Because our office is one of the centers participating in a mirikizumab study for adolescents, I was particularly interested in seeing the published results of a phase 2 study in 191 adults.
BE Sands et al. Gastroenterol 2022; 162: 495-508. Open Access: Efficacy and Safety of Mirikizumab in a Randomized Phase 2 Study of Patients With Crohn’s Disease
Summary Video Link (worth a watch!): Summary of Mirikizumab Study (4:25 minutes)
Background: “Mirikizumab (LY3074828) is a humanized immunoglobulin G4 (IgG4)–variant monoclonal antibody that binds specifically to the p19 subunit of IL23 and has demonstrated efficacy in psoriasis and ulcerative colitis, and is currently in phase 3 testing for psoriasis, ulcerative colitis, and CD. We evaluated the efficacy and safety of mirikizumab for the treatment of patients with moderately-to-severely active CD”
Methods: Patients (N = 191) were randomized (2:1:1:2) to receive placebo (PBO), 200, 600, or 1000 mg mirikizumab, administered intravenously (IV) every 4 weeks. Patients who received mirikizumab and achieved ≥1 point improvement in Simple Endoscopic Score-CD at Week 12 (rerandomized maintenance cohort) were rerandomized to continue their induction IV treatment (combined IV groups [IV-C]) or receive 300 mg mirikizumab subcutaneously (SC) every 4 weeks. Nonrandomized maintenance cohort included endoscopic nonimprovers (1000 mg) and PBO patients (PBO/1000 mg) who received 1000 mg mirikizumab IV from Week 12. The primary objective was to evaluate superiority of mirikizumab to PBO in inducing endoscopic response (50% reduction from baseline in Simple Endoscopic Score-CD) at Week 12.
**approximately two thirds of participants had received biologic therapy and approximately half of all patients in this trial having experienced at least 1 biologic failure
Key findings:
- At Week 12, endoscopic response was significantly higher for all mirikizumab groups compared with placebo (PBO) (200 mg: 25.8%, P = .079; 600 mg: 37.5%, P = .003; 1000 mg: 43.8%, P < .001; PBO: 10.9 %).
- Endoscopic response at Week 52 was 58.5% (24/41) and 58.7% (27/46) in the IV-C (combined IV groups) and SC (subcutaneous) groups , respectively. See 4th and 6th slides below which show that those with response at 12 weeks continued with response at 52 weeks.




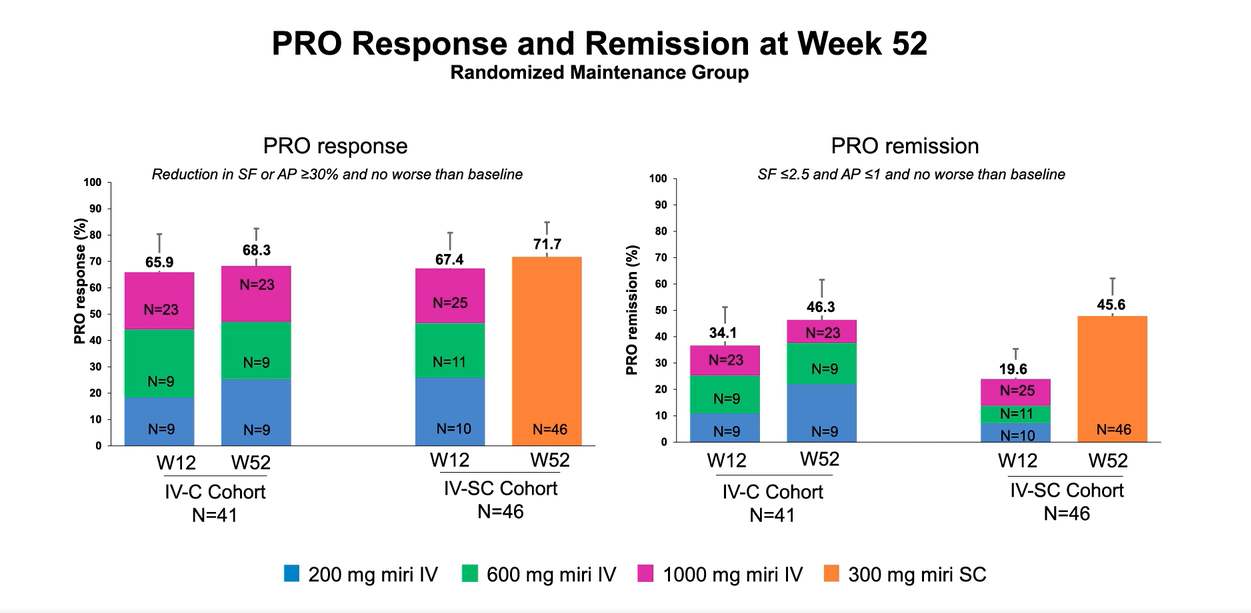


the highest dose, 1000 mg. A significant number of non-improvers responded at week 52.
My take: In this study of adults, with moderate to severe Crohn’s disease, Mirikizumab showed good efficacy and safety at both 12 weeks and 52 weeks. Because about half of the participants were biologic failures, this indicates that this agent shows promise in those with refractory disease.