Background: “The prevalence of obesity among patients with inflammatory bowel disease (IBD) is estimated at 15-40%, and continues to rise. Obesity has been associated with a more severe phenotype of IBD.”
Methods: Retrospective cohort with 244 patients. Semaglutide was the most commonly prescribed agent (54%).
Key findings:
GLP-1RA use led to weight loss from 102 kg to 97.6 kg at 12-24 weeks postinitiation
GLP-1RA was associated with a significant drop in CRP from 10.1 mg/dL to 3 mg/dL
In a subset of 32, fecal calprotectin values decreased from 825 mcg/kg to 235 mcg/kg (P= 0.13)
Limitations: Retrospective study with a short duration, lack of a control group for this study, and lack of endoscopic data.
My take: As with the broader population, GLP-1 RAs help with weight loss in patients with IBD. Many patients may derive health benefits from weight loss alone. This study, though with numerous limitations, indicates the potential beneficial effects on the activity of IBD based on improvements in biomarkers.
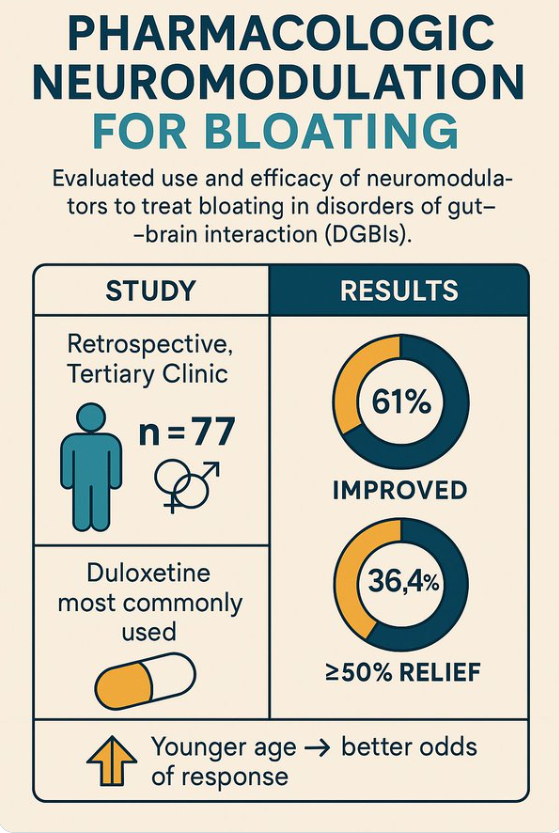
This was a small retrospective study of consecutively referred patients with a DGBI (N = 77; ages 18-74, 87% female) to a tertiary neurogastroenterology clinic who were prescribed a neuromodulator for a primary complaint of bloating in 2016-2022. Duloxetine was the most commonly prescribed neuromodulator (n = 52, 67.5%).
My take: This study shows that neuromodulators are likely beneficial for bloating symptoms. Dr. Garza () previously noted that in patients with bloating “the typical increase in excess gas during bloating symptoms is only 22 mL.” Thus, “A lot of bloating symptoms are due to increased sensitivity and ‘weird gas handling.’ The latter could include compression of diaphragm rather than elevation.”
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
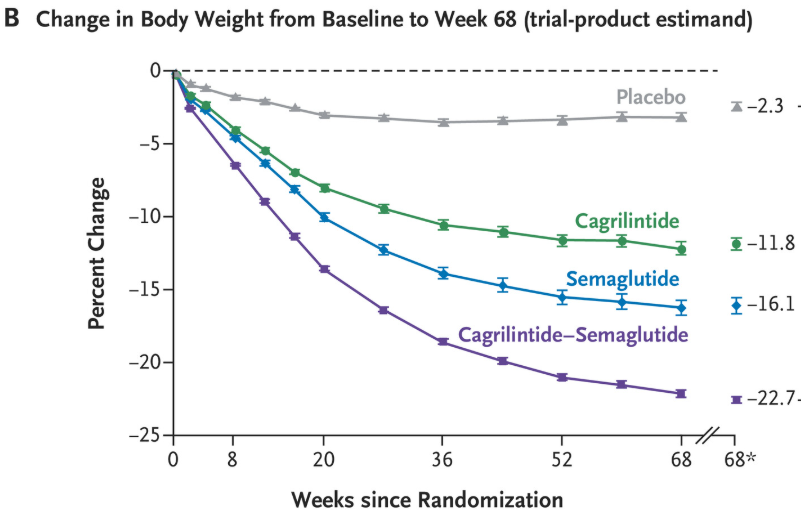
WTGarvey et al. N Engl J Med 2025;393:635-647. Coadministered Cagrilintide and Semaglutide in Adults with Overweight or Obesity
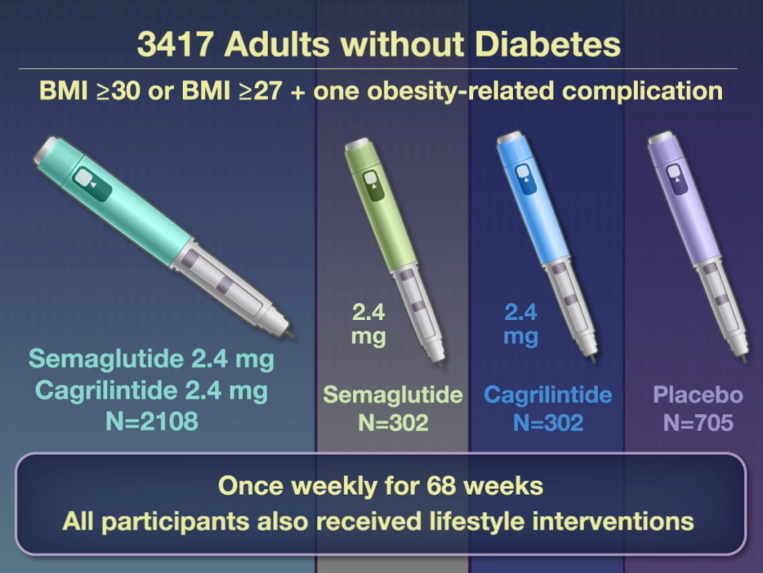
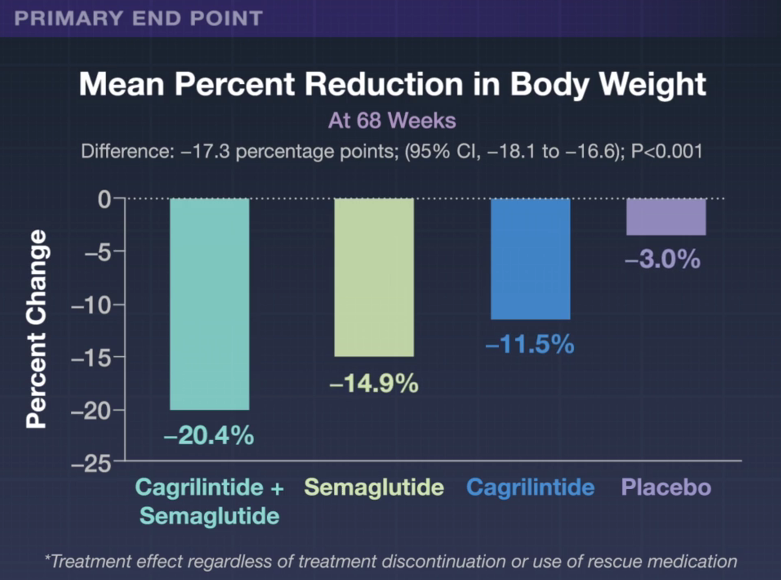
This phase 3a, 68-week, multicenter, double-blind, placebo-controlled and active-controlled trial (REDEFINE 1) examined the efficacy of the combination of Cagrilintide and Semaglutide (known as CagriSema). Patients had a body-mass index (BMI) of 30 or higher or a BMI of 27 or higher with at least one obesity-related complication. The combination druge was delivered as a fixed-dose in a single-dose, single-use pen device. 6.1% of trial participants had BMI <30.
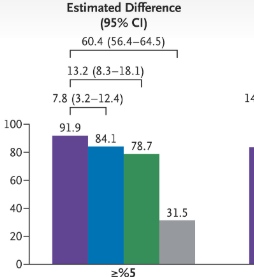
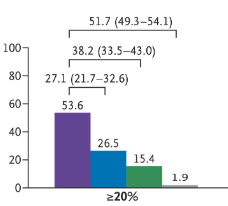
Percentage of patients with at least 5% weight loss Percentage of patients with at least 20% weight loss
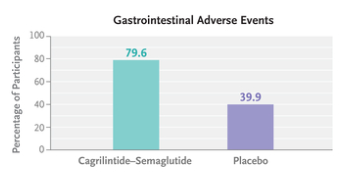
