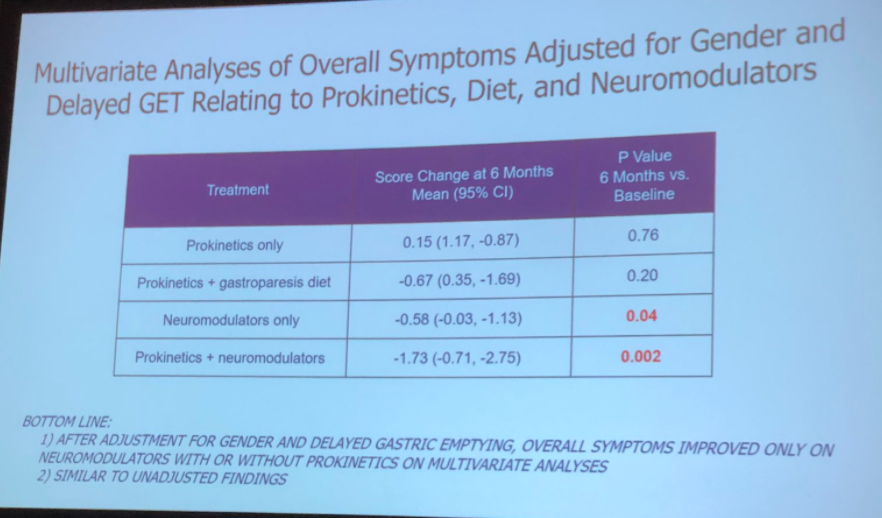
Prokinetics were not effective as monotherapy for gastroparesis. Neuromodulators were effective with and without a prokinetic:
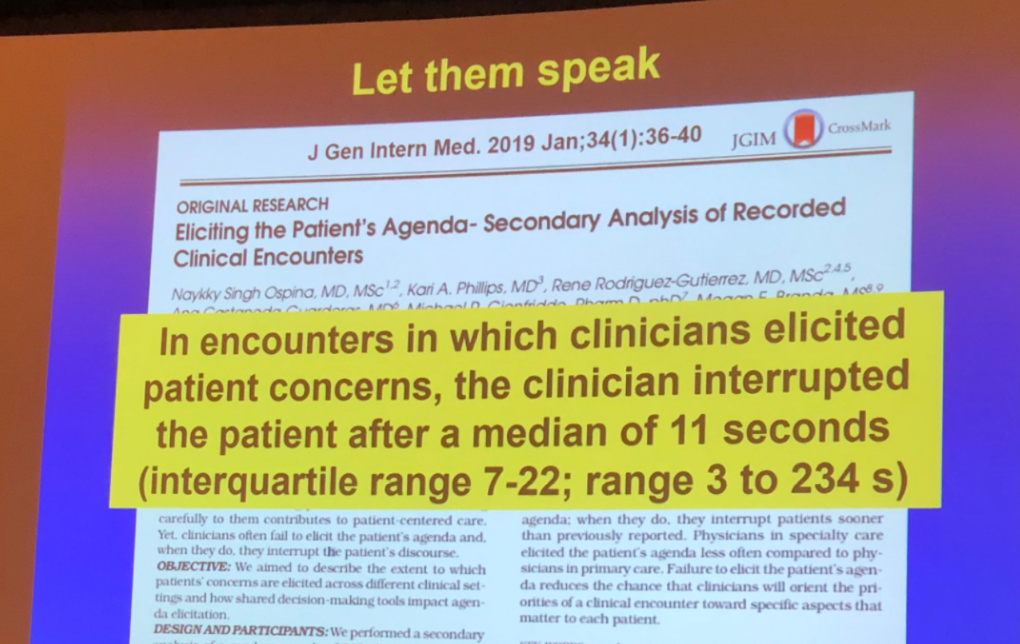
The most remarkable medical invention: The chair
Magnets recalled:

Prokinetics were not effective as monotherapy for gastroparesis. Neuromodulators were effective with and without a prokinetic:
The most remarkable medical invention: The chair
Magnets recalled:
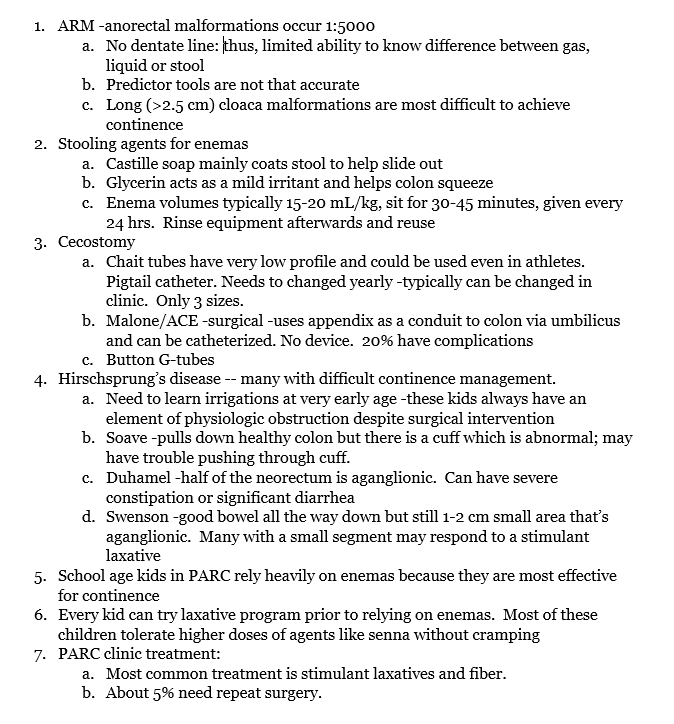
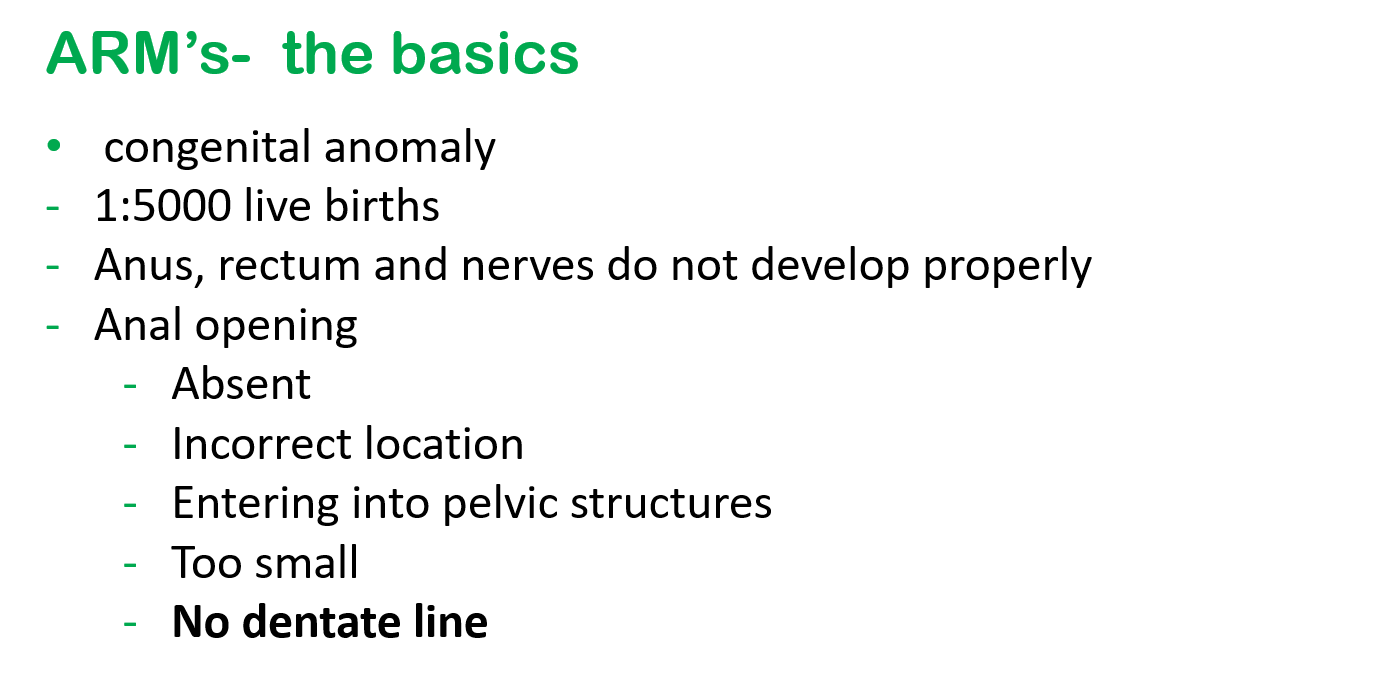
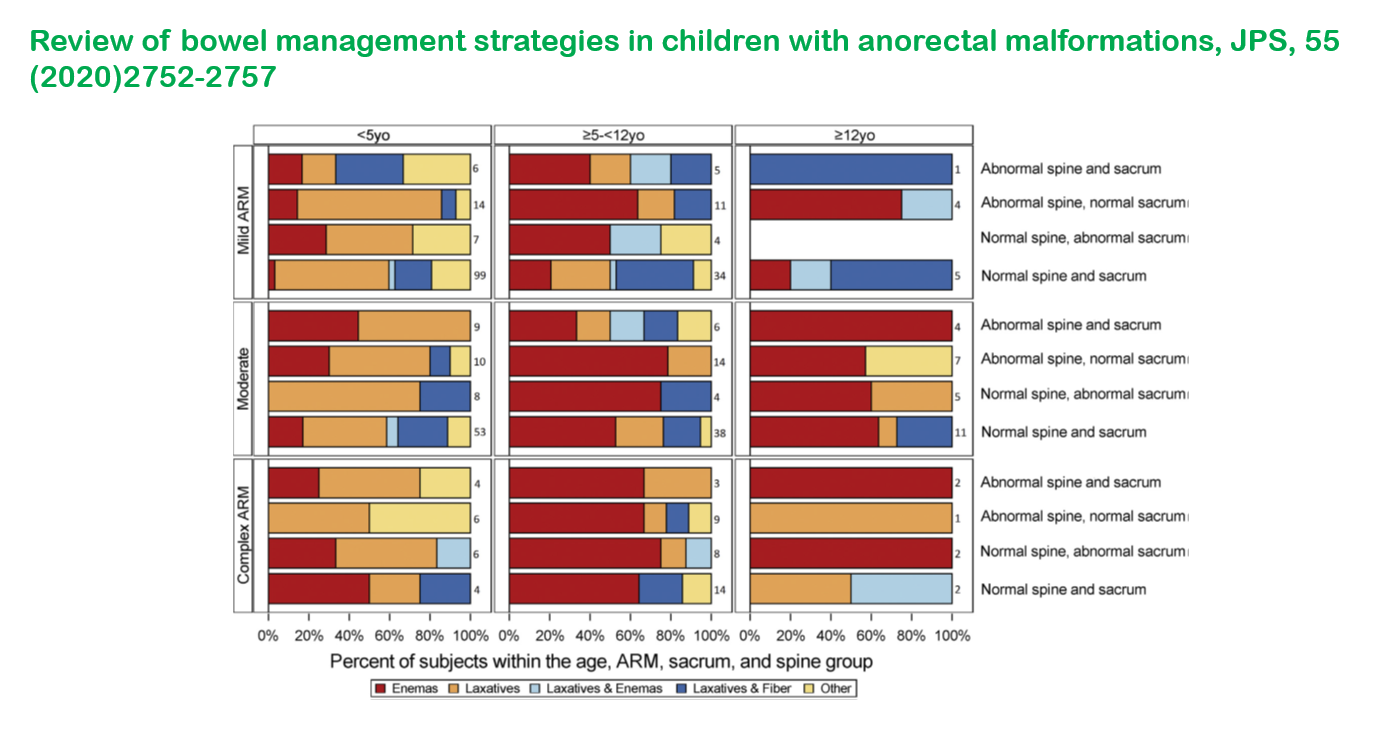
