No Exaggeration: Too Many Children Are Dying in the U.S. “The sad fact is that a child or adolescent in the United States is 57% more likely to die by the age of 19 years than those in other wealthy nations.” This is due mainly to more deaths from MVAs and from gun violence.
Link (12-page) Le Bonheur Dysphagia -Thickeners The algorithms suggest starting with oatmeal and then rice cereal for thickening in infants. Recipes are available for how much cereal is needed for each formula based on desired consistency.
This guide reviews the common thickeners including SimplyThick, Nestle ThickenUp Clear, Hormel: Thick & Easy Clear, Gelmix (see below), Purathick, DysphagiAide, Thick-It, Gerber Rice Cereal, Beechnut Oatmeal Cereal
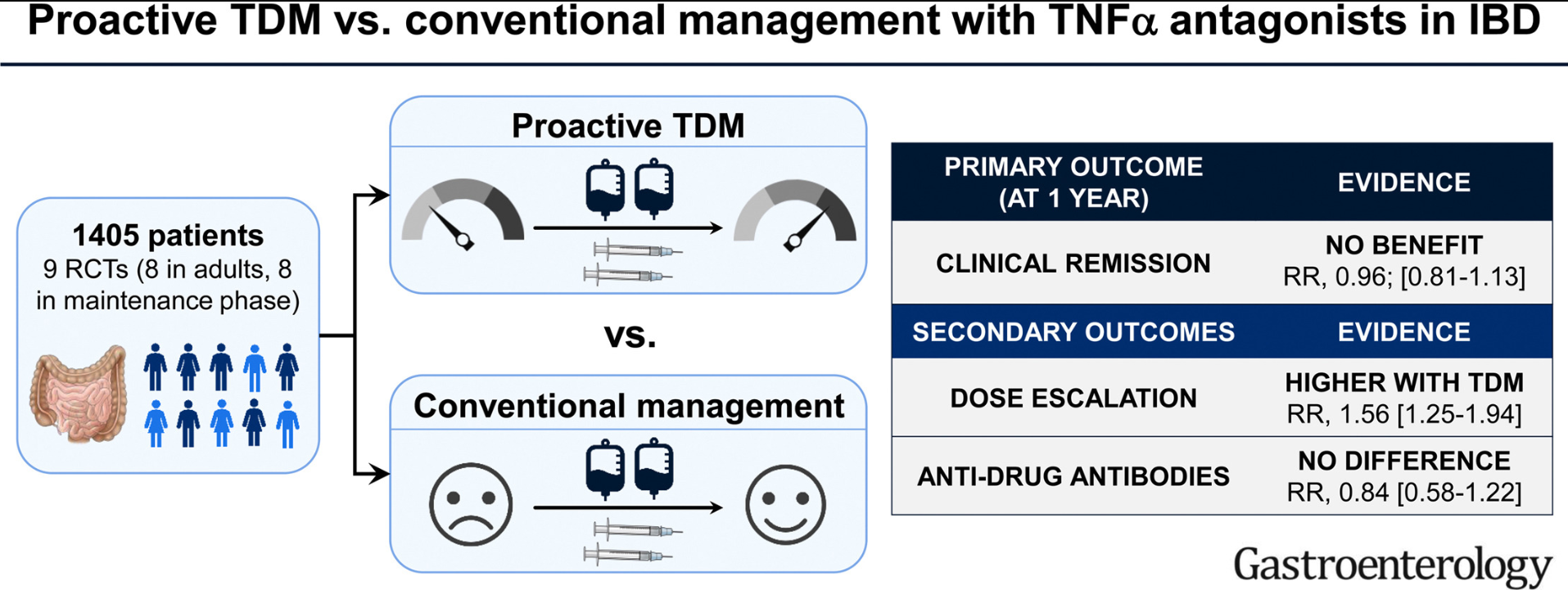
On meta-analysis of 9 RCTs (8 RCTs in adults, and focusing on maintenance phase), there was no significant difference in the risk of failing to maintain clinical remission in patients who underwent proactive TDM (267/709; 38%) vs conventional management (292/696; 42%) (relative risk [RR], 0.96)
The discussion in this paper makes some important points, as there are some populations in which proactive TDM is more likely to be beneficial.