“Gastrointestinal adverse events (affecting 79.6% in the cagrilintide–semaglutide group and 39.9% in the placebo group), including nausea, vomiting, diarrhea, constipation, or abdominal pain, were mainly transient and mild-to-moderate in severity.”
“Although 57.4% of the participants assigned to cagrilintide–semaglutide were receiving the maximum dose at 68 weeks, 74.7% had received the maximum dose at some point after randomization…doses below the target might be highly effective for some patients and that dose reductions based on the clinical judgment…may be appropriate.”
This same issue also examined the use of this combination in patients with type 2 diabetes (REDEFINE 2). in this study with 1206 patients, “the estimated mean change in body weight from baseline to week 68 was −13.7% in the cagrilintide–semaglutide group and −3.4% in the placebo group.”
The editorial by CM Hales (“Expanding the Treat-to-Target Toolbox for Obesity and Diabetes Care”) notes that “six deaths occurred in the two trials combined, all in the cagrilintide–semaglutide groups, including one suicide in each trial. Previous studies of suicidality with GLP-1 receptor agonist treatment have not supported a causal link,6 but it continues to be of concern.”
My take (from the editorial): “A sustainable treat-to-target approach should extend to lifelong maintenance of health gains after initial weight loss. The intensity and composition of lifestyle interventions in the context of highly effective pharmacologic therapies also need further study. The pharmaceutical pipeline is promising, with potential improvements in safety (such as preservation of lean mass) and more convenience for patients (such as oral administration and monthly dosing). Greater effects on the health of Americans may be achieved not with antiobesity medications producing ever greater magnitudes of weight loss but with expanded access to safe and effective therapies for those who would most benefit.”
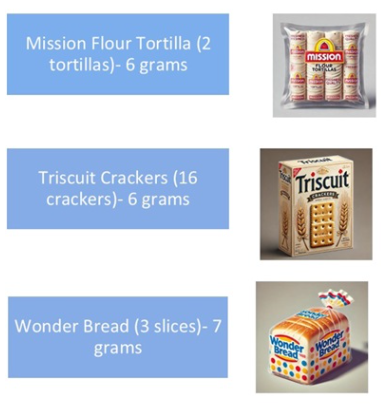
Figure 3 lists the content of several common foods -some noted below
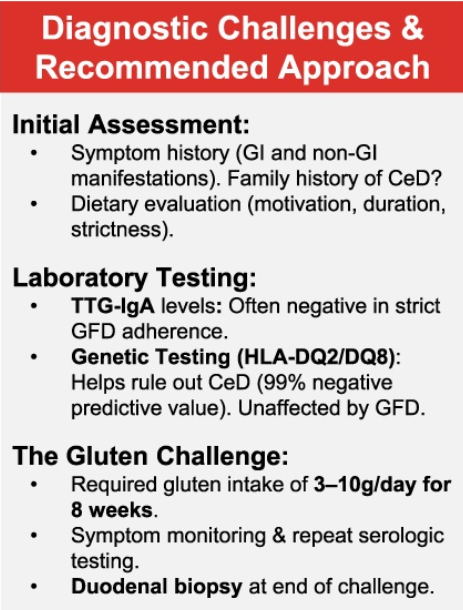
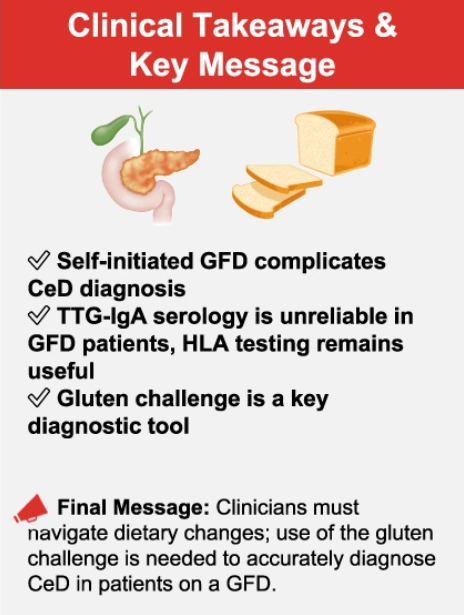
While gluten exposure increases the diagnostic yield of currently available tests, there are novel tests being developed “which may aid in the diagnosis of CeD regardless of diet, with a particular focus on immune-based assays. One such innovation involves the use of tetramer-based assays, which enable the direct detection of gluten-specific T cells in the blood. These tetramers, designed to bind to HLA-DQ2 molecules, can help identify T cells that have been activated by gluten exposure. This presents a highly specific immune marker for CeD. Even for those on a GFD, sensitivity (97%) and specificity (95%) have been impressive.”