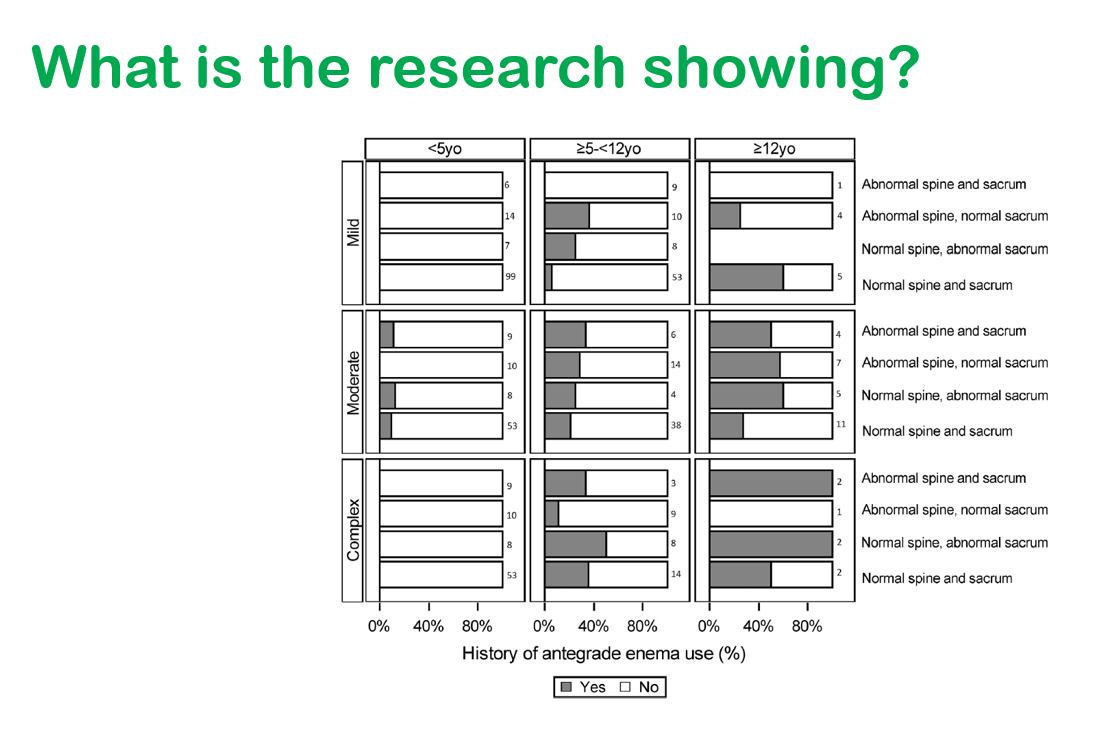
I recently had the opportunity to hear a terrific lecture by Kathleen Hoff regarding efforts to achieve continence for children, especially those with anorectal malformations. This blog entry has abbreviated/summarized the presentation. Though not intentional, some important material is likely to have been omitted; in addition, transcription errors are possible as well.
Key points (my notes followed by screenshots of some of the slides):
How to reach PARC team:





Related blog posts:
A recent clinical problem-solving case (TW Fredrick et al. NEJM 2021; 385; 549-554. Turning Purple with Pain) is a good review on episodic pain and acute intermittent porphyria (AIP).
The case presentation regarded a 32 yo with episodic severe pain for 10 years (associated with constipation) that required morphine. Episodes occurred every month or two and lasted for several days. Some clues in this case included the development of hyponatremia, purple urine, and an episode in which she was “out of it.” This episode was attributed to opioid use and providers were concerned about opioid-seeking behavior and a conversion disorder.
She had extensive evaluations including imaging, panendoscopy, and labs. Atypical labs included serum tryptase, cortisol, and C1 esterase inhibitor level. Ultimately, her constellation of findings led to a urine porphyrin levels which disclosed elevated porphobilinogen (PBG) and delta-aminolevulinic acid. The diagnosis of AIP was confirmed with genetic testing.
Key points:
My take: This article provides a useful overview. AIP needs to be considered in adolescents with severe abdominal pain that results in hospitalization (especially if episodic).
