This link for the NASPGHAN abstracts :NASPGHAN 2017 Scientific Abstracts
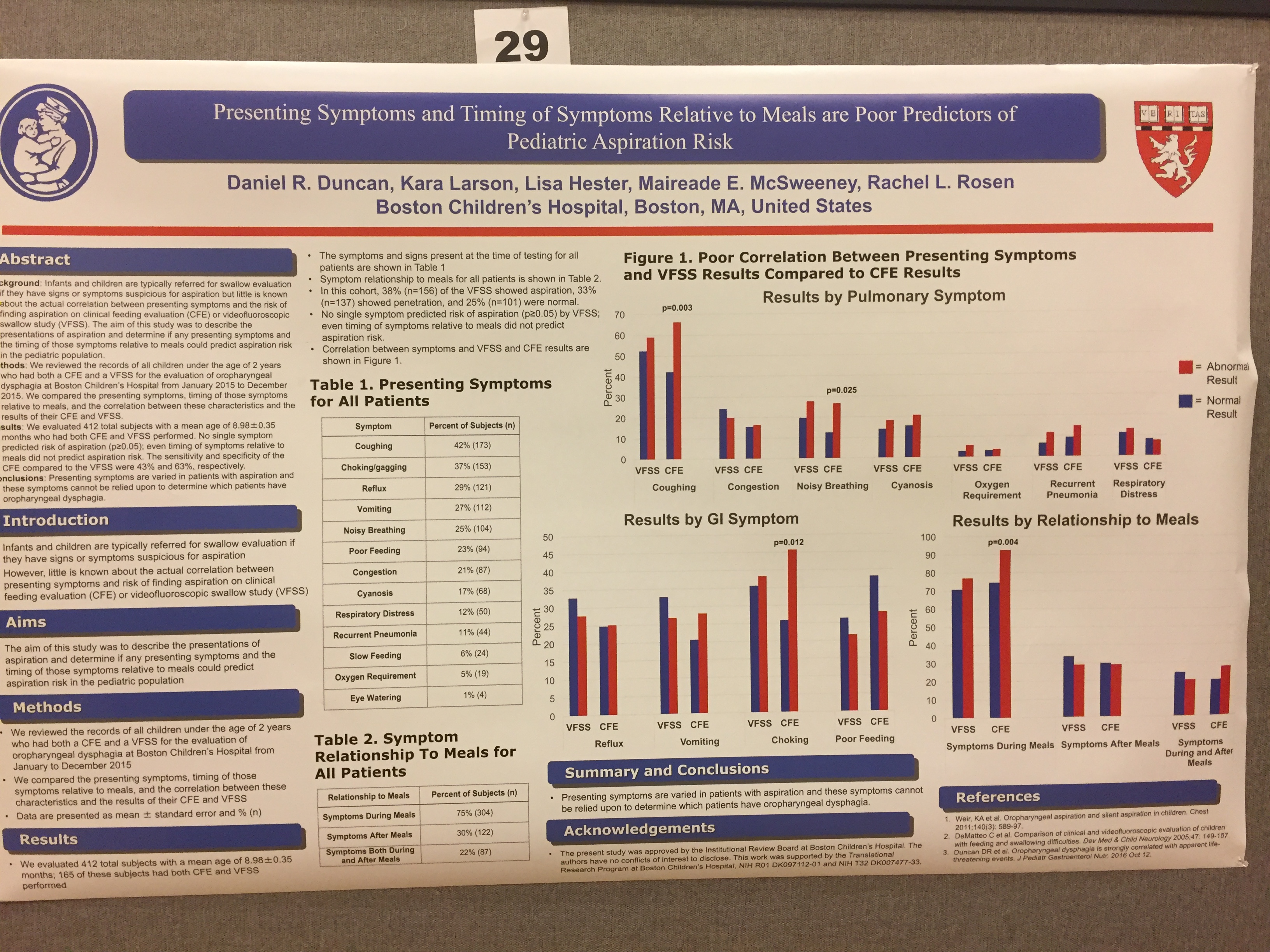
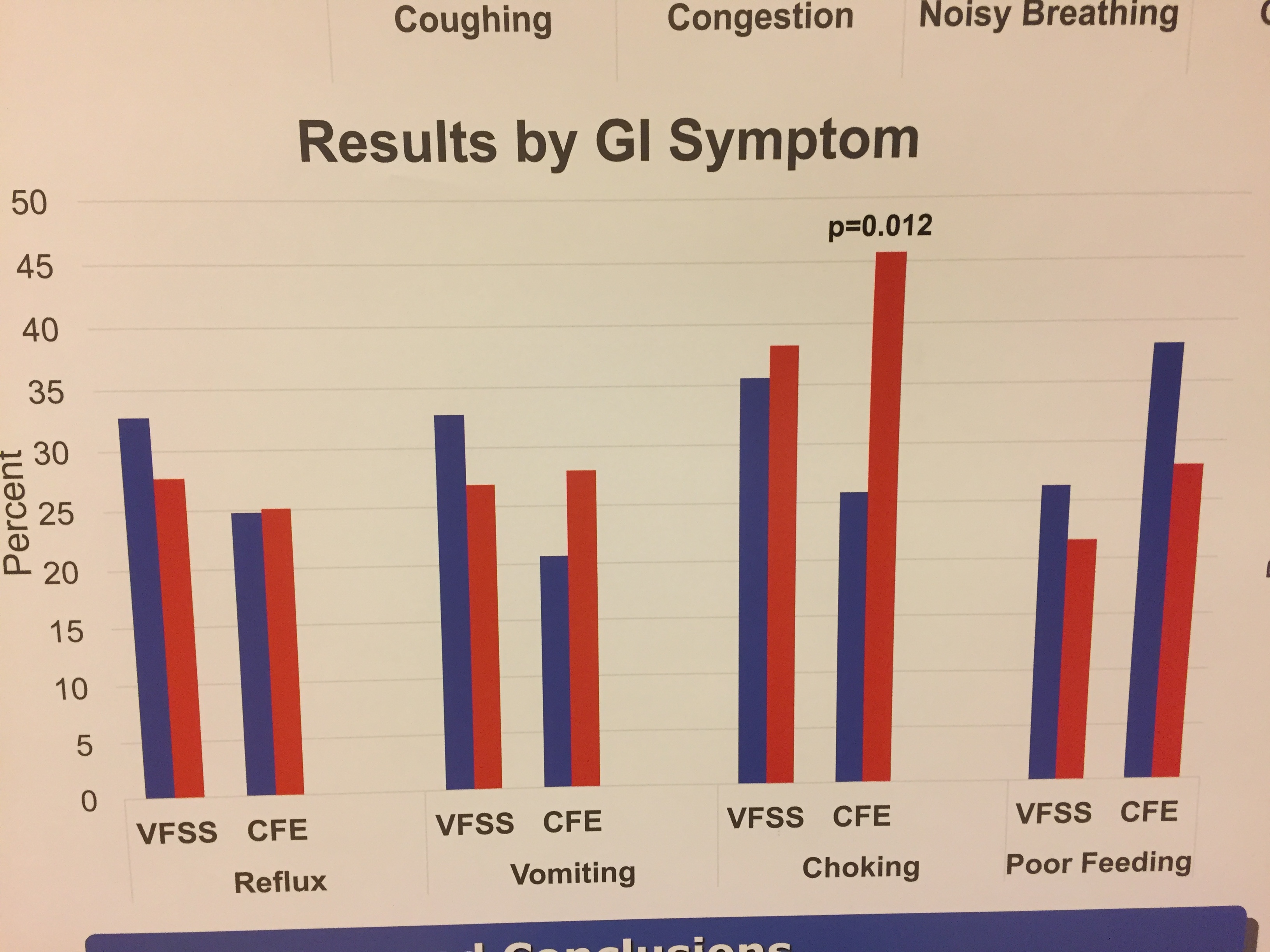
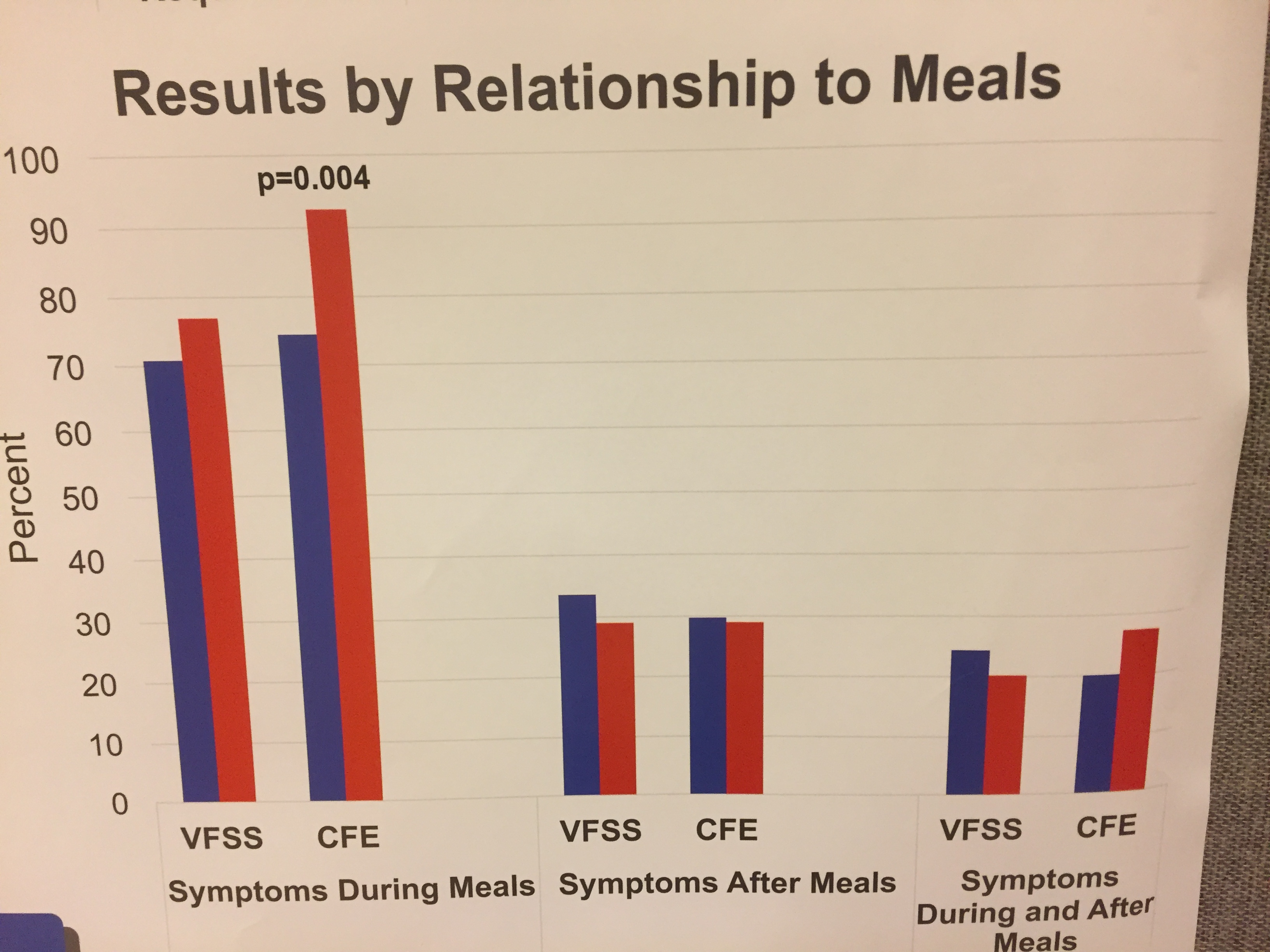
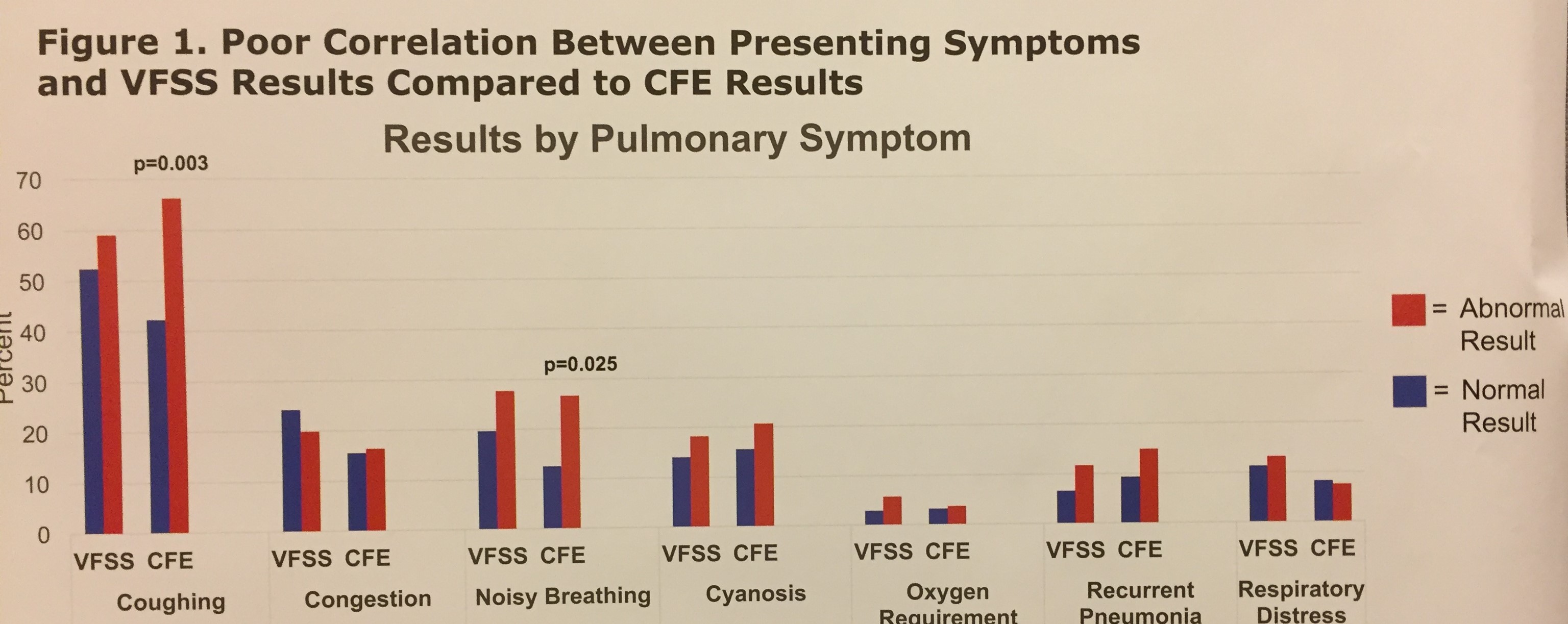
The following slides are from some of the abstract posters. This first poster (next 5 pics) showed that symptom association with meals is not predictive of aspiration among a selected group of children who underwent swallow study evaluations. In the figures, the blue bars are children who passed the swallow study whereas the red bars indicate the children who failed the swallow study.

