23.8% of liver transplant recipients reported current MJ use (of 538 who responded to survey
Top reasons for MJ use were recreation (56.5%), anxiety (54.8%), and pain (53.2%)
Among respondents, 21.0% currently used CBD, usually in the form of creams or lotions (58.9%) and to relieve pain (84.9%) and anxiety (31.1%)
The authors note that MJ (marijuana) use previously was not associated with adverse liver tranplant outcomes (in one study); however, there are “there are case reports of drug interactions resulting in tacrolimus toxicity in patients using MJ and CBD.” And, MJ by inhalation may increase the risk for pulmonary fungal/aspergillosis. The use of MJ was similar to previous data in the general Colorado population, “18.1% of adults aged 18 and older in Colorado had used MJ in the past month in 2017-2018, compared with 10.2% of adults nationally.”
My take: Cannaboid use is common in liver transplant recipients and in the general population. More data is needed to understand its safety.
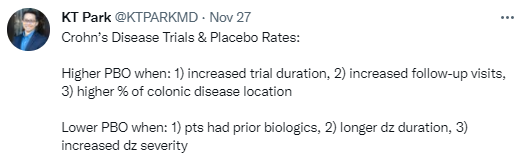
The authors searched MEDLINE, EMBASE and CENTRAL from inception to March 2021. Eligible studies were placebo-controlled trials of pharmacological interventions for CD
Key findings:
In 125 studies (91 induction, 46 maintenance), placebo clinical remission and response rates for induction studies were 18% [95% confidence interval (CI) 16-21%], and 32% (95%CI 29-35%), respectively, and for maintenance studies were 28% (95%CI 23-34%) and 30% (95%CI 24-37%), respectively
Endoscopic remission and response rates (for placebo) in induction studies were 8% (95%CI 4–18%), and 16% (95%CI 11–23%), respectively
Trials enrolling patients with prior biologic exposure, longer disease duration and higher CD activity index scores were associated with lower placebo clinical remission rates
Increased duration of follow-up, more follow-up visits and a greater proportion of patients with colonic disease distribution were associated with higher clinical placebo rates
My take: These studies show fairly high placebo responses and thus they reinforce the need for well-designed trials with objective endpoints.
Recent articles indicate the possibility of preclinical disease detection of inflammatory bowel disease; perhaps this is analagous to the “precrime’ detection in The Minority Report which allowed the police to arrest people before they committed their crime.
In this study from Sweden, the authors used biobanked plasma samples from 72 individuals with ulcerative colitis (UC) and matched healthy controls (n=140). Then the findings were validated in an inception cohort (n=101 with UC and 50 healthy controls. In addition, a cohort of heathy twin siblings of patients with UC (n=41) were matched with healthy controls (n=37).
Key findings:
Six proteins (MMP10, CXCL9, CCL11, SLAMF1, CXCL11 and MCP-1) were up-regulated (P < .05) in preclinical ulcerative colitis compared with controls
MMP10, CXCL9, CXCL11, and MCP1, but not CCL11 and SLAMF1, were significantly up-regulated among the healthy twin siblings. This up-regulation is triggered by exposure to genetic and early environmental factors.
The discussion elaborates on the role of these proteins.
“MMP10 is classified as a stromelysin. Upregulated levels of stromelysin have been detected in inflamed segments of the colon from patients with ulcerative colitis….The observed preclinical upregulation of MMP10 [thought to promote wound healing] in plasma might indicate that endogenous pathways for wound healing are up-regulated several years before clinically overt ulcerative colitis to counteract disease progression and maintain mucosal homeostasis”
“Eotaxin (CCL11) is a potent chemoattractant of monocytes…eosinophilic-driven inflammation represents an early element in the pathogenesis of ulcerative colitis”
“CXCL9 and CXCL11 has been observed previously in inflamed colonic tissue specimens and blood from patients with ulcerative colitis… Both chemokines are regulated by IFN-gamma and attract CXCR3-positive CD4þ T cells and natural killer cells to the inflammatory site”
My take: This study shows up-regulation of 6 plasma proteins indicating activation of both pro-inflammatory and tissue-repairing pathways several years before clinically overt UC. It offers hope of intervention to prevent the development of UC.
