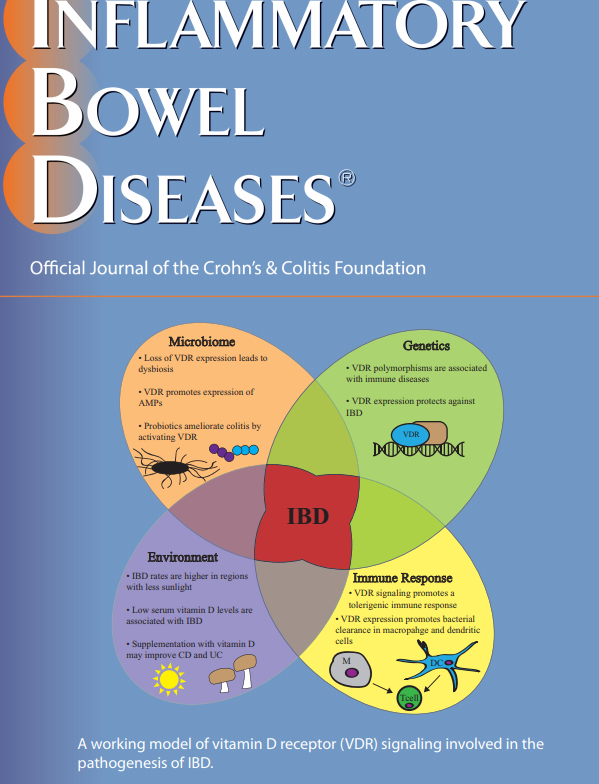
Vitamin D Receptor Signaling in IBD. Inflamm Bowel Dis 2018; 24: 1149-54. This article reviews the ways vitamin D/vitamin D receptor may contribute to the genetic, environmental, immune, and microbial aspects of IBD.
LY Chi et al. Inflamm Bowel Dis 2018; 24: 1344-51. This study with 223 pediatric patients & young adults found that current or prior combination therapy with infliximab, compared to monotherapy resulted in higher infliximab levels and lower antibody formation. Combination agent was mainly methotrexate (n=71) rather than thiopurine (n=13). In those with infliximab dose <10 mg/kg, those currently receiving combination therapy had median level of 11.1 compared with 7.0 for prior combination and 5.86 for monotherapy (never combination).
CM Johnson et al. Clin Gastroenterol Hepatol 2018; 16: 900-7. In this retrospective study with 1466 patients with Crohn’s disease, the subset of patients with granulomas (n=187, 12.8%) were associated with a more aggressive phenotype and a younger age at diagnosis (23.6 years compared with 27.9 years; P= .0005). These patients had higher rates of steroid use, narcotic use, more stricturing and penetrating disease along with increase rates of surgery.