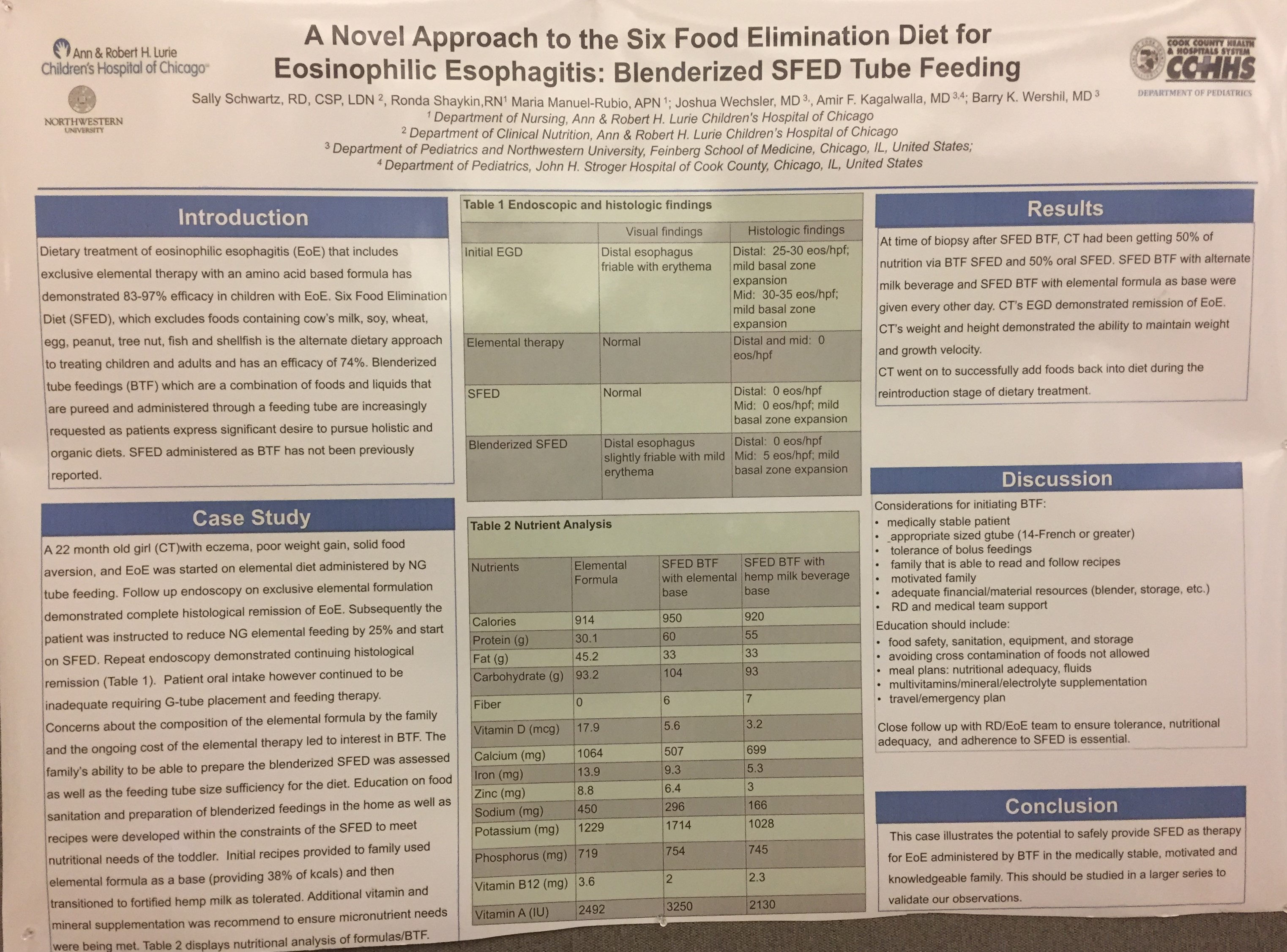
This next slide demonstrated that a six food diet for EoE could be administered blenderized via a gastrostomy tube.
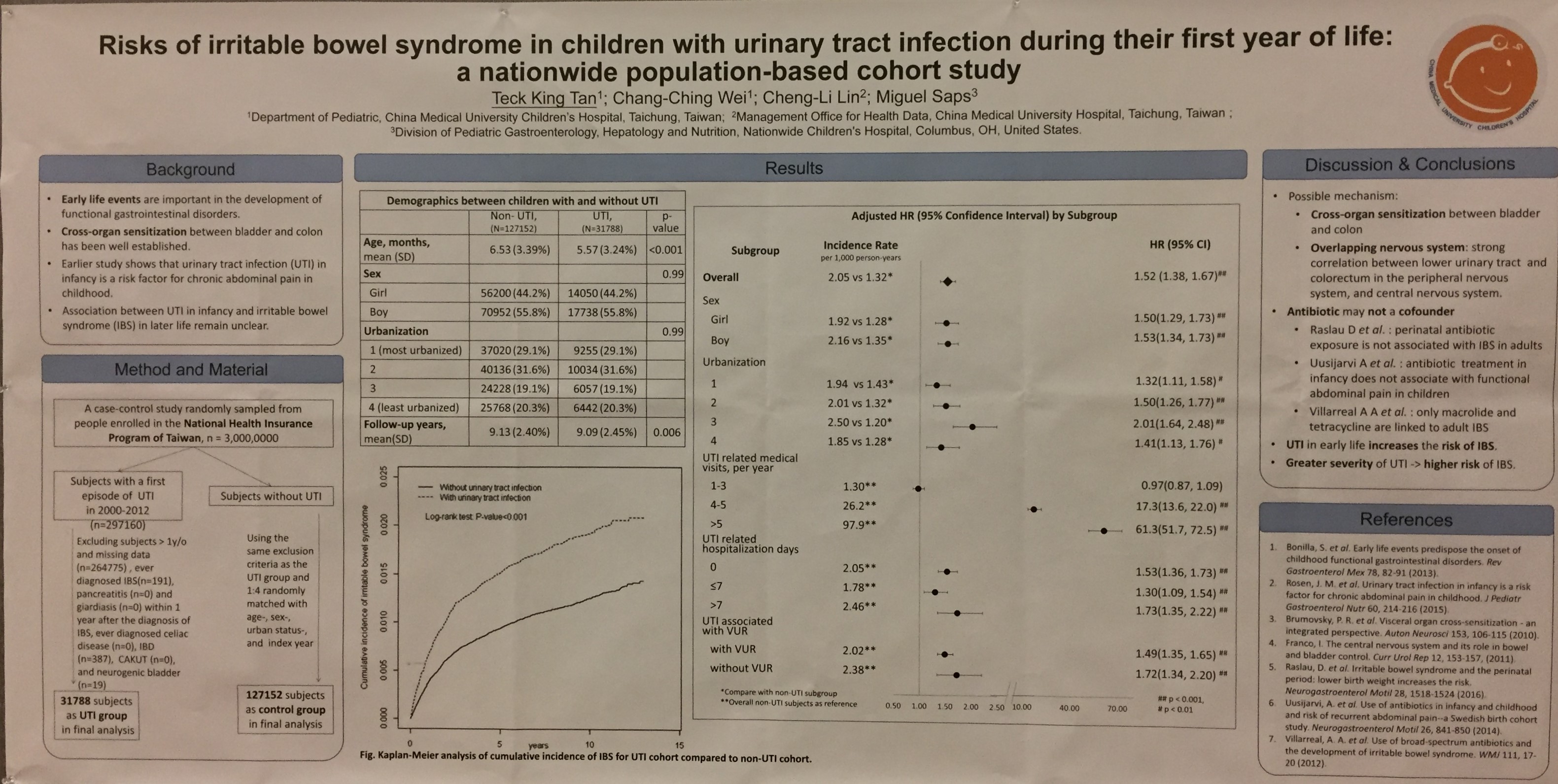
The next slide showed that irritable bowel syndrome was more frequent (overall hazard ratio of 1.52) following a urinary tract infection in the first year of life.