In this study, the authors measured host serum antibody response to 6 microbial antigens at enrollment (Prometheus enzyme-linked immunosorbent assay test: anti-Saccharomyces cerevisiae antibodies immunoglobulin A/immunoglobulin G, anti-OmpC, anti-A4-Fla2, anti-FlaX, anti-CBir1) and derived the sum of positive antibodies (AS).
Key finding:
“High baseline AS (≥2) (43% of cases, 11% of controls) was associated with higher risk of developing CD (adjusted odds ratio, 6.5; 95% confidence interval, 3.4–12.7; P < .001). Importantly, this association remained significant when adjusted for markers of gut barrier function, fecal calprotectin, C-reactive protein, and CD-polygenic risk score, and in subjects recruited more than 3 years before diagnosis. Causal mediation analysis showed that the effect of high AS on future CD development is partially mediated (42%) via preclinical gut inflammation.
The main reason I had to highlight this article is the study period was 42 years!!! (1977-2019, n=236 children). Key findings: “Unique HLA profiles are seen in each subgroup of juvenile AILD: DRB1*03 for AIH-1, DRB1*03 plus DRB1*07 for AIH-2, and DRB1*13 for ASC. DRB1*03 and the A1-B8-DR3 haplotype are disease-predisposing genes for all three subgroups. The influence of HLA class II genes on disease severity is strong, DRB1*03 homozygosity and possession of DRB1*13 being associated to histologically more advanced disease from onset, while DRB1*07 is linked to the least optimal response to immunosuppression”
The “EVIDENCES IV study was a multicenter, randomized, double-blind, placebo-controlled phase 2 study to evaluate the safety and efficacy of saroglitazar.” n=106. Key findings:
For ALT: mean percent change from baseline at week 16 was −25.5% (5.8), −27.7% (5.9), and −45.8% (5.7), with saroglitazar 1 mg, 2 mg, and 4 mg, respectively, versus 3.4% (5.6) in placebo (P < 0.001 for all)
Compared with placebo, saroglitazar 4 mg improved liver fat content on MRI PDFF (4.1% [5.9] vs. −19.7% [5.6]), adiponectin (−0.3 μg/mL [0.3] vs. 1.3 μg/mL [0.3]), homeostatic model assessment–insulin resistance (−1.3 [1.8] vs. −6.3 [1.7]), and triglycerides (−5.3 mg/dL [10.7] vs. −68.7 mg/dL [10.3]) (P < 0.05 for all)
Saroglitazar was well-tolerated. A mean weight gain of 1.5 kg was observed with saroglitazar 4 mg versus 0.3 kg with placebo (P = 0.27)
My take: This study shows the potential of one agent for pharmacologic therapy for NAFLD/MAFLD.
“A majority of LT recipients (75%) identified themselves as survivors. Integral to the definition of survivorship was overcoming hardship (including experiences on the waiting list) and the unique experience of being given a “second chance” at life. Motivations to survive included a new chance at life (55%), family (40%), spirituality/faith (30%), and fear of rejection (15%)”
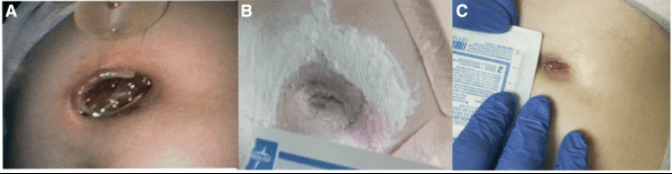
This case report describes a 10 yo with multiple medical problems with an expanding G-tube site with mucosal prolapse “where the G-tube balloon easily fell out of her gastrocutaneous fistula.”