Related blog post: Liver Shorts -June 2020 (with AIP article)
Also, data supporting COVID-19 effectiveness in reducing the risk of hospitalization–CDC study shows unvaccinated people are 29 times more likely to be hospitalized with Covid (CNBC)


S Phillips, MA Wiliams. NEJM 2021; 385: 577-579. Open Access: Confronting Our Next National Health Disaster — Long-Haul Covid
A few excerpts:
My take: It is unfortunate that many cases of long-haul Covid that will develop could be prevented with vaccination


Job Openings: Pediatric Gastroenterologists
Description
GI Care For Kids is seeking multiple experienced Pediatric Gastroenterologists to join our group of 15 pediatric gastroenterologists and 5 advanced practice providers. Our highly-regarded and busy private practice provides state-of-the art, comprehensive care in our offices and at Children’s Healthcare of Atlanta at Scottish Rite, located across the street from our main office.
Our group includes general pediatric gastroenterologists as well as physicians with a wide range of subspecialization, including inflammatory bowel disease, short bowel syndrome, eosinophilic diseases, motility disorders, feeding disorders, aerodigestive disorders, and celiac disease. Many of our physicians are recognized nationally for their achievements. With our clinical colleagues at Children’s Healthcare of Atlanta, we are rated as the #8 pediatric gastroenterology program in the country by U.S. News.
Important features of our practice include the following:
We are looking for candidates with prior clinical experience (prefer 2 or more years after fellowship) and excellent communication skills. Additional expertise in advanced endoscopy or pancreatic specialization would be ideal but not a requirement for consideration. All candidates should be board-certified in pediatric gastroenterology.
The Atlanta area is a thriving city (except during a snowstorm) with excellent schools and recreational opportunities. Our office offers competitive salary, benefits, vacation time (20 work days including CME time), and partnership opportunity. Compensation package includes family health insurance, profit sharing, and CME allowance. Hospital coverage averages 1 week/1 weekend per month. Night call is shared and averages about 2 nights per month. Our group is committed to fostering a diverse, equitable, inclusive, and family-friendly environment in which all physicians and staff can excel and achieve work/life balance.
Please send letter of interest and curriculum vitae to: Katrin Herzog. Email address: kherzog@gicareforkids.com
G D’Arcangelo et al. JPGN 2021; 73: 242-246. Is Fecal Calprotectin a Useful Marker for Small Bowel Crohn Disease?
In this retrospective study with 98 patients, the authors examined the sensitivity and specificity of fecal calprotectin (FC) at a cutoff of 150 mcg/g in comparison to findings of ileocolonoscopy and MRE in those with isolated ileal CD (L1, n=14), colonic CD (L2, n=10) and ilecolonic CD (L3, n=74) . Note: the abstract erroneously states the cutoff as 50 mcg/g.
Key findings:
My take: Though this study had only 14 patients with isolated ileal disease, it is likely that a calprotectin level is less reliable as a biomarker in these patients.
Related article: Jukic A, Bakiri L, Wagner EF, et al Calprotectin: from biomarker to biological functionGut Published Online First: 18 June 2021. doi: 10.1136/gutjnl-2021-324855. Thanks to KT Park for this reference. Open Access- Full text: Calprotectin: from biomarker to biological function
Related blog posts:

T Niseteo et al Nutr Clin Pract 2021: 1-7. Modified Crohn’s disease exclusion diet is equally effective as exclusive enteral nutrition: Real-world data Thanks to Kipp Ellsworth for this reference.
This was a retrospective study with 61 children, median age, 14.4 years; overall, 42 (69%) achieved clinical remission based on weighted PCDAI. The study compared a modified Crohn’s disease exclusion diet (CDED) (modified as 80% in this group had 1–2 weeks of EEN initially) to EEN; PEN accounted for ~50% of calories CDED/PEN group received mainly modulen whereas EEN received a number of standard polymeric isocaloric formulas (eg. pediasure, osmolite, ensure plus). Concomitant medical therapy was used in ~80% of patients (most often azathioprine).
Key finding: Clinical remission was similar in both groups: 27 of 41 (65.9%) received EEN and 15 of 20 (75.0%) received CDED + PEN after 6-8 weeks of treatment. In addition, both groups had improvement in CRP and Hemoglobin.
*Several authors grants/payments from formula manufacturers.