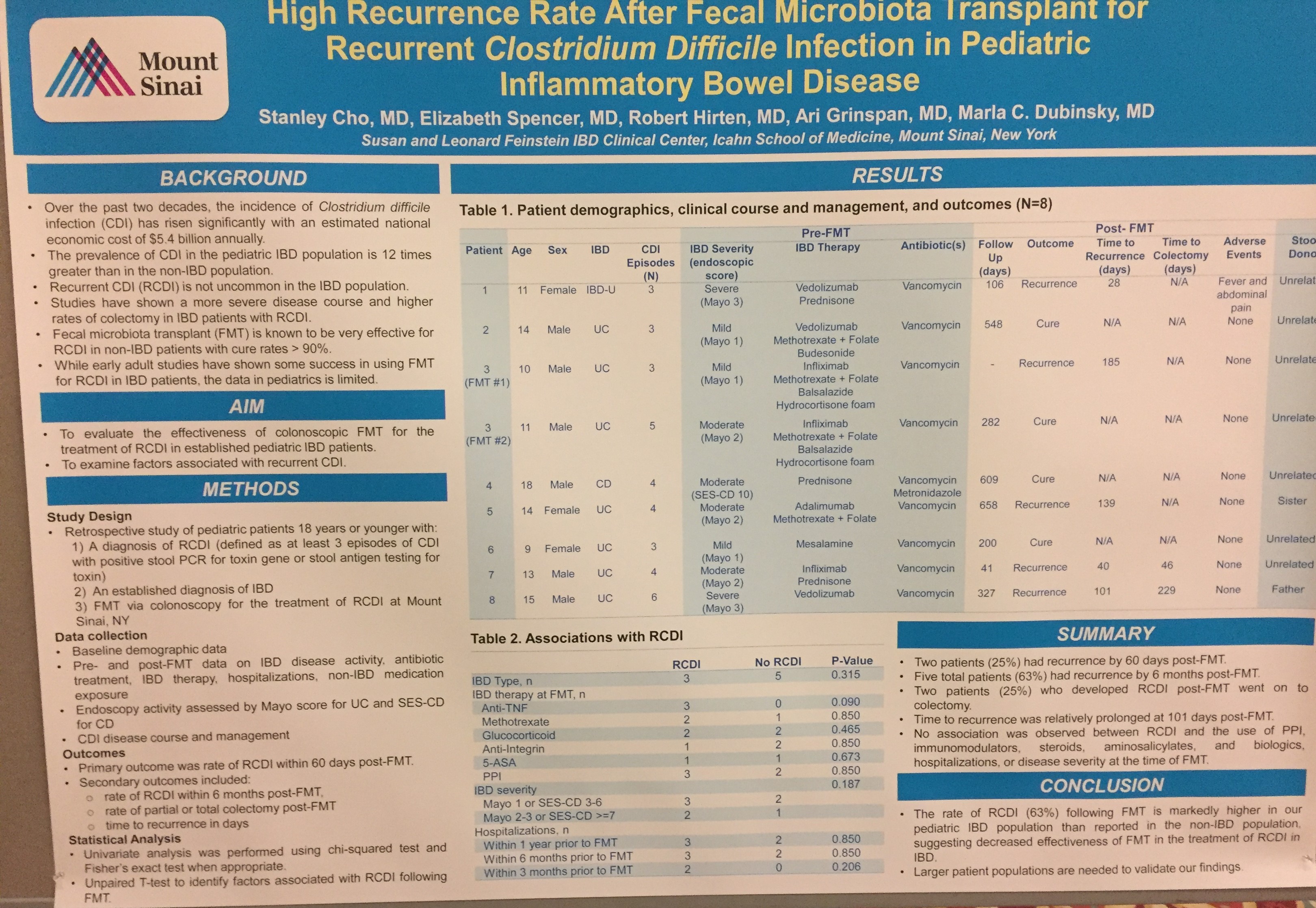
The next pictures are from a poster discussing high rates of recurrent C difficile infection following fecal microbial transplantation in pediatric patients with inflammatory bowel disease (mainly ulcerative colitis). An inference from this study would be that many cases of C difficile that were attributed as causing