TF Danialifar et al. JPGN 2024; https://doi.org/10.1002/jpn3.12151 Open Access! Genetic and acquired sucrase-isomaltase deficiency: A clinical review
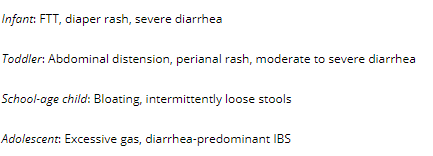
Most Common Presentation by Age:
Key points:
- 37 potential SI gene variants, including the four most common variants seen in genetic sucrase-isomaltase deficiency (GSID). Some variants have isomaltase activity and individuals with these variants can tolerate/digest starch
- Children with disorders of gut–brain interaction (DGBI) with a primary complaint of loose stools were found to have a higher prevalence of SI pathologic variants, the vast majority heterozygous, compared with those in a reference consortium database (4.5% vs. 1.3%, respectively).28 Children with DGBI who had primarily abdominal pain did not have a higher prevalence of SI pathologic variants
- Disaccharidase testing: Disaccharidase assay on duodenal mucosal tissue homogenates is currently the gold standard for diagnosing overall SID…One in five cases with pan-disaccharidase deficiency of all four or all five evaluated enzymes may be associated with heterozygous SI mutations and sucrase deficiency.39 A ratio of sucrase to lactase at 1.0 or less has been proposed as a guide to CSID, but may miss cases
- Genetic testing: Genetic tests for four common mutations up to the entire SI gene are commercially available.9, 39 The test is typically performed using genomic DNA extracted from buccal/cheek swab and blood samples. One specialty laboratory also accepts formalin-fixed paraffin-embedded biopsy tissues and other biopsy samples.
- Diet: Good dietary advice is provided in Table 3 (see below).
- Sacrosidase Treatment: Dosing of sacrosidase is weight-based, with a recommendation of 1 mL for patients weighing less than 15 kg and 2 mL for patients weighing more than 15 kg. The enzyme should be taken with each meal or snack, mixed into 2–4 ounces of room temperature liquid, and divided with half taken before the meal and half taken midway through

Related blog posts:
- Health Benefit from Disease State: Sucrase-Isomaltase Deficiency
- Disaccharidase Deficiencies in Recurrent Abdominal Pain
- Congenital Sucrase Isomaltase Deficiency
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.