
Key findings:
At week 54 in the CD study, statistically significant higher proportions of CT-P13 SC–treated patients vs placebo-treated patients achieved clinical remission (62.3% vs 32.1%; P < .0001) and endoscopic response (51.1% vs 17.9%; P < .0001)
In the UC study, clinical remission rates at week 54 were statistically significantly higher with CT-P13 SC vs placebo (43.2% vs 20.8%; P < .0001).
CT-P13 SC was well tolerated, with no new safety signals identified.
The mean serum infliximab trough concentrations at weeks 14 and 54 were 13.2 and 14.8 mcg/mL with CD study and 14.6 and 16.3 with UC study, respectively.
Proportions of patients achieving co-primary and key secondary end points at week 54 in the CD study (all randomized population)Proportions of patients achieving primary and key secondary efficacy end points at week 54 in the UC study (all randomized population)
Discussion:
“The present findings are generally comparable with or numerically better than those observed in previous clinical trials that evaluated IV infliximab in patients with CD or UC…At week 50 in the SONIC trial, 35% of patients receiving infliximab achieved corticosteroid-free clinical remission,30 compared with 40% of patients in the CT-P13 SC group in the current study.”
“In terms of UC, the ACT 1 study4 found that patients receiving infliximab 5 mg/kg and 10 mg/kg were more likely to achieve clinical remission based on total Mayo score after 54 weeks (34.7% and 34.4%, respectively) compared with participants receiving placebo (16.5%), and in the current study, 43.2% and 20.8% of patients, all of whom had responded to induction therapy, achieved clinical remission at week 54 in the CT-P13 SC and placebo groups, respectively.”
This study had a high rate of antidrug antibody detection (63.8%–65.1%)…” likely due to the use of highly sensitive, next-generation ADA assays, which have improved sensitivity compared with those used in historical studies… This suggests that route of administration of CT-P13 does not affect rates of ADA formation, and that the observed incidence of ADA is not unexpected.”
“The decision to initiate CT-P13 SC maintenance therapy at week 10, 4 weeks after finishing CT-P13 IV induction therapy, was based on results of PK or pharmacodynamic model simulation.”
My take: These studies suggest that SC infliximab is likely to have similar efficacy as IV infliximab