symptoms could in fact have been from a flare up of their IBD. More details about the diagnosis of C difficile (based on PCR or ELISA) would be helpful
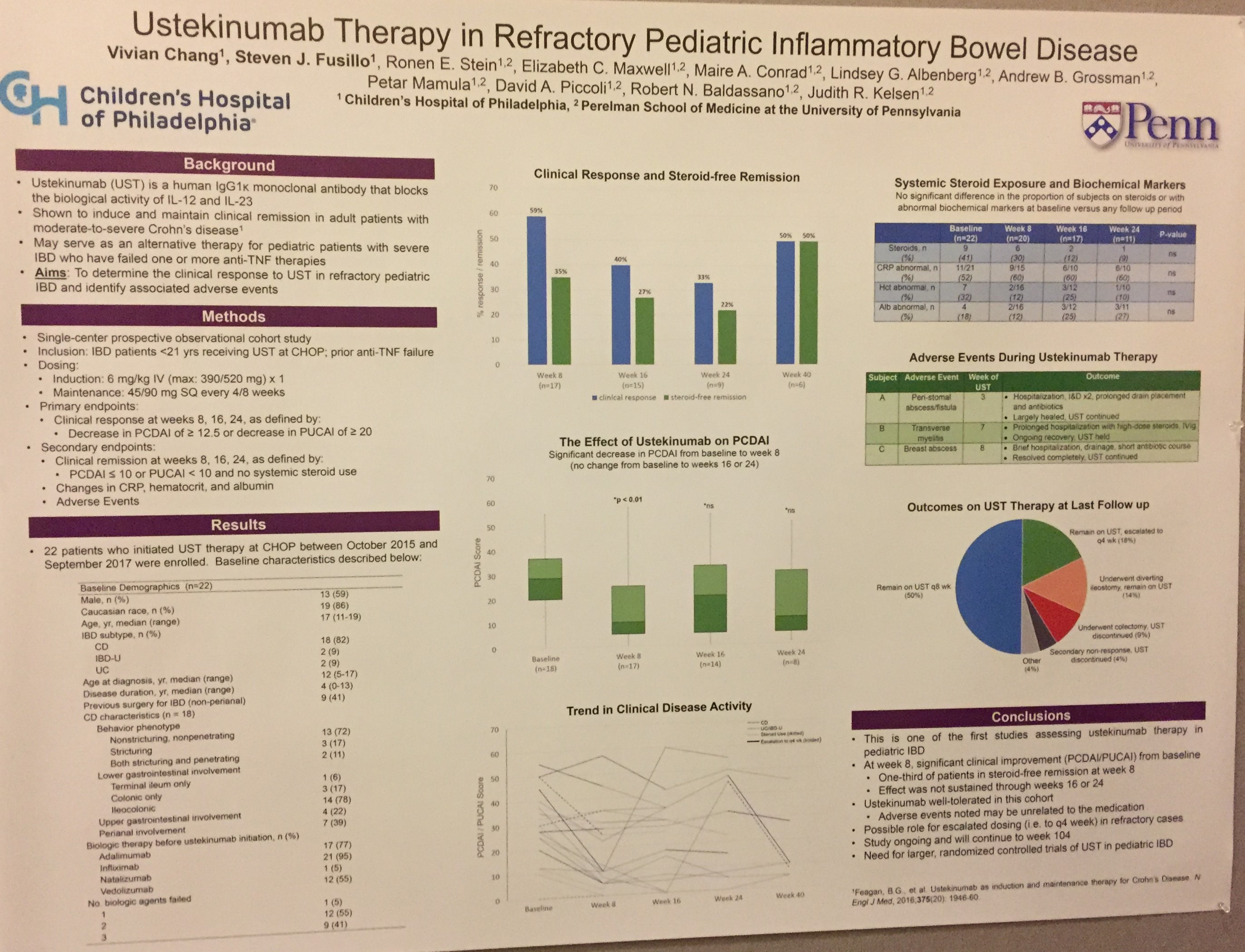
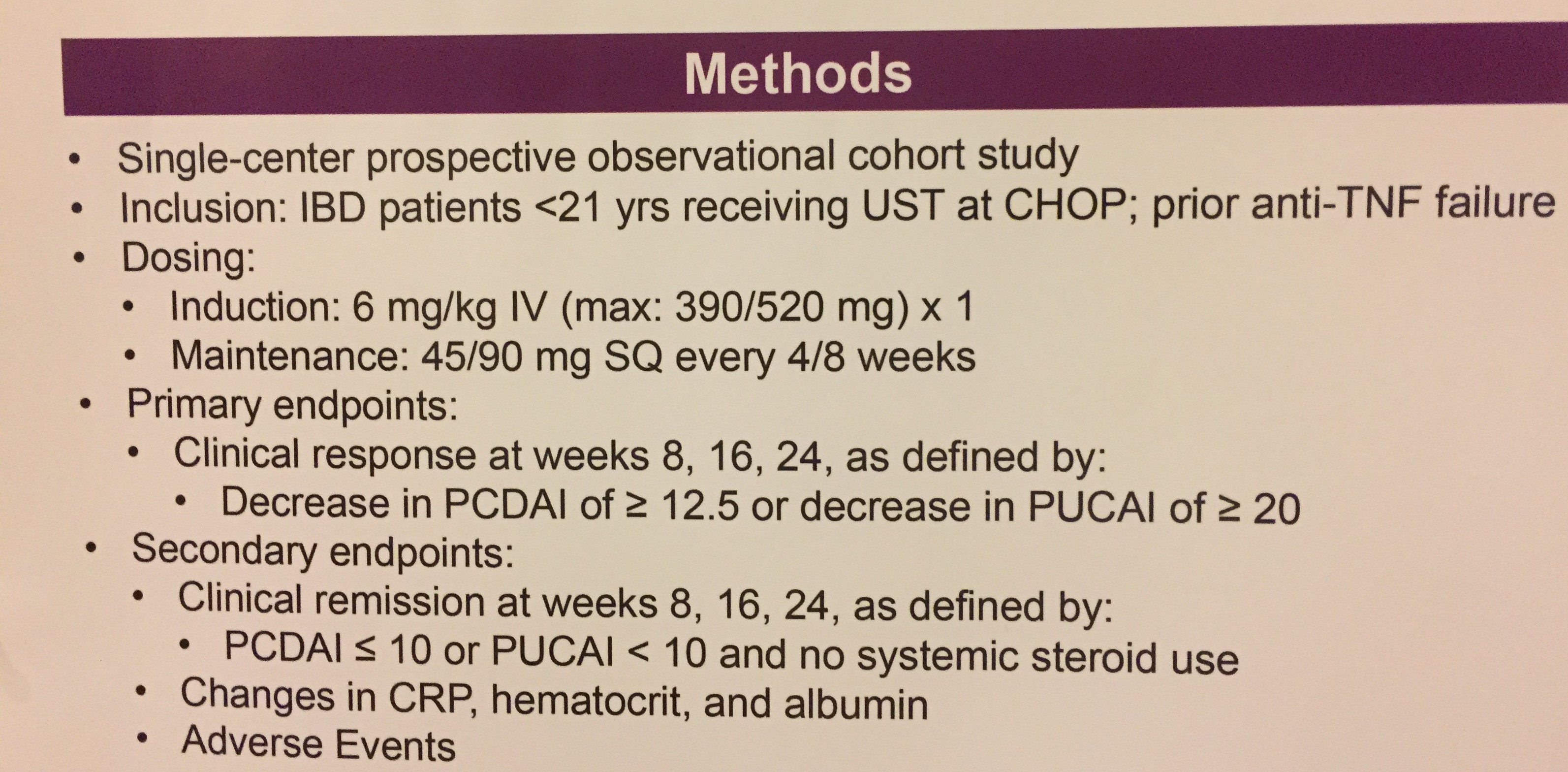
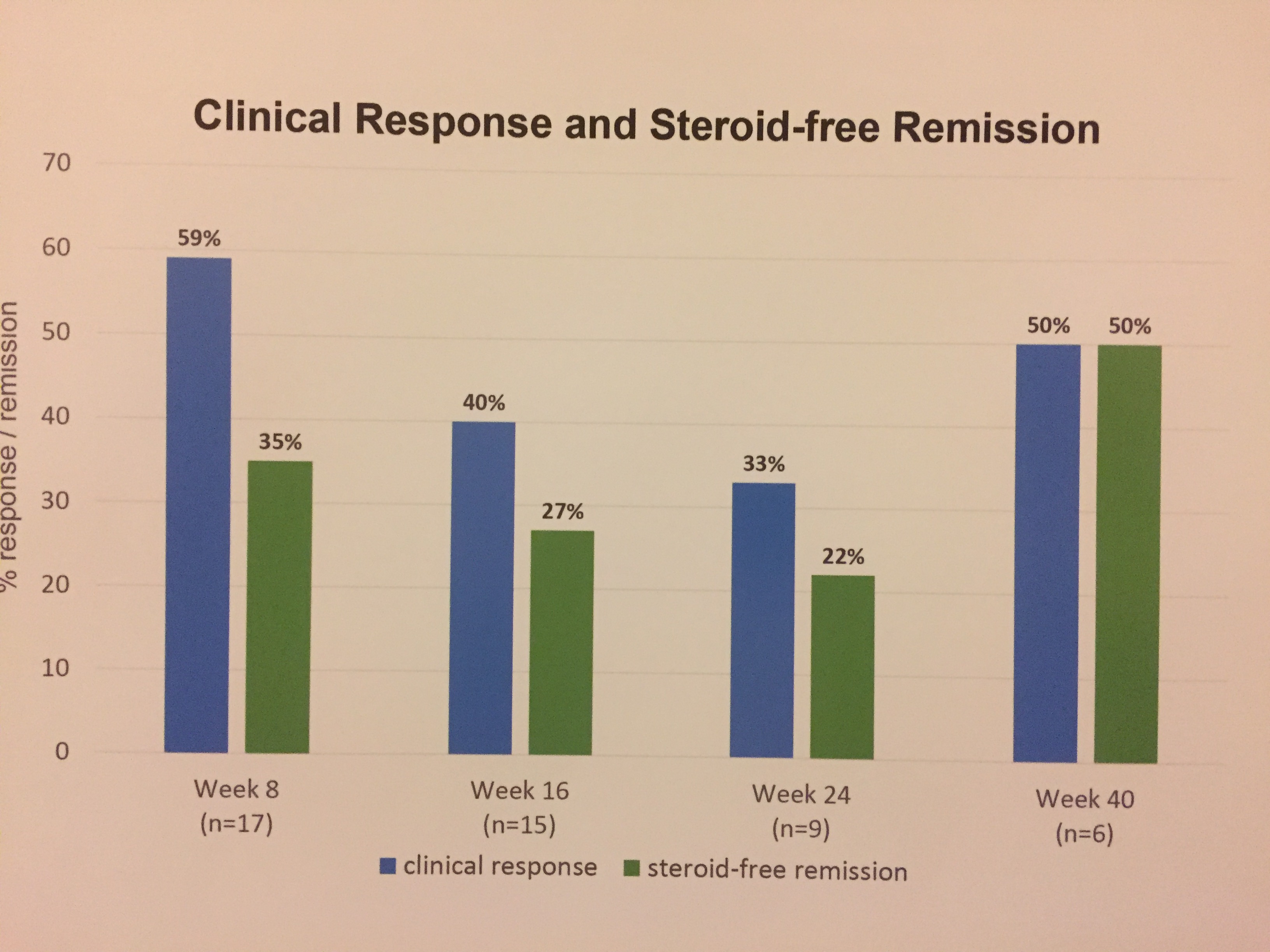
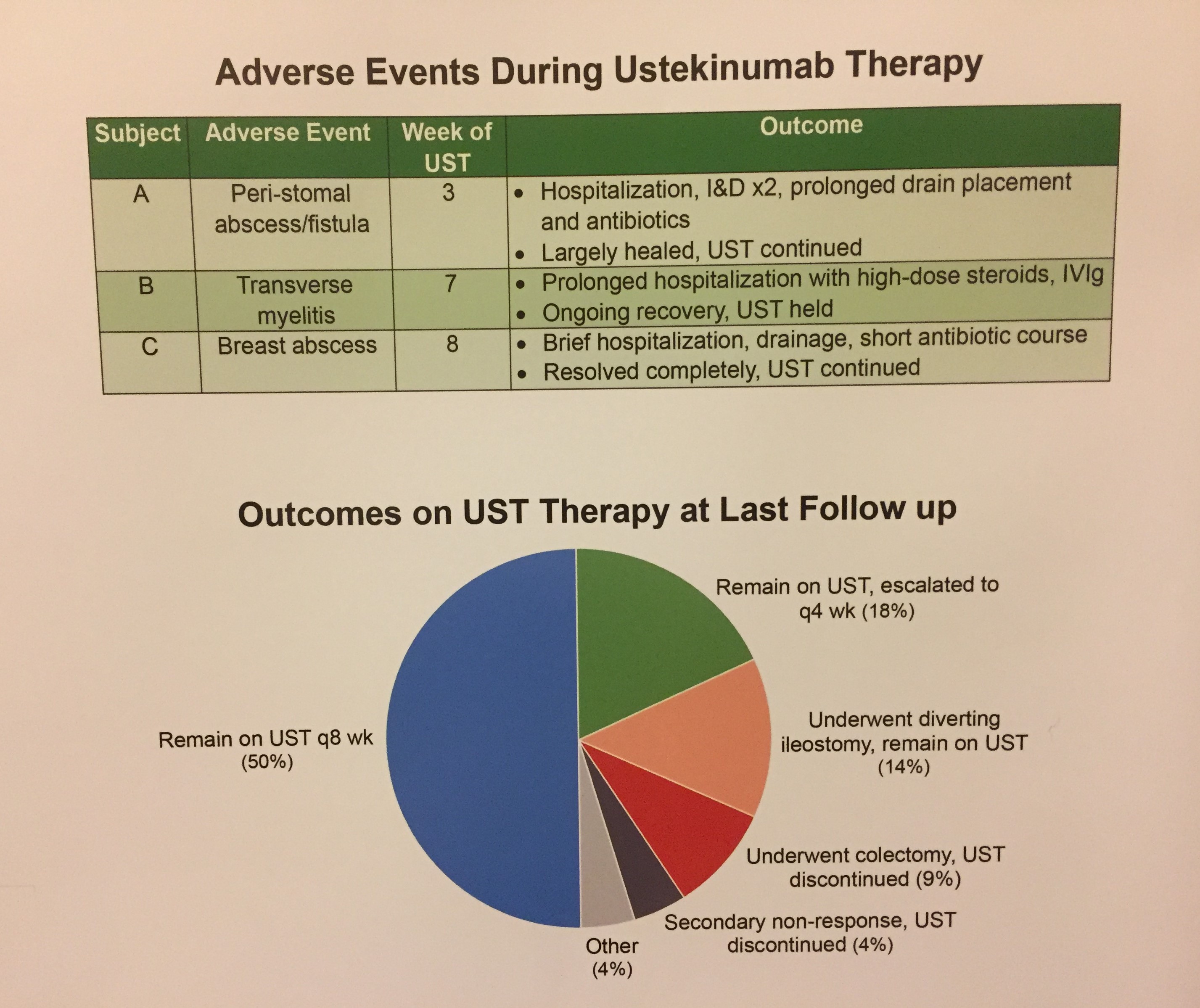
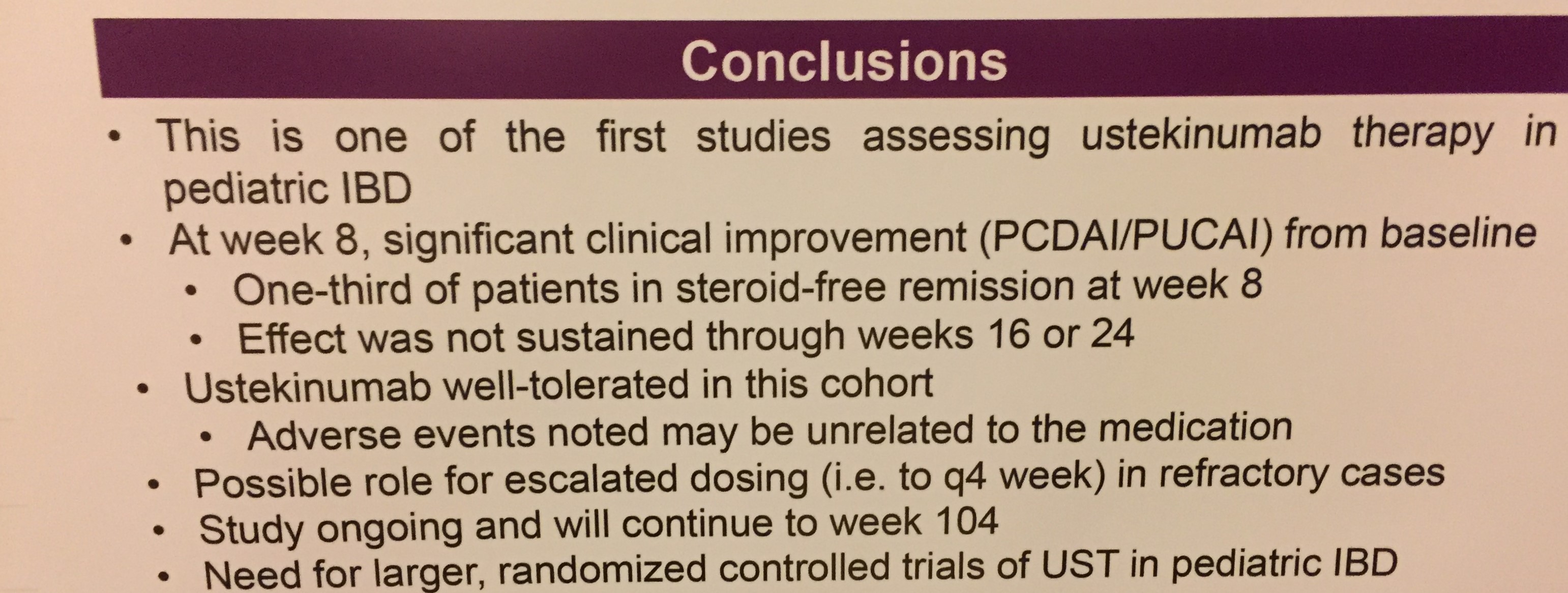