Pediatrics:
“The impact of proactive TDM in pediatric patients also merits further consideration. This concept may be particularly important in pediatrics due to the variability in size of patients, which may not be adequately addressed by weight-based dosing.33 This is especially important in younger children, where it has been shown that standard TNFα antagonist regimens and trough levels may not be applicable in this age group, and may require more frequent escalation of therapy.34,35 In the PAILOT trial, proactive TDM in children with clinical response to adalimumab was associated with higher rates of maintaining sustained corticosteroid-free clinical remission at all visits from week 8–72, compared with reactive TDM in which physicians were informed of trough concentration only after loss of response.”
Induction Dosing (Adults and Children):
“It is possible that the early measurement of biologic drug concentrations, to identify patients who may have accelerated clearance, and optimization of a subset of these patients early in the course of therapy may offer benefit.1,30 …Ongoing trials such as OPTIMIZE (NCT04835506) and TITRATE (NCT03937609) in which infliximab is optimized during the induction phase through a pharmacokinetic dashboard in patients with Crohn’s disease and acute severe ulcerative colitis will shed further light on this.”
My take: So far, studies in adults have not shown that proactive therapeutic drug monitoring has been effective in improving clinical outcomes. This may change particularly if studies focus on patients on monotherapy who are at increased risk of subtherapeutic levels. No matter what happens in adults, there is sufficient data showing that proactive therapeutic drug monitoring is essential in children. This is especially important as ‘routine” dosing of infliximab in children may be subtherapeutic in nearly 80%.
This article makes a compelling case that most U.S. consumers do not know the true risks of alcohol intake; this is likely in part due to the >$1 billion spent each year on marketing by the alcohol industry.
Leading causes of alcohol-related harms:
Fatal and nonfatal injuries resulting from acute intoxication (including injuries caused by motor vehicle crashes)
Chronic diseases including hypertensive heart disease, cirrhosis, pancreatitis and several types of cancer.2 Even light or moderate drinking increases the risk of these conditions, particularly cancer (eg. breast, colon, and stomach)2
Risks during pregnancy include miscarriage, preterm birth, and fetal alcohol syndrome (these risks are not specifically addressed in this commentary)
Also not noted in this article, alcohol is considered a major contributor to violence, including intimate partner violence
Key points –Scope of Problem and Informing Consumers:
“In April 2022, the Centers for Disease Control and Prevention (CDC) released new mortality statistics showing that alcohol consumption now accounts for more than 140,000 deaths per year in the United States, or more than 380 deaths per day. The Covid-19 pandemic has exacerbated alcohol-associated harm in the United States, with alcohol-related deaths increasing by 25% during the first year of the pandemic as compared with the previous year”(White AM, Castle IP, Powell PA, Hingson RW, Koob GF. Alcohol-related deaths during the Covid-19 pandemic. JAMA 2022;327:1704-1706).
“A national survey of U.S. adults, for example, found that nearly 70% are unaware that alcohol consumption increases the risk of cancer.3…Some alcohol companies even seek to link their products to health campaigns. Several companies, for example, have sold seasonal, pink ribbon–themed alcoholic drinks during October to promote their efforts to raise funds for breast-cancer research — despite compelling evidence that alcohol increases the risk of developing breast cancer.”
The authors advocate for better warning labels. They argue that “updated alcohol warnings would provide new risk information to many Americans, … implementing such warnings would be a sensible policy for addressing industry dominance over alcohol-related information, even if warnings’ effects on consumption are fairly small.”
Eric Topol: Paxlovid and Long Covid This in-depth article reviews the benefits of paxlovid (early) and later, including the reduction of Long Covid in 26% in a recent study. It also provides a table for potential drug interactions (Thanks to Jeff Lewis for sharing).
This clinical problem-solving case: “3-year-old boy was brought to the hospital with a 4-day history of vomiting and abdominal pain in the left lower quadrant. He had associated chills without fever, nonbloody and nonbilious emesis, constipation, reduced urinary output, and a decreased activity level.” He developed a rash more than 5 days after presentation.
This turns out to be a good review of IgA Vasculitis (HSP).
