V Jairath et al. Clin Gastroenterol Hepatol 2024; 22: 1077-1086. Open Access! ENTERPRET: A Randomized Controlled Trial of Vedolizumab Dose Optimization in Patients With Ulcerative Colitis Who Have Early Nonresponse
Methods: ENTERPRET was a phase 4, open-label, randomized, controlled trial (n=278) that included patients with moderate to severe UC who had high drug clearance at week 5 (serum concentration, <50 μg/mL) and nonresponse to standard vedolizumab treatment at week 6. At week 6, eligible patients were randomized 1:1 to receive standard dosing (300 mg every 8 weeks) or dose-optimized vedolizumab (600 mg at week 6, then 300 mg every 4 weeks; or 600 mg at week 6, then 600 mg every 4 weeks [based on week 5 serum concentration]).
After an initial clinical response of 47.5% (132/275) at week 6, 108 patients were subsequently randomized into either standard (n = 53) or dose-optimized vedolizumab (n = 55). The majority (86%) with nonresponse at week 6 had high drug clearance
Key findings at week 30:
- Endoscopic improvement: 10 patients (18.9%) with standard vedolizumab vs 8 patients (14.5%) with dose-optimized vedolizumab
- Clinical remission: Five patients (9.4%) with standard vedolizumab vs 5 patients (9.1%) with dose-optimized vedolizumab
- Clinical response: 17 (32.1%) with standard vedolizumab vs 17 (30.9%) patients (30.9%) with dose-optimized vedolizumab
In their discussion, the authors note the gain of clinical response of ~16% in both groups is consistent with other studies showing “8% to 16% increase in the proportion of patients who had a clinical response between 6 and 14 weeks.” Thus, duration of treatment may be more important that serum drug level.
My take (borrowed in part from authors): “In patients with early nonresponse and high drug clearance, vedolizumab dose optimization is probably not required.” At week 30, both standard dosing and dose-optimized groups had a significant response despite lack of response at 6 weeks. So, it may be best to give a longer treatment course before reaching a conclusion on vedolizumab’s efficacy.
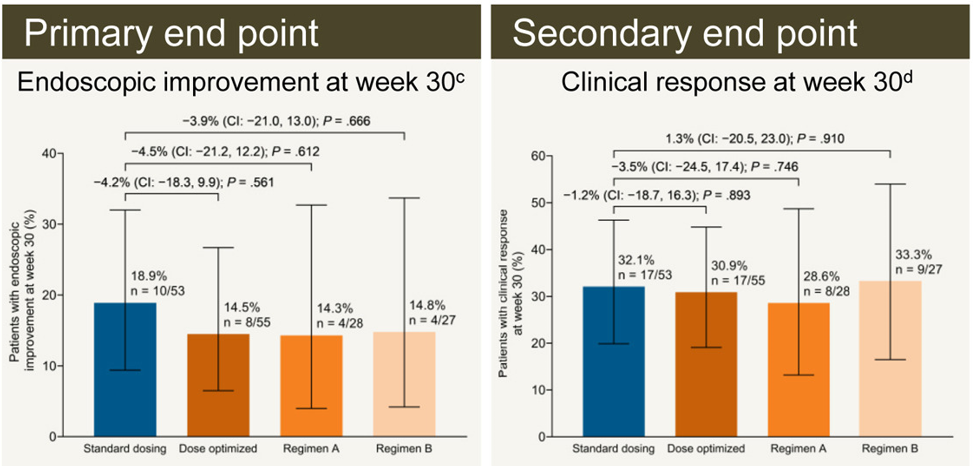
d Reduction in total Mayo score of >/=3 points and >/= 30% from baseline with an accompanying decrease in rectal bleeding subscore of >/=1 or absolute rectal subscore of </= 1
Related blog posts: