COVID-19 Vaccine Effectiveness (8/10/21):

————————————————————————————————————-
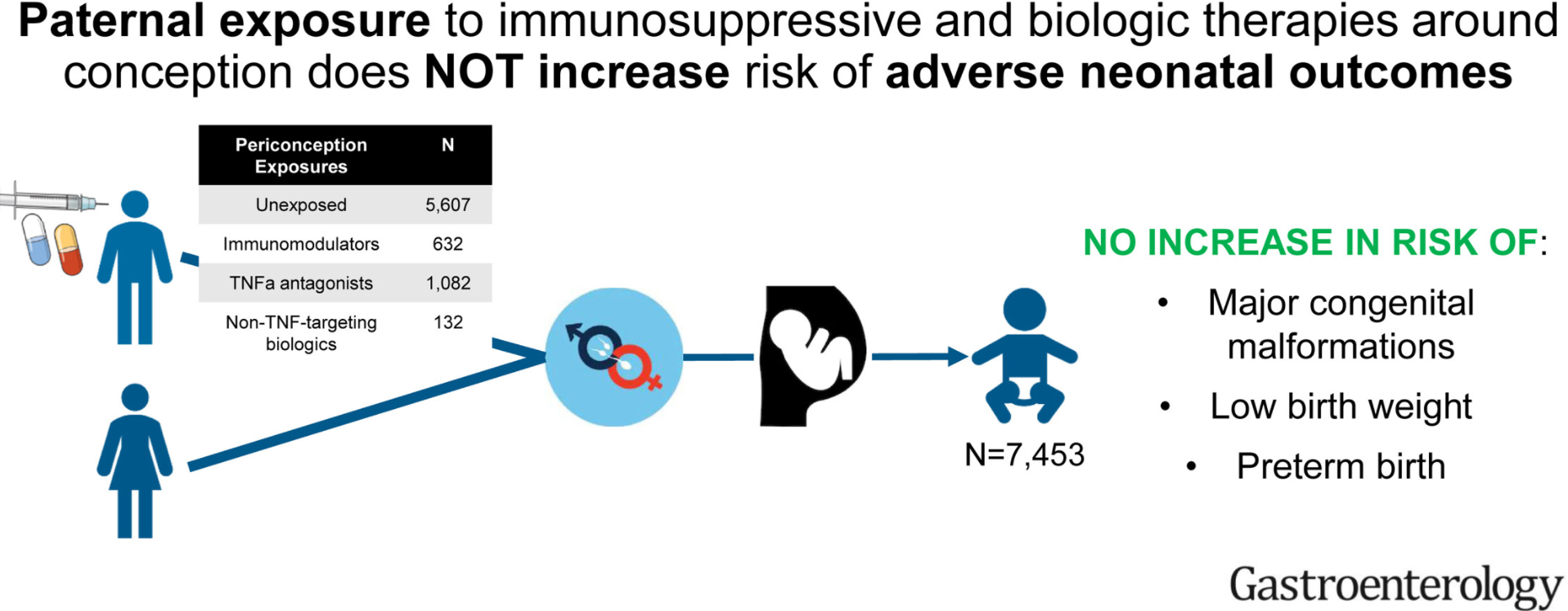
J Meserve et al. Gastroenterol 2021; 161: 107-115. Full text: Paternal Exposure to Immunosuppressive and/or Biologic Agents and Birth Outcomes in Patients With Immune-Mediated Inflammatory Diseases
Methods: The investigators used a deidentified administrative claims database (OptumLabs Data Warehouse) with a total of 7453 expectant fathers with immune-mediated diseases.
Key findings:
- As compared to unexposed fathers (3.4% prevalence of major congenital malformations), exposure to immunosuppressives/biologics were not associated with increased risk of major congenital malformations: thiopurines (relative risk [RR], 1.12; 95% confidence interval [CI], 0.66–1.76), methotrexate (RR, 0.67; 95% CI, 0.21–1.55), TNF-α antagonists (RR, 1.14; 95% CI, 0.81-1.57), and non–TNF-targeting biologic agents (RR, 1.75; 95% CI, 0.80–3.24).
- No association was observed between paternal medication exposure and risk of preterm birth or low birth weight.
Editorial, pg 24-27: S Friedman et al. Full text: Does Fatherhood Matter? Preconception Use of Biologics and Immunomodulators by Fathers With Immune-Mediated Diseases and Birth Outcomes of Their Offspring
“Regarding major congenital malformations, we believe that the results should be interpreted with caution. The numbers of these outcomes are relatively low and the statistical precision of the risk estimates should be taken into consideration.”
My take: Overall, this study is reassuring. Though it is difficult to prove these medications do not have impacts on newborns, if these effects were frequent, it would likely be evident in this type of study.