The site was treated with three modalities, though the authors attribute the improvement to the use of sucralfate:
Nasojejunal feedings
Removal of Gastrostomy tube for 5 days
Sucralfate: “1 gram tablet, ½ tablet crushed sprinkled around the ostomy site 3 times a day. Powder was used to fill in the defect and any residual powder medication was gently cleaned off before the next application”
Images showing improvement noted below
The authors provide pathophysiological reasons for sucralfate’s effectiveness:
Treatment with sucralfate helped reduce the 2 cm x 1.5 cm site (Panel A) over 5 days to Panel B and over 4 weeks to Panel C
Background: “The general unavailability of culture-based susceptibility testing for H pylori has resulted in the almost universal reliance on hopeful (empiric) therapy and a high proportion of treatment failures.” Besides the lack of availability of culture-based susceptibility testing, the global increase in prevalence of antimicrobial resistance contributes to the poor cure rates obtained with empiric use of the currently most popular triple therapies for H pylori infection.
Methods:H pylori isolates (n=170) (clinical isolates and formalin-fixed, paraffin-embedded) were tested for susceptibility to amoxicillin, clarithromycin, metronidazole, levofloxacin, tetracycline, and rifabutin using agar dilution and NGS targeted to 23S rRNA, gyrA, 16S rRNA, pbp1, rpoB and rdxA. Agreement was quantified using κ statistics.
Key findings:
Agreement between agar dilution and NGS from culture isolates was very good for clarithromycin (κ = 0.90012), good for levofloxacin (κ = 0.78161) and fair for metronidazole (κ = 0.55880), and amoxicillin (κ = 0.21400)
Comparison of NGS from tissue blocks and agar dilution from isolates from the same stomachs demonstrated good accuracy to predict resistance for clarithromycin (94.1%), amoxicillin (95.9%), metronidazole (77%), levofloxacin (87.7%), and tetracycline (98.2%)