A few excerpts:
IgA vasculitis is the most common vasculitis of childhood.1 The disease is classified as a small-vessel vasculitis and most commonly affects White and Asian children, with a slight male predominance. It results from the deposition of IgA immune complexes in involved organ systems and is preceded by infection in most patients.2 This is perhaps unsurprising given the primary function of IgA in mucosal immunity. The most commonly implicated organism is group A β-hemolytic streptococcus.1
IgA vasculitis primarily involves the skin, gastrointestinal tract, joints, and kidneys, with involvement in 95%, 70%, 70 to 90%, and 40 to 50% of cases, respectively, in case series3; other data suggest that kidney involvement is even more common, with microhematuria present in the majority of patients.4 Less common manifestations include orchitis (in 14% of male patients) and, in rare cases, central nervous system involvement.3 Skin involvement is almost universal; a petechial or purpuric rash in dependent areas (typically the buttocks and lower legs) is the classic manifestation, but other skin manifestations, including bullae, edema, and necrosis, can be seen.1,3
IgA vasculitis affecting the gastrointestinal tract can manifest as upper or lower gastrointestinal bleeding. Bowel edema can create a lead point, causing intussusception in up to 3% of patients, as occurred in our patient.1 …In the majority of cases, the rash precedes the onset of gastrointestinal symptoms; our patient was among the minority (approximately 25%) of patients in whom this order is reversed.5 Rare gastrointestinal complications include bowel infarction, perforation, strictures, and protein-losing enteropathy.2,5
I read this article shortly after convincing a surgical colleague to explore a well-appearing 6 month old with gastrointestinal bleeding for a Meckel’s diverticulum rather than undergo endoscopy.
In this retrospective cohort study of hospitalized infants (n=56, =/< 12 months) with gastrointestinal bleeding, the authors reviewed endoscopic procedures (EGD, Colonoscopy, Flexible Sigmoidoscopy) with respect to identifying diagnosis and in terms of outcomes.
Key points:
Seven endoscopies identified sources of GIB: gastric ulcers, a duodenal ulcer, gastric angiodysplasia, esophageal varices, and an anastomotic ulcer.
Intervention for bleeding control occurred in just 3 cases (5.4%); two of these had liver disease.
Most (55%) had no abnormalities on endoscopy
The authors detail two fatal cases in which GIB started in the first week of life. Both had complications occurring within 3 hours of endoscopy, one with a gastric perforation and one with necrotizing enterocolitis.
My take: Endoscopy in infants with GIB is rarely beneficial. Supportive care and surgical interventions should be considered, especially in those without underlying liver disease.
Savage Alpine Trail at Denali National Park. Parts of Denali can be seen in the background
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
In the introduction, the authors note: “Gastroesophageal reflux (GER) is a physiological process defined as the passage of gastric contents into the esophagus with or without regurgitation and vomiting, while GER disease (GERD) is pathophysiologic and occurs when GER is associated with troublesome symptoms and/or complications.”
“This distinction between GER and GERD remains enigmatic among survivors in the neonatal intensive care unit (NICU). Reflux-type symptoms (arching, irritability, acute life-threatening events, coughing, failure to thrive, and swallowing difficulties) in this high-risk infant population can be troublesome to the parent and provider, and empiric management using pharmacological and dietary changes are common albeit with consequences.”
Methods: “Infant Gastroesophageal Reflux Questionnaire Revised (I-GERQ-R) and 24-hour pH-impedance data were analyzed from 94 infants…[and] Longitudinal data from 40 infants that received randomized GER therapy (proton pump inhibitor [PPI] with or without feeding modifications) for 4 weeks followed by 1-week washout were analyzed. Relationships between I-GERQ-R and pH-impedance metrics (acid reflux index, acid and bolus GER events, distal baseline impedance, and symptoms) were examined and effects of treatments compared.”
Key findings:
Acid-suppressive therapy with feeding modifications had no effect on symptom scores or pH-impedance metrics. Clearance of refluxate worsened despite PPI therapy.
Correlations between I-GERQ-R and pH-impedance metrics were weak or non-existent, indicating that physicians cannot depend only on the questionnaire to diagnose and treat GERD in premature infants.
My take: This study shows that reflux symptoms are unreliable in establishing a diagnosis of reflux disease in infants. In addition, medical treatments were not beneficial in infants with abnormal pH-impedance metrics. Perhaps, it is time to acknowledge that we cannot even agree what reflux “disease” is in (premature) infants.