My take: This study while favorable towards a combination of CDED/PEN is limited by small numbers, retrospective design, limited followup and absence of data on mucosal healing.
Related blog posts:
K Lambert et al. AP&T 2021; https://doi.org/10.1111/apt.16549. Systematic review with meta-analysis: dietary intake in adults with inflammatory bowel disease. Thanks to Ben Gold for this reference.
This meta-analysis included 19 studies of adults with IBD involving dietary intake. Results “show inadequate energy for all subgroups of adults with IBD (mean intake in adults with IBD 1980 ± 130 kcal), as well as fiber (14 ± 4 g), folate (246 ± 33 mg) and calcium (529 ± 114 mg) per day.” Further, “In comparison to the healthy control groups, IBD patients consumed significantly less dietary fiber (SMD −0.59; 95% CI, −0.73 to −0.46).”

Gastro & Endo News July 2021, Full Text: Disease Surveillance With Every Flush: Introducing the Smart Toilet
Key finding:
An excerpt:
“At the 2021 virtual Digestive Disease Week, Duke University gastroenterologist Deborah Fisher, MD, and engineering professor Sonia Grego, PhD, showed that toilets enabled with artificial intelligence can analyze stool samples for signs of acute or chronic gastrointestinal disease, such as bleeding, infections or even inflammatory bowel disease.”
My take: I definitely do NOT want my toilet to be too smart. It would not be hard to imagine the toilet berating me for what I ate for dinner the night before.

A lot of research is looking at how alterations in the microbiome affect a plethora of medical outcomes. Recently, there was a study linking sugar consumption in adolescence with an increased risk of adenomas (full text link: Simple Sugar and Sugar-Sweetened Beverage Intake During Adolescence and Risk of Colorectal Cancer Precursors; Gastroenterol 2021; 161: 128-142).
Now, a study indicates that taking oral antibiotics can influence the risk of developing antibodies to infliximab.
Full text (open access): Antibiotic use differentially affects the risk of anti-drug antibody formation during anti-TNFα therapy in inflammatory bowel disease patients: a report from the epi-IIRN (thanks to John Pohl for this reference)
Citation: Gorelik Y, Freilich S, Gerassy-Vainberg S, et al Antibiotic use differentially affects the risk of anti-drug antibody formation during anti-TNFα therapy in inflammatory bowel disease patients: a report from the epi-IIRNGut Published Online First: 03 August 2021. doi: 10.1136/gutjnl-2021-325185
This study reviewed data from 1946 patients with 363 who developed anti-drug antibodies (ADA). Then, specific pathogen and germ-free C57BL mice were treated with respective antibiotics and challenged with infliximab. ADA were assessed after 14 days.
Key findings:
My take: The combination of retrospective data and mouse studies suggests that taking some antibiotics (mainly penicillins and cephalosporins) could increase the risk of immunogenicity to infliximab and increase the risk of anti-drug antibodies.

SJ Moltu et al JPGN 2021; 73: 274-289. Full Text: Nutritional Management of the Critically Ill Neonate: A Position Paper of the ESPGHAN Committee on Nutrition
Background: The authors of this position paper are trying to modulate the treatment recommendations based on the PEPaNIC trial. This “large randomized trial, the Early versus Late Parenteral Nutrition in the Pediatric Intensive Care Unit (PEPaNIC) trial, showed that withholding parenteral nutrition (PN) during the first week of acute illness improved early outcomes as compared to PN initiated during the first 24 hours after admission in children [Fivez T, Kerklaan D, Mesotten D, et al. Early versus late parenteral nutrition in critically ill children. N Engl J Med 2016; 374:1111–1122] (71). Effects were similar in the subgroup of 209 term-born neonates recruited to the trial (72). Despite this finding, many clinicians appear reluctant to limit early nutritional support due to (1) concerns about possible harm by not providing adequate nutrients during the first week of critical illness, particularly in neonates and undernourished children (73), and (2) the belief that exogenous dietary protein provision is essential during critical illness (73).”
Key recommendations:
My take: Particularly in preterm infants, adequate nutrition should not be withheld due to their very limited reserves. In term critical infants, these guidelines offer a logical approach until more studies are available.
Related blog posts:

