I Novak, NK Velazco. Pediatrics in Review; 2024: 45: 175-187. Gastrostomy Tubes: Indications, Types, and Care
Thanks to Patrick Reeves for sharing this reference. While reading this article, I was reminded of Debbie Mason RN. She worked mainly for Colin Rudolph when I was a fellow at Cincinnati. She would teach the fellows the ‘ins and outs’ regarding gastrostomy tubes (GTs).
Some of the points from this article:
- Background: In one large study, 25% of hospitalized pediatric patients in 63 U.S. hospitals required a temporary NG tube. GTs “preferred for longer-term access due to being less prone to accidental dislodgement, blockage, and interruption of feeds. They are also more durable, discrete, and avoid nasal trauma.” They are probably safer too for longer-term use. (An omission in the article: AMT bridles can help maintain NGs.)
- Indications: Reviews the extensive list of reasons for GT placement, most related to inadequate nutritional intake (related to many chronic disease processes)
- Contraindications are reviewed. “Absolute contraindications include active sepsis or peritonitis, massive ascites, uncorrectable coagulopathy, portal hypertension with significant varices, and history of total gastrectomy.” Transoral PEG tube is contraindicated, as well, if pharyngeal or esophageal obstruction, malrotation, or colonic interposition.
- Preprocedural evaluation is described. Some have recommended UGI prior to placement in those with congenital anomalies. Others have stated that “even congenital anomalies should not mandate an upper GI series given how rare malrotation is in general.” Many children benefit from NG feeding trials prior to GT placement which can also improve nutritional status preoperatively.
- The placement methods and types of GTs are reviewed. “As of now, there is no clearly identified optimal technique” (eg. laparoscopic GT vs PEG). The others note a meta-analysis of 22 studies (n >5000) found a higher rate of major complications with PEG placement. The authors recommend T-fasteners if GT balloon is used for initial placement.
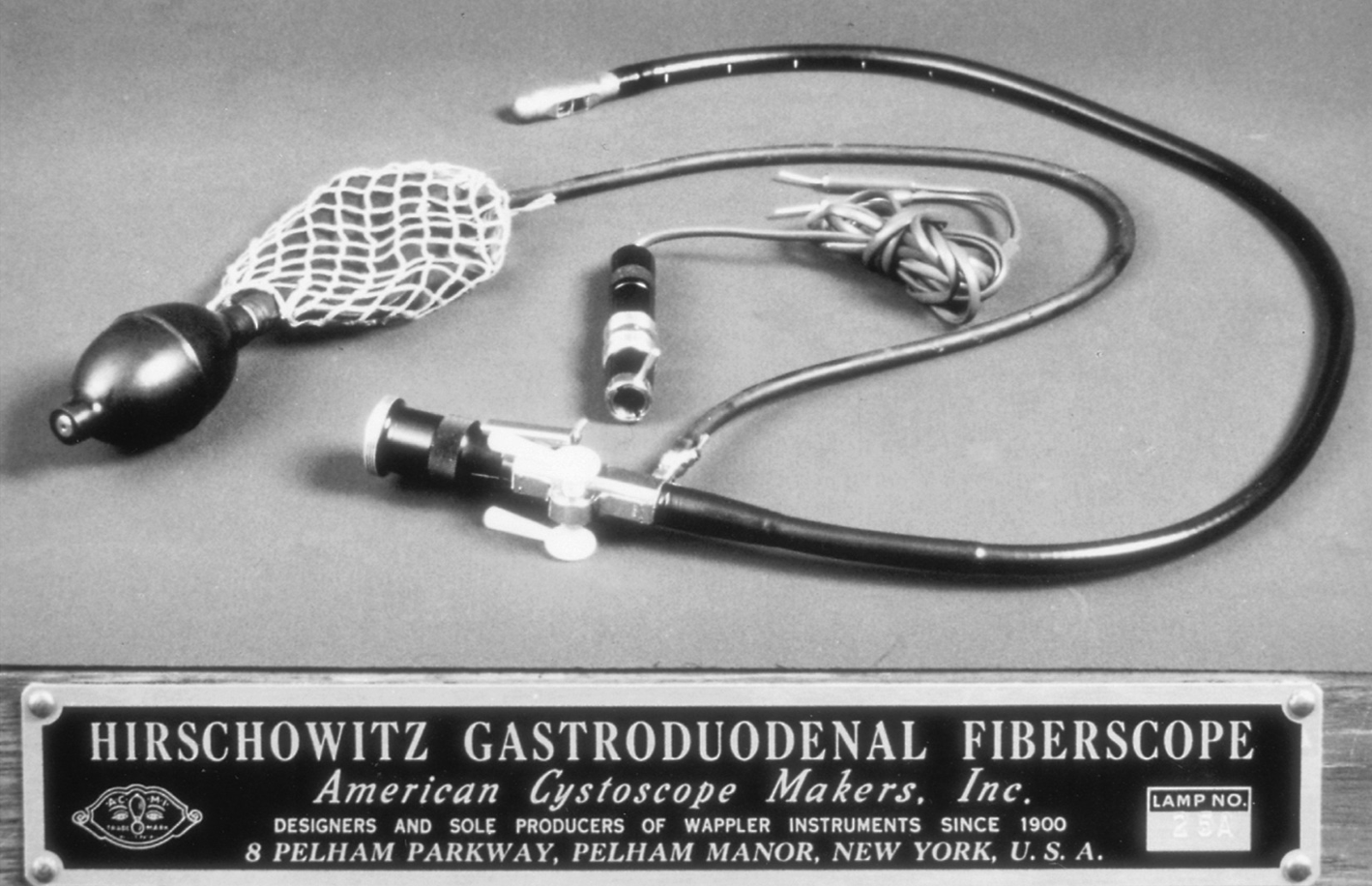
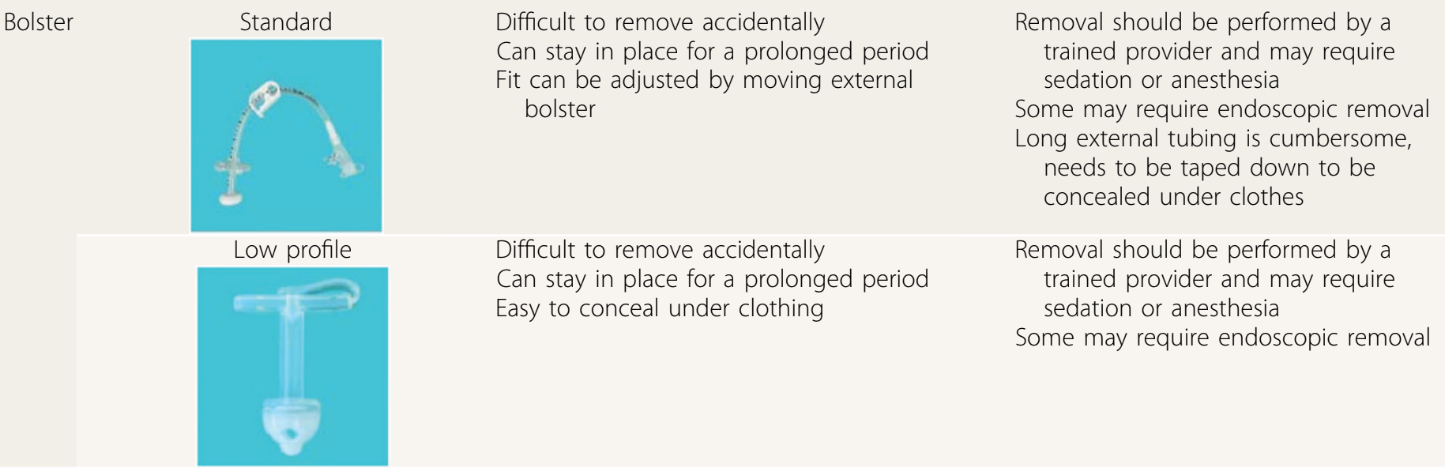
- Examples of bolster-type (non-balloon) GTs:
- GT complications are discussed including infection, peritonitis, bleeding (rare to need a transfusion), injury to adjacent organs, pneumoperitoneum (usually benign and transient), hypergranulation, cellulitis (often treated with a first-generation cephalosporin or topical mupirocin), dislodgement, tube migration, and buried bumper syndrome. For early dislodgement (especially first 4-6 weeks after placement), blind reinsertion should be avoided.