In this retrospective review with 701 patients, 95 (14%) had a gap in care (mean time without care, 4.8 ± 2.3 years). Key findings:
Patients post-gap had higher endoscopic severity (2.4 vs 1.5; P < .001) and smaller esophageal diameters (11.0 vs 12.7 mm; P = .04).
Strictures were more prevalent with longer gap time (P < .05 for trend). Each additional year of gap time increased odds of stricture by 26%, even after accounting for pre-gap dilation. Additionally, of 67 patients without pre-gap fibrosis, 25 (37%) had at least one fibrotic feature (stricture, narrowing, or requiring dilation) post-gap.
Consecutive adult patients with EoE (n=199) completed a 16-cm functional luminal imaging probe (FLIP) during endoscopy were evaluated in a cross-sectional study. Key findings:
Mucosal eosinophil density was similar between abnormal contractile responses (CRs) and normal CRs (median 34 vs 25)
Abnormal CRs more frequently had reduced esophageal distensibility (distensibility plateau <17 mm in 56% vs 32%), with more severe ring scores, and a greater duration of symptoms (median, 10 y vs 7 y)
Thus, abnormal esophageal CRs were related to EoE disease severity, especially features of fibrostenosis. This study suggests that esophageal wall remodeling, rather than eosinophilic inflammatory intensity, was associated with esophageal dysmotility in EoE.
My take: Despite my satirical title, I think these articles are helpful by documenting that ongoing EoE results in worsening esophageal dysfunction/dysmotility (especially if not treated). In addition, they provide insight into the natural history/pathophysiology of EoE.
Heads up! Next year’s Aspen Pediatric GI Meeting will be July 10-14 -terrific learning experience and opportunity to mingle with some exceptional leaders in our field:
In this prospective ‘real-world’ study (adults and children), “cumulative data from each infusion (INF), weight, albumin, C-reactive protein, IFX dose, IFX trough level, and antidrug antibody presence were used to inform subsequent INF dosing.” Key findings:
69% of patients (n=180) required accelerated dosing by the 4th infusion dose. In addition, median dosing intervals were accelerated by ~2 weeks for the 3rd infusion and ~4 weeks for the 4th infusion
The authors report only 6% did not receive a 4th infusion. This early treatment failure rate is much lower than prior studies.
123 of 180 remained on infliximab at week 52 (~32% failure rate); however, this rate is overestimated as there were 26 patients who were not considered failures but were changed to home infusions, moved or lost to followup.
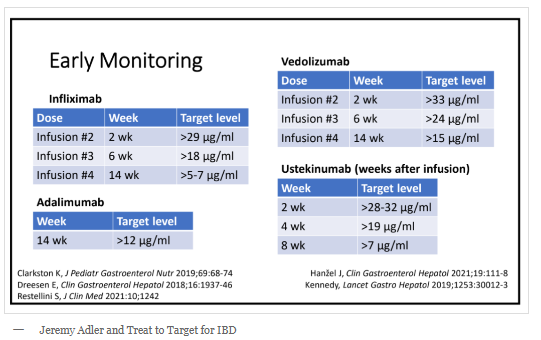
My take: The 8-week interval between induction dose (3rd) and maintenance dose (4th) is too long for many pediatric patients. For those using proactive therapeutic monitoring, checking a level prior to 3rd dose should be considered. Using an automated dosing system (like “iDose”) is likely to be helpful in optimizing response. Current target levels for TDM noted in recent post: Selected Slides from NASPGHAN 2022 Postgraduate Course (part 2) & copied below.
Methods: Within the IQVIA Legacy PharMetrics Adjudicated Claims Database, the authors identified pediatric patients (n=68) with UC who underwent proctocolectomy with IPAA between January 1, 2007, and June 30, 2015. Key finding: In the first 2 years following IPAA, the cumulative incidence of pouchitis was 54%. My take: Most patients continue to experience significant problems after “curative” surgery.
The 6th International Symposium on Peadiatric Inflammatory Bowel Disease (PIBD) was held on September 7-10, 2022, in Edinburgh, Scotland. Highlights of several featured presentations (including video presentation on exposome) regarding the latest updates on nutrition and diet are included at this link (courtesy of Nutritional Therapy for IBD website): PIBD Symposium 2022 Nutritional Highlights
Near Denali, AK
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.