The next poster provides data from CHOP experience with Ustekinumab. Overall, in this highly-selected (refrcactory) population the long term improvement was low; while one-third had steroid-free remission at week 8, this was not maintained at week 16 and week 24. In addition, among the 22 patients, one developed transverse myelitis.
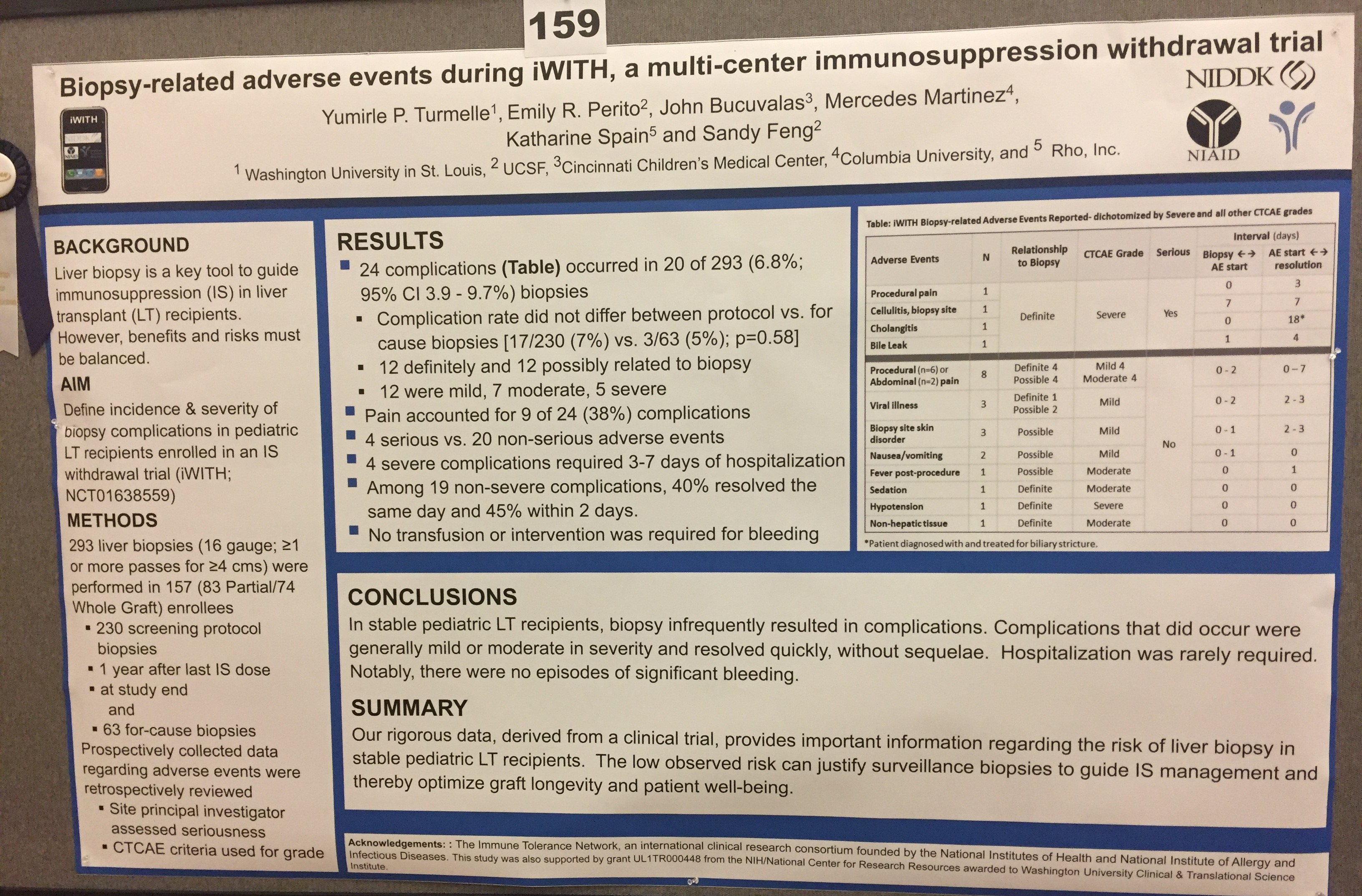
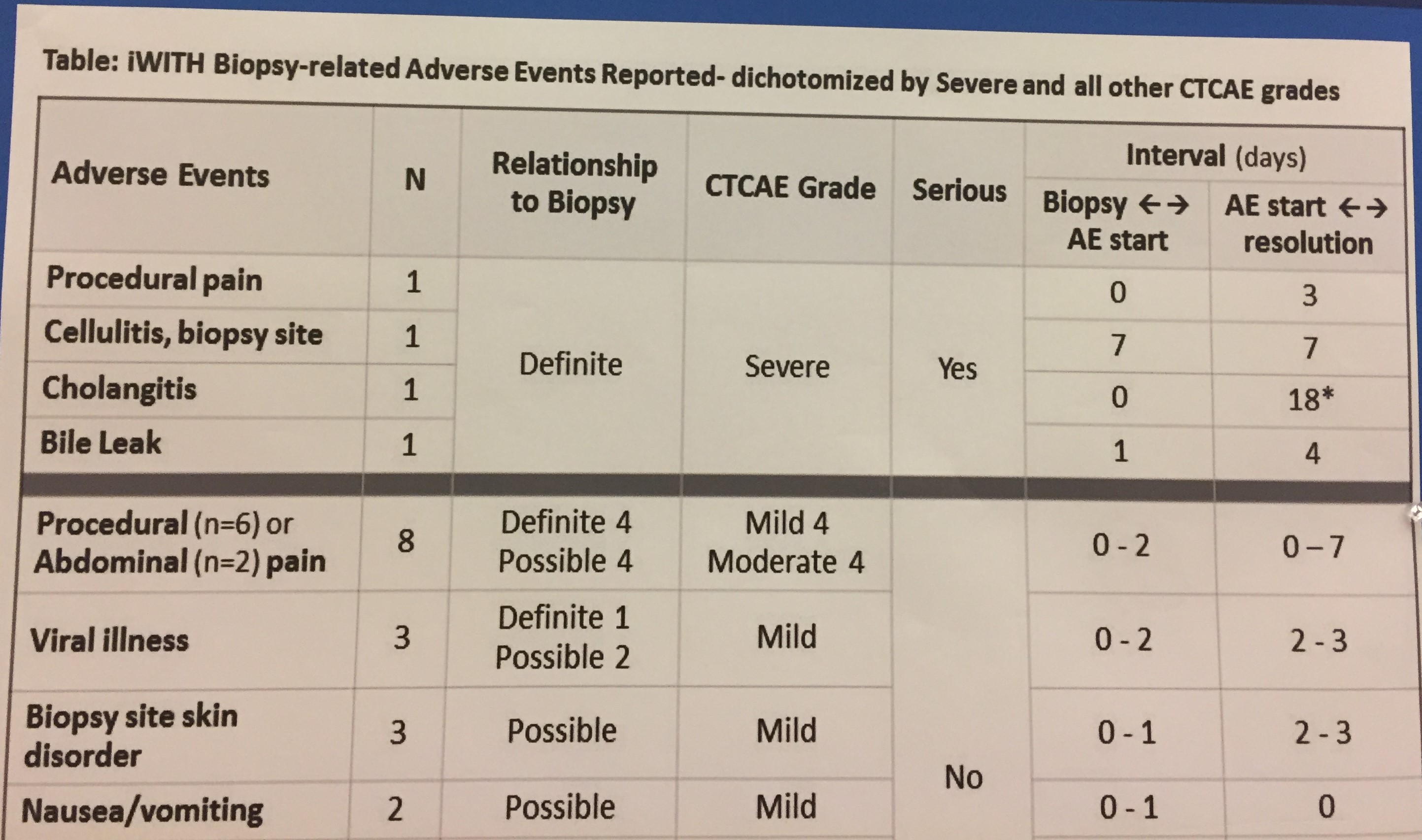
This study that follows (next two pics) documented the relative safety of liver biopsies (mainly percutaneous without interventional radiology) in the post-transplant period. The two most serious adverse events, cholangitis and bile leak, helped identify biliary strictures.
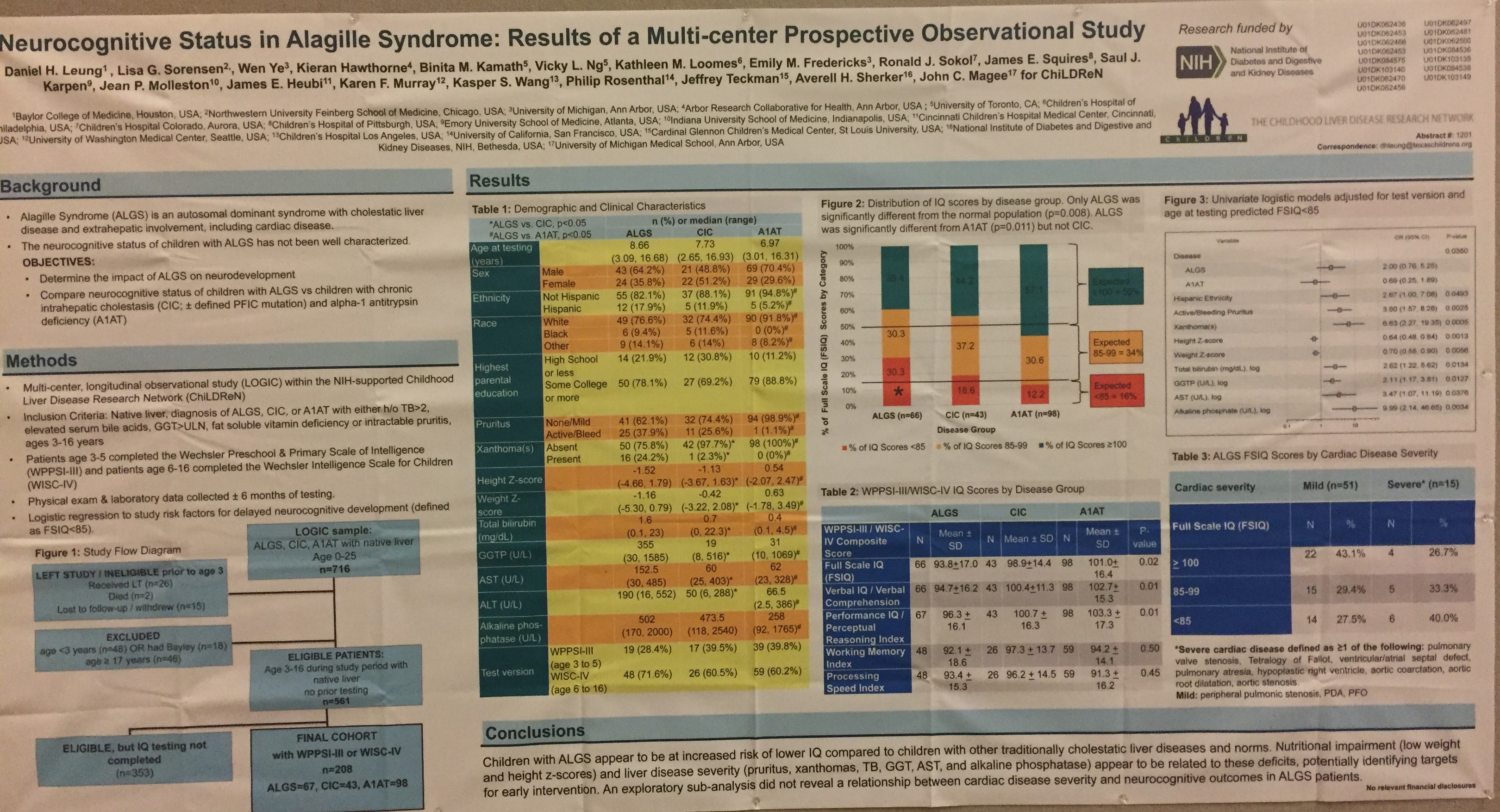