My take: This article provides practical advice for evaluating whether celiac disease is present in those already consuming a GFD.
Briefly noted: The authors present a case report of an adolescent girl post cardiac transplant with hypergammaglobulinemia and presumed celiac disease (CD), who had a persistently elevated anti‐tissue transglutaminase immunoglobulin A despite a gluten free diet. Ultimately, she was diagnosed with polytypic plasmacytosis from suspected immune dysregulation.
Key point:
This case serves as a reminder that when treating those with persistently elevated tTG IgA on a strict GFD, etiologies outside of CD need to be considered.
My take: I had a young girl several years ago who had celiac diagnosis at an outside institution. She had multiple autoimmune disorders. After not responding to treatment, she had a follow-up panendoscopy showing ongoing IELs in duodenum and villous blunting. These findings were noted in the ileum as well. On reviewing her initial biopsies, the pathologist indicated that her findings could be celiac but it was suspected to be an immune dysregulation. Subsequently, she was diagnosed with CTLA4 deficiency and had a marked response to abatacept therapy.
Methods: The researchers conducted a 17‐item Qualtrics survey of patients who participated in intensive multidisciplinary intervention treatment to improve the volume and variety of solid food intake and replace enteral feeding due to chronic food refusal an average of 6 years following intervention. 75 met eligibility criteria; 36 caregivers (48%) completed the survey
Key findings:
Most patients (80%) who achieved full wean from feeding tube dependence at program discharge maintained their wean at the time of the survey
Most caregivers (89%) described their child’s relationship with food as “good” or “neutral”
My take:
Our group works closely with the authors and appreciate all of their help
Survey studies have a lot of limitations and often conclusions are hampered by low participation
It looks like intensive feeding therapy has good durability. It would be interesting if we could know what would have happened to these children without therapy. How many would have gradually improved on their own?
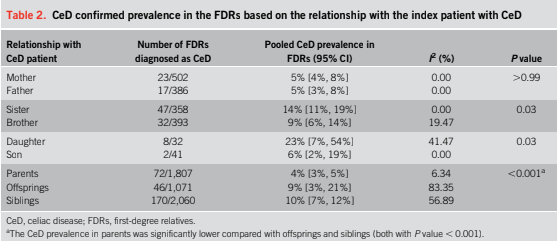
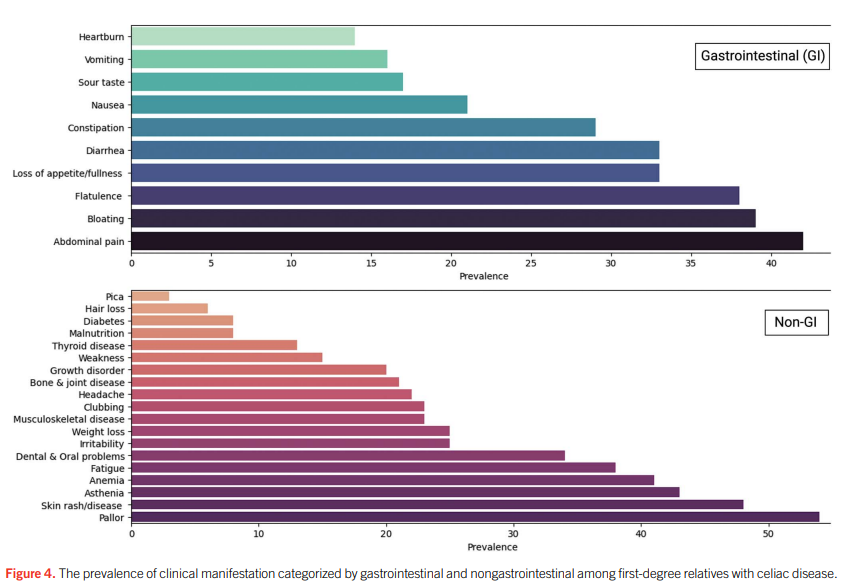
Methods: Of 8,764 studies screened, 34 studies involving 10,016 first-degree relatives (FDRs) of patients with Celiac Disease (CeD) were included
Key findings:
The pooled estimates for seroprevalence and the biopsy-confirmed CeD prevalence in FDRs were 11% and 7%, respectively
Daughters and sisters had the highest prevalence rates at 23% and 14%, compared with sons and brothers at 6% and 9%, respectively. Mothers/fathers prevalence rates were 5%. It is noted, however, that the stud only included 32 daughters and 41 sons, making these estimates less reliable
Abdominal pain (42%), bloating (39%), and flatulence (38%) were the most common gastrointestinal symptoms, while 34% of FDRs with CeD were asymptomatic
Discussion points:
Discrepancy between serology and biopsy: “First, not all individuals who tested positive through serological screening underwent a confirmatory duodenal biopsy. Second, some individuals with positive anti-tTG Ab may have false-positive results, or the disease process is still in the early stages of the disease, where intestinal damage is not yet detectable. This highlights that relying solely on serological screening without follow-up evaluations and intestinal biopsy can lead to overestimating the true prevalence of CeD.”