- GT care: The authors recommend starting feeds “not more than 3 to 6 hours” after placement to monitor for immediate postoperative complications, and cleaning site with warm water, saline or soap. Once the site has healed showering and bathing can resume; swimming can be permitted a few weeks after placement. Medications should be given via gastric port (if GJ) for better absorption of medications and lessen risk of tube clogging.
- Troubleshooting: This is the most useful part of this article. Advice on peristomal leakage: “Placing larger tubes should be avoided because this will only enlarge the stoma tract…removal of the tube for a few hours can be considered because this permits the tract to start closing.” Leakage is often due to issues with balloon volume, poor fit, gastric pressure (eg dysmotility, gastroparesis) and poor wound healing. Clogging: “Carbonated beverages, juices, and meat tenderizer…studies have not shown these to be effective.” Lukewarm water, left to stand 20 minutes, is the first line agent for declogging. Other options include commercial enzymatic decloggers, and mechanical decloggers.
- GT removal is discussed and I disagree with the authors that “persistent gastrocutaneous fistulas are rare after removal” (though the majority will close with conservative management). The authors do not recommend cutting GT bolsters due to risk of obstruction and note that endoscopic removal is often necessary.
My take: This article would be well-positioned as part of any GI fellows’ required curriculum and has a bunch of pointers for experienced clinicians as well. It could easily be used for material for ABP questions too. The article is much more detailed than the summary I have provided.
Also, another relevant resource (not discussed in article): Oley Foundation (oley.org). This foundation aims to help those living with home IV nutrition or tube feeding through advocacy, education, community and innovation.
Related blog posts:
- Gastrostomy Tube Recommendations in Pediatrics
- Reducing Gastrostomy Tube Placement in Children with Aspiration & COVID-19 Tracking
- Does Gastrostomy Tube Placement Lower Rates of Hospitalization?
- Less stress after gastrostomy tube placement
- Gastrojejunostomy Complications Frequent
- Updated ESPGHAN Percutaneous Endoscopic Gastrostomy Position Paper
- Helpful Position Paper: Percutaneous Endoscopic Gastrostomy in Children
- 5 Signs Your Child Needs a Feeding Tube
- Is a Laparoscopic Gastrostomy Better Than a Percutaneous Endoscopic Gastrostomy?
- Impact of NG Feeding Program for NICU Graduates
- Complications with G-tube Placement (reports 2015 study with same group)
- Surgery for Reflux Works Best in Those Who Need it the Least | gutsandgrowth