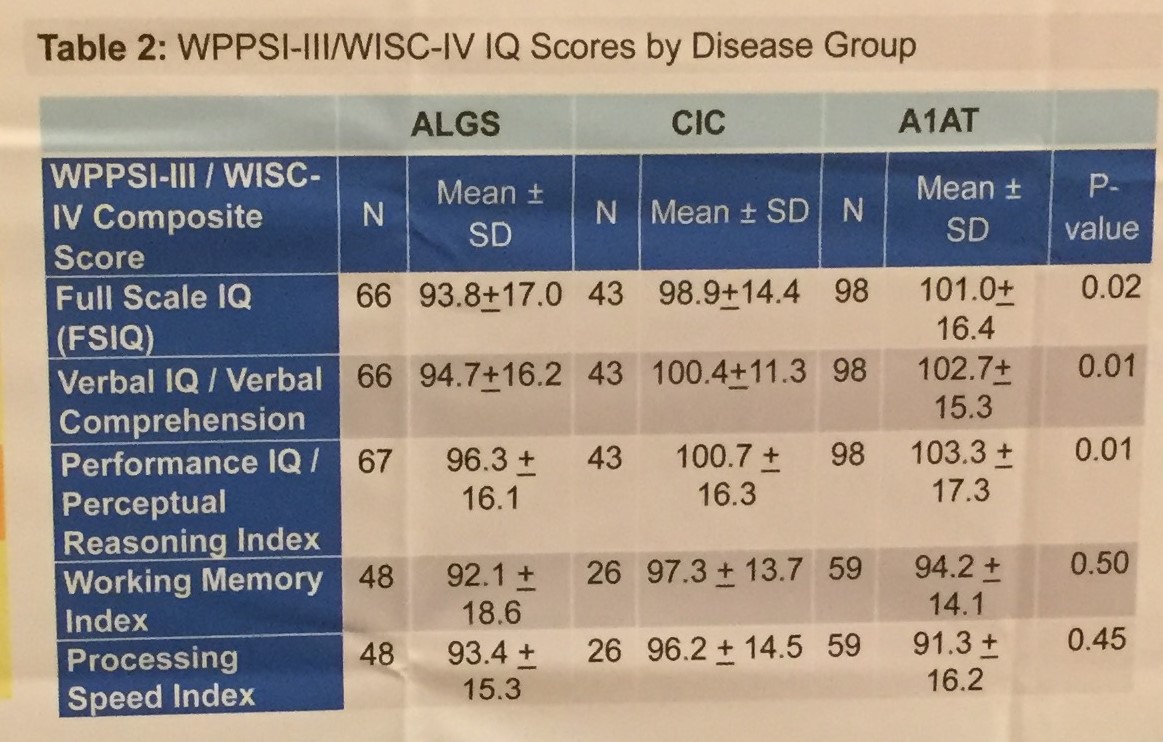
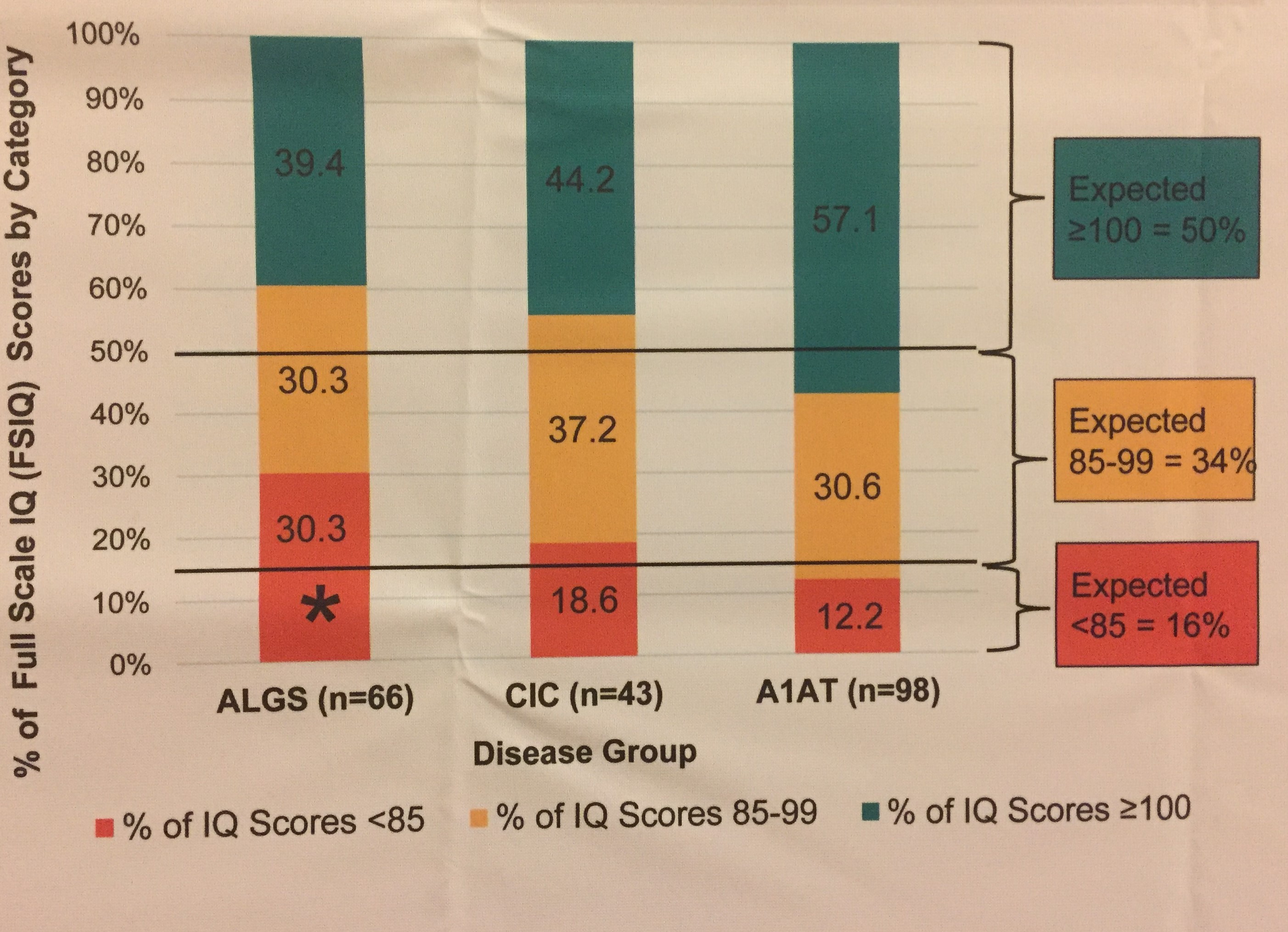
The following collaborative study examined the neurocognitive status of children with Alagille syndrome. Overall, this study shows that children with Alagille syndrome are at increased risk of low IQ compared to children with other cholestatic diseases.
![]()
![]()