Limitations: “Some included studies only screened the siblings of indexed patients with CeD. For example, one study reported a prevalence of 22% among siblings. Given that genetic factors play a pivotal role in the pathogenesis of CeD and that the prevalence of CeD among siblings is often higher than that of other FDRs, this selective screening approach could potentially introduce selection bias into the overall prevalence of CeD in FDRs.”
My take: This study supports routine screening of first-degree relatives of patients with Celiac Disease, especially as many are asymptomatic.
Roughly 15 million people — six percent of adults in the United States — have metabolic dysfunction-associated steatohepatitis, known as MASH. Rates of the disease are rising…
Wegovy, which is a weekly injection, is now approved for adults with MASH and moderate-to-advanced levels of fibrosis, or excessive scar tissue in the liver. The drug is not intended for people with cirrhosis…
Wegovy will be a welcome addition to the options doctors can prescribe — as long as their patients can access them. The drug carries a list price of over $1,300 a month, although most people do not pay that full amount. Many people have lost insurance coverage for weight-loss drugs, as plans struggle to keep up with the costs.
Related review article:G Targher et al. NEJM 2025; 393: 683-698. Metabolic Dysfunction–Associated Steatotic Liver Disease. This review article succinctly covers the epidemiology, manifestations, disease progression and pivotal pharmacologic advances.
“A team of researchers found evidence of shady organizations churning out fake or low-quality studies on an industrial scale. And their output is rising fast, threatening the integrity of many fields…“If these trends are not stopped, science is going to be destroyed,” said Luís A. Nunes Amaral, a data scientist at Northwestern University and an author of the study”
““Science relies on trusting what others did, so you do not have to repeat everything,” Dr. Amaral said….By the 2010s, journal editors and watchdog organizations were warning that this trust was under threat. They flagged a growing number of papers with fabricated data and doctored images. In the years that followed, the factors driving this increase grew more intense.”
“As more graduate students were trained in labs, the competition for a limited number of research jobs sharpened. High-profile papers became essential for success, not just for landing a job, but also for getting promotions and grants. Academic publishers have responded to the demand by opening thousands of new scientific journals every year…”
“Organizations known as paper mills are now turning scientific fraud into a lucrative business. Scientists eager to pad out their resumes can pay hundreds to thousands of dollars to be named as an author of a paper that they had nothing to do with…paper mills often use artificial intelligence to alter the text they lift from other papers…”
“The papers that Dr. Amaral and his colleagues could study came to light only because of the work of independent sleuths. To estimate how many paper mill papers have yet to be exposed, Dr. Amaral’s team created a statistical model that accurately predicted the rate at which suspicious papers surfaced. They estimate that the number of paper mill products may be 100 times greater than the ones they have identified…”
“In their new study, they calculated that the number of suspicious new papers appearing each year was doubling every 1.5 years. That’s far faster than the increase of scientific papers overall, which is doubling every 15 years.”
““We need to stop making it profitable to game the system.”
My take: This problem has preceded the widespread use of AI, although Al makes it harder to detect. Unfortunately, fake scientific reporting appears to be worsening.
Related article: Jessica Steier NY Times 8/19/25: The Playbook Used to ‘Prove’ Vaccines Cause Autism This article details very specifically how David Geier (now appointed by RFK Jr to evaluate vaccines and autism) and his father have produced multiple flawed studies regarding vaccine safety. This commentary takes a particularly deep dive into one of his articles on the preservative thimerosol. She shows that the authors likely used p-hacking to identify “atypical autism” since there was not a significant association with autism, compared different time cohorts (the control group was from a period with different diagnostic criteria/lower rates of autism), did not include confounders, and supported their arguments with “personal citing.”
Some excerpts:
There have been some 70 studies since Mr. Wakefield’s looking for any link between vaccines and autism. Of these, 26 have linked vaccines to autism in some way, and 43 found no connection between vaccines and autism.
A whopping two-thirds of studies that claimed to have found a link were written by David and Mark Geier. These studies have been heavily criticized for using deceptive research techniques and flawed data.
Among the eight other studies that found a link, four were retracted for data manipulation, flawed methods or undisclosed conflicts of interest. Most of the authors have been involved in anti-vaccination campaigns and have had other papers retracted.
One such study that Mr. Kennedy referred to in his Senate confirmation hearing was published in a WordPress blog disguised as a journal and was funded by an anti-vaccine organization, among other problems.
Fortunately, independent scientists have conducted more than 40 high-quality studies since 1998 involving over 5.6 million people across seven countries. All found no connection between vaccines and autism. These studies were rigorously designed, were reviewed by independent peers and do not contain telltale signs of data manipulation, as the Geier studies do.
Recently Dr. Bezerra gave our group a terrific lecture. I have taken some notes and shared some of his slides. There may be inadvertent omissions and mistakes in my notes. In addition, Dr. Bezerra’s presentation included several lengthy animations which helped explain the basic science concepts. These are not included in this summary.
Prior to his presentation to our group, Dr. Bezerra’s accomplishments had been recognized with the Shwachman Award, the highest honor bestowed by our national pediatric GI organization NASPGHAN (NASPGHAN Awards 2025). On a personal note, Jorge was the first person to give me hands-on instruction with an endoscope and I have a great deal of admiration for his humility, thoughtfulness and scientific achievements.