“By targeting all of the genes responsible for antibiotic resistance, it is possible to obtain genotypic susceptibility data for all of the antibiotics of potential use, without the need to perform” culture and antibiotic susceptibility testing
“Hulten et al show not only that they obtained comparable results with the reference method (phenotypic) for most of the antibiotics, but also that NGS can also be performed on both culture isolates and stored histologic preparations. This result is important because it avoids the need for extra biopsies and culture”
“NGS could also be applied on stools. In this particular environment where H pylori DNA is found in a low amount, excellent DNA extraction methods are mandatory and progress is being made in this field”
My take: NGS can bring H pylori treatment to a new era (like almost all other infections). “Molecular methods can potentially augment or even replace the current in vitro methods for susceptibility testing, which are cumbersome, technically challenging, and time-consuming.”
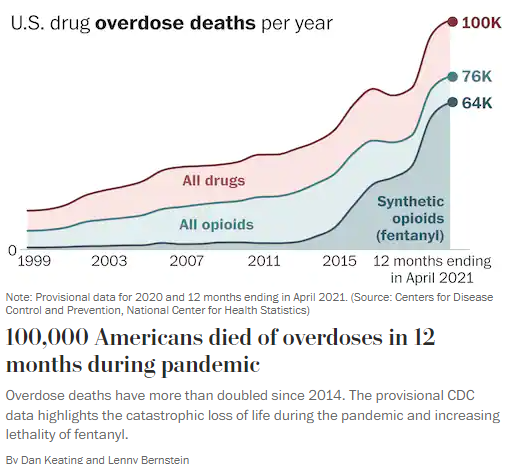
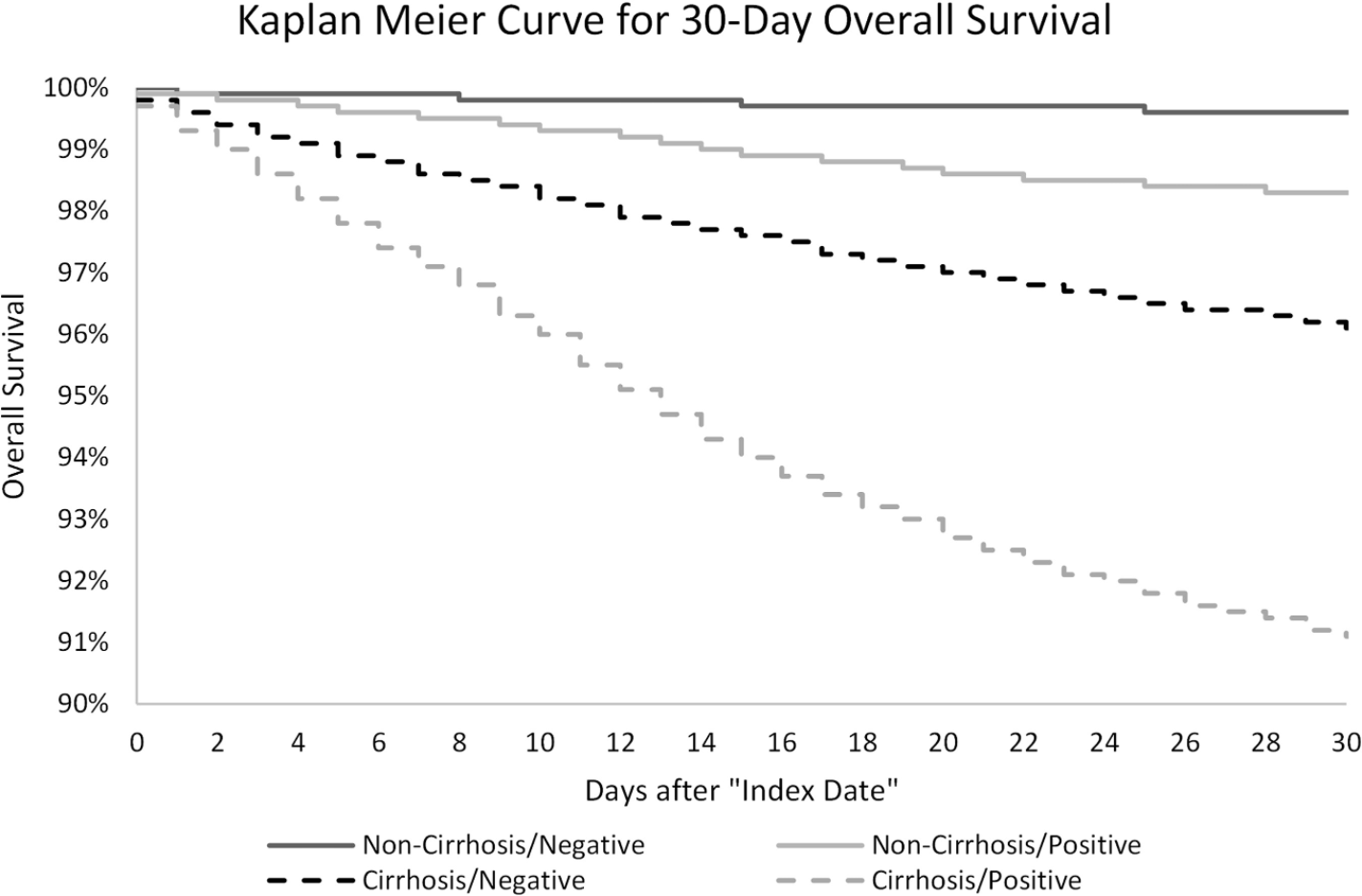
Key finding: “In this study of approximately 221,000 nationally representative, diverse, and sex-balanced patients with CLD; we found SARS-CoV-2 infection in patients with cirrhosis was associated with 2.38 times mortality hazard, and the presence of cirrhosis among patients with CLD infected with SARS-CoV-2 was associated with 3.31 times mortality hazard”
A recent article on simplifying the “simple” endoscopic assessment for Crohn’s disease reminded me of a scene from “There’s Something About Mary” (see below) where one of the characters plans to market a 7 minute abs video to replace the 8 minute abs video craze.