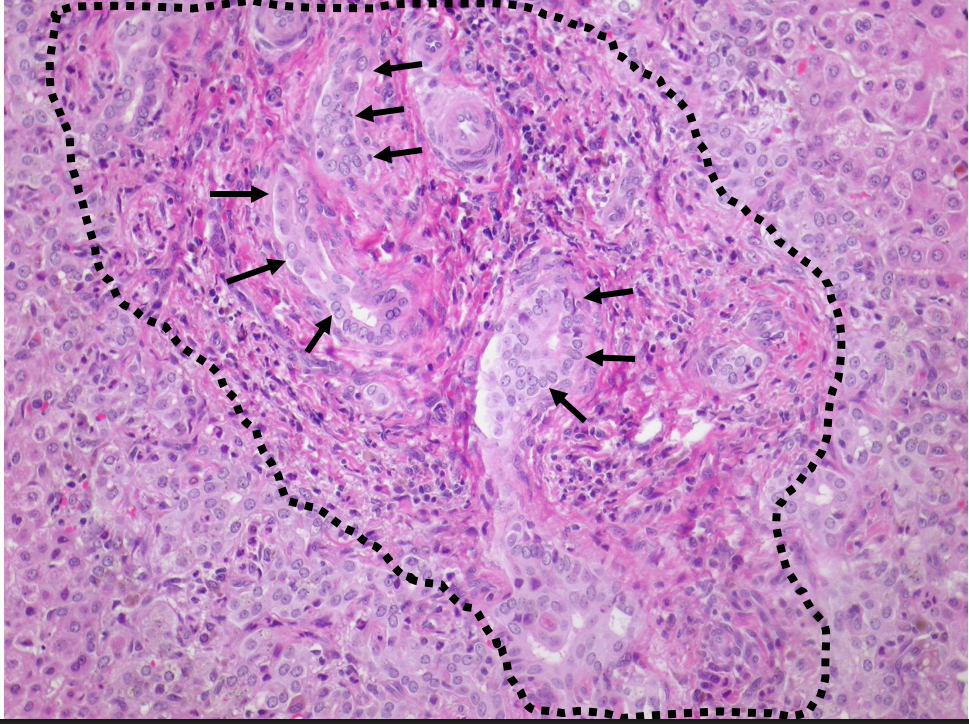
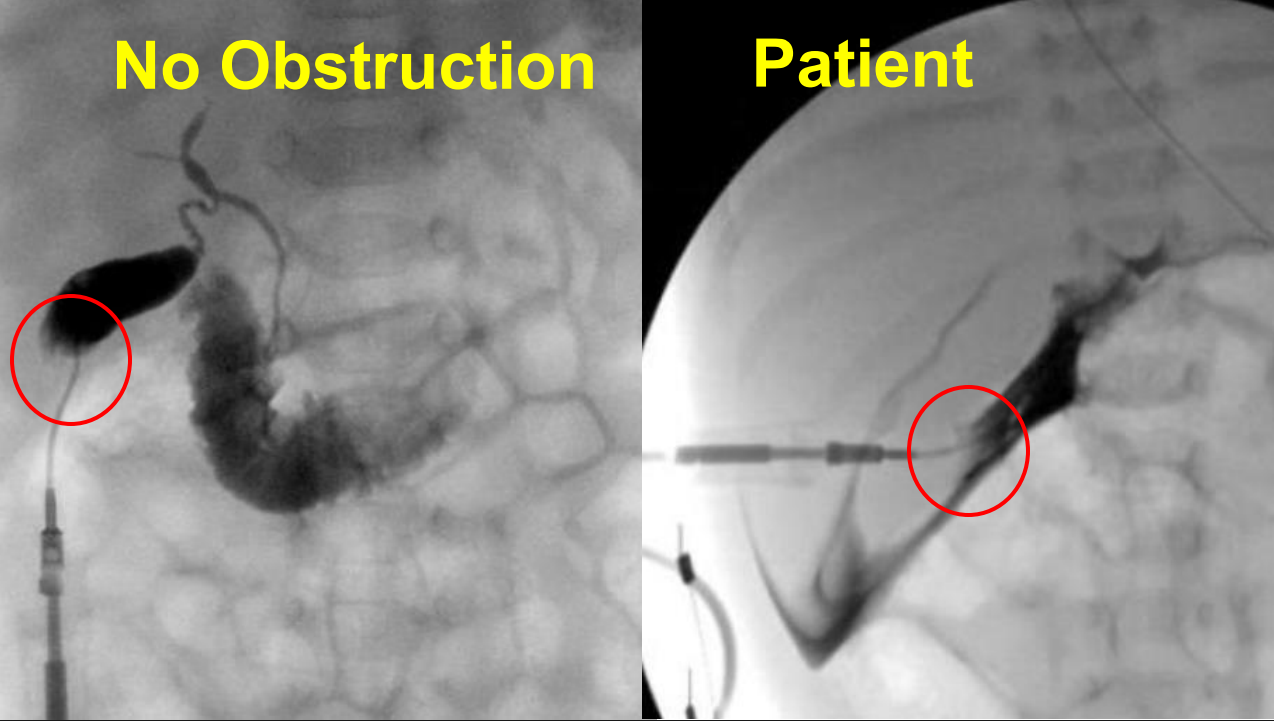
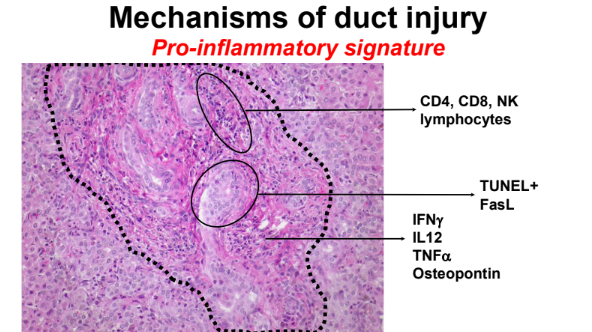
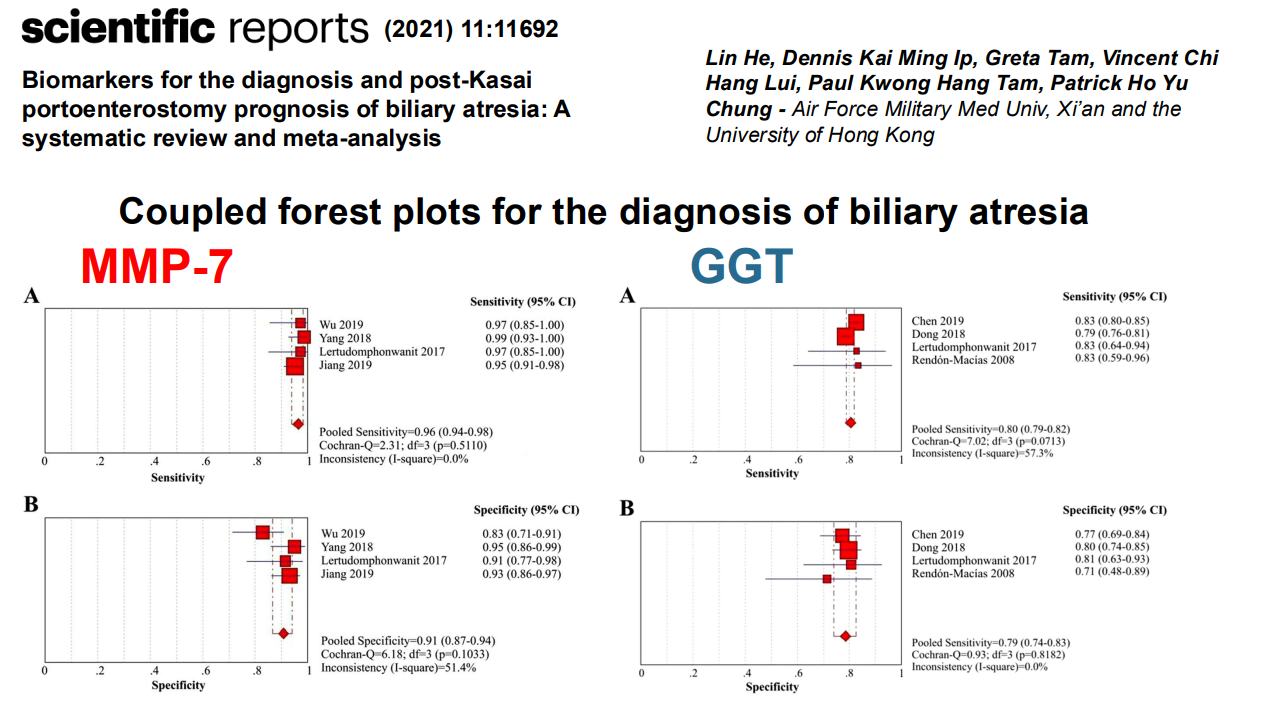
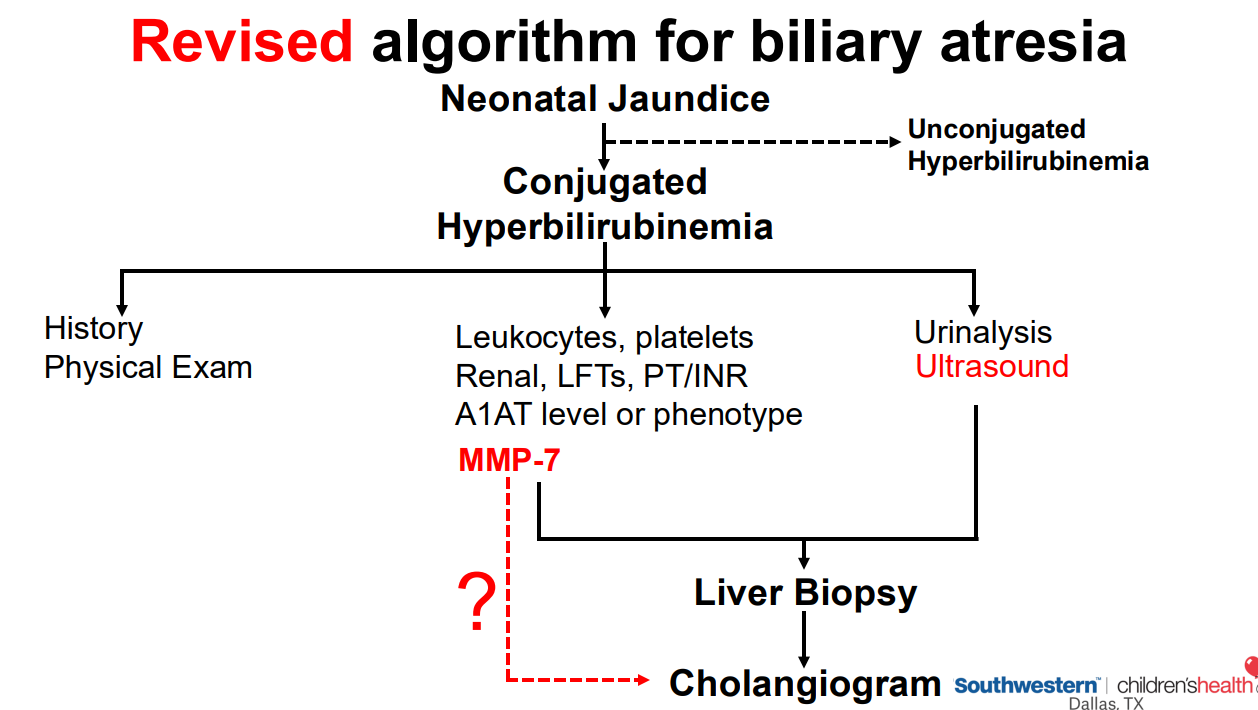
Liver biopsy from patient with BA showing bile duct proliferation .Operative cholangiograms from a patient with normal anatomy and one with BA that shows contrast extravasation without patent biliary tract
Key points:
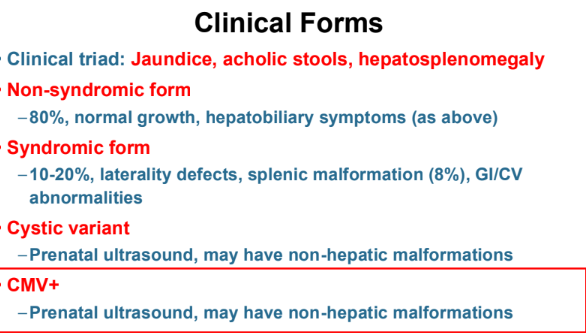
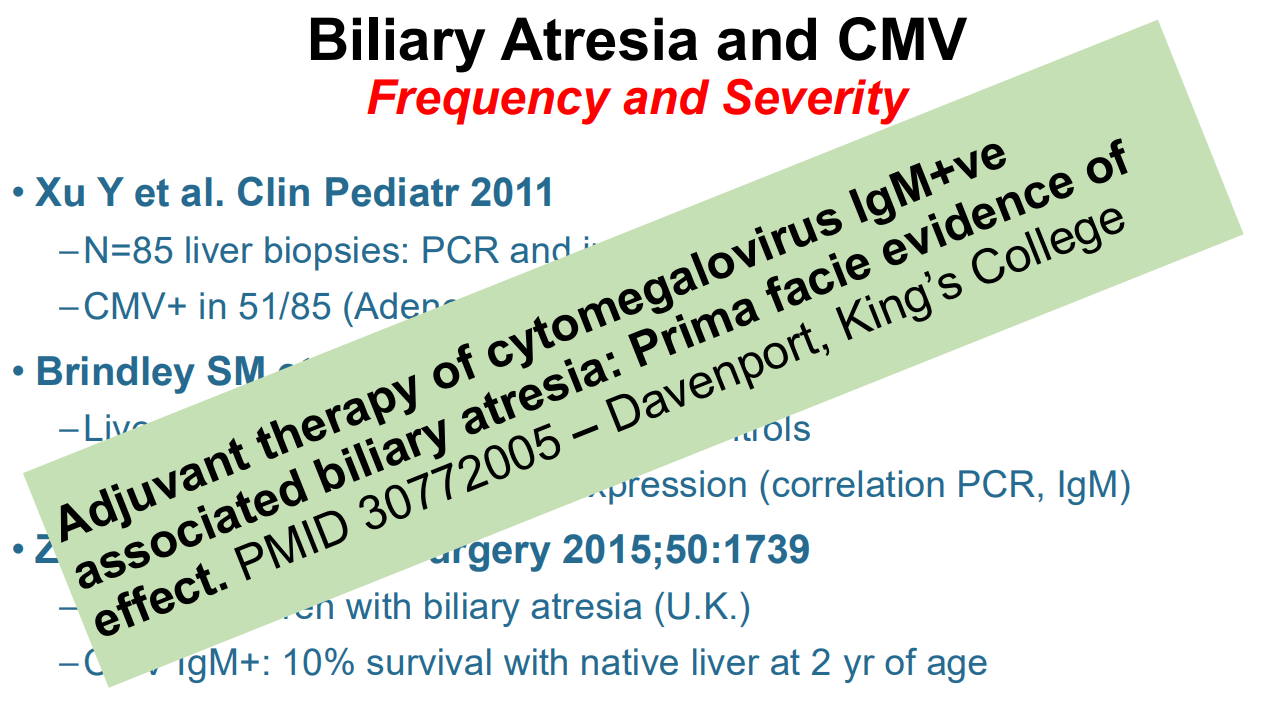
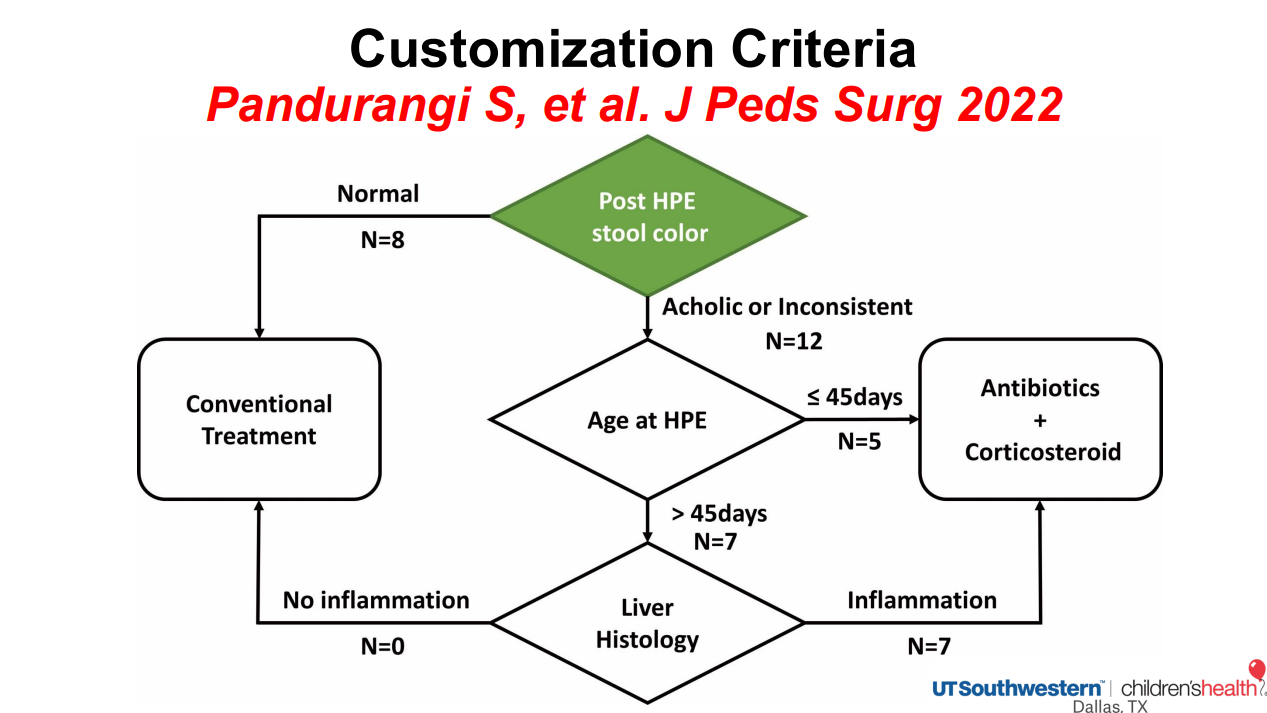
Cytomegalovirus (CMV) is frequently associated with biliary atresia (BA). Treatment of CMV when detected may improve outcomes
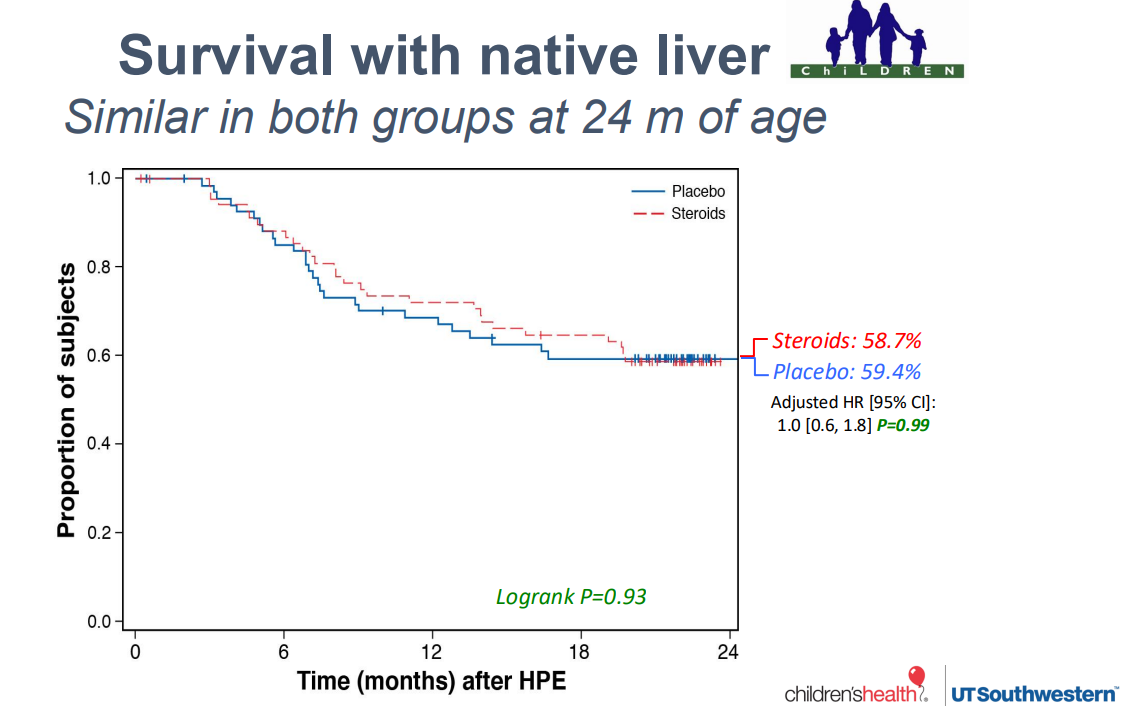
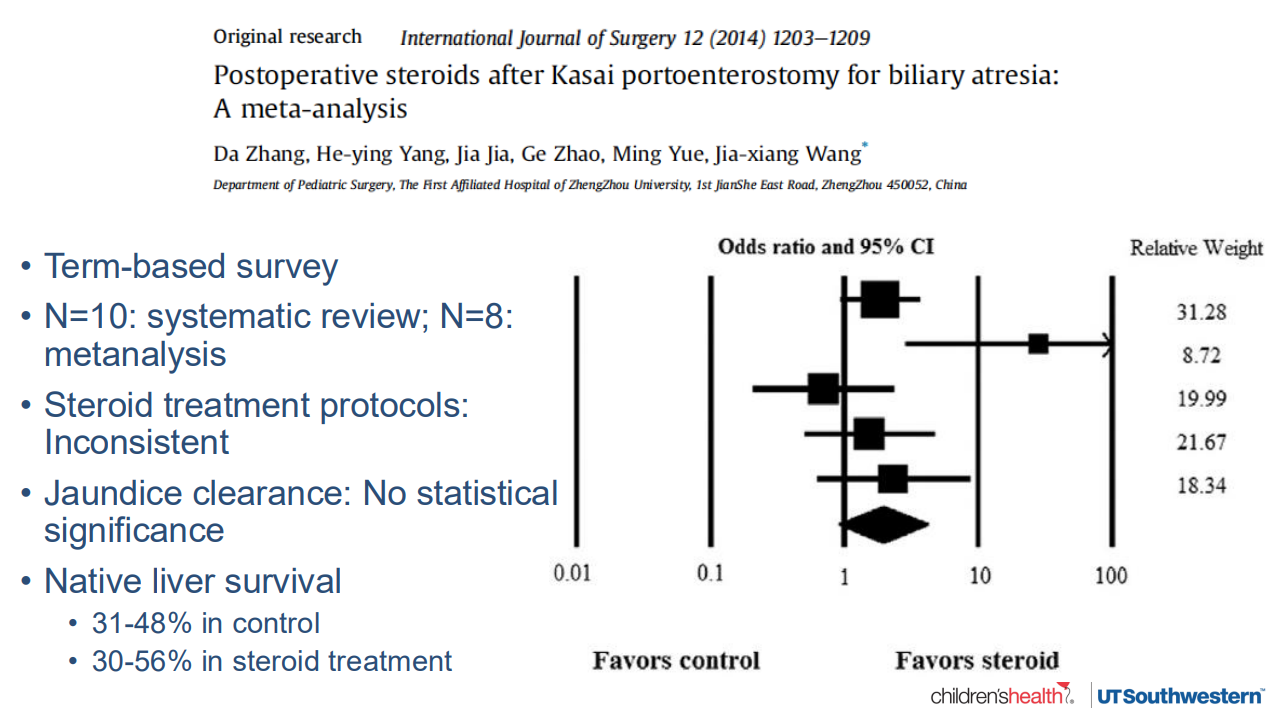