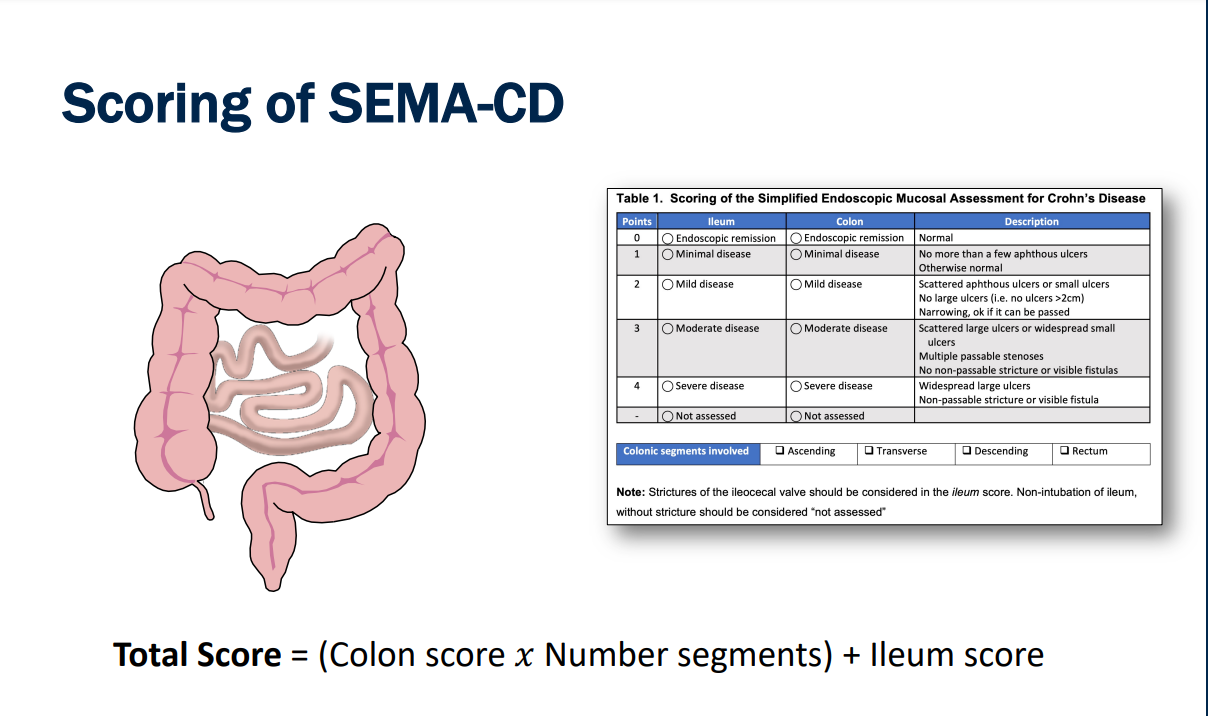
The article describes replacing the current “SES-CD” (or Simple Endoscopic Score for Crohn’s disease) with SEMA-CD (or Simplified Endoscopic Mucosal Assessment for Crohn’s disease).
The SEMA-CD was scored by assigning a numerical value ranging from 0 (remission) to 4 (severe disease) for each bowel region (ileum and colon). The colon score was multiplied by the number of involved colonic segments and then added to the ileum score. “For example, if overall the colon was felt to have moderate involvement, and only the ascending and transverse colon had mucosal abnormalities, then a score of 3 for moderate disease would be multiplied by a total of 2 segments for a total [colon] score of 6.”
Key finding:
While there was excellent correlation between SES-CD and SEMA-CD, SEMA-CD was much easier as it required one scoring for the entire colon rather than evaluation of each segment
The authors note that clinical assessment is inadequate to monitor CD. CDAI (PCDAI) are poor surrogates for mucosal improvement…”30-68% of patients in clinical remission have evidence of mucosal inflammation on colonoscopy….Patients whose disease is managed based on clinical information alone are more likely to have disease complications, need more surgeries, or lose response to medications.”
My take: The SEMA-CD appears to be much easier than the SES-CD and thus more likely to be useful in clinical practice (& research), especially as it becomes incorporated into routine endoscopy software. If the SEMA-CD is widely adopted, we will need to be on the lookout for the ‘6 minute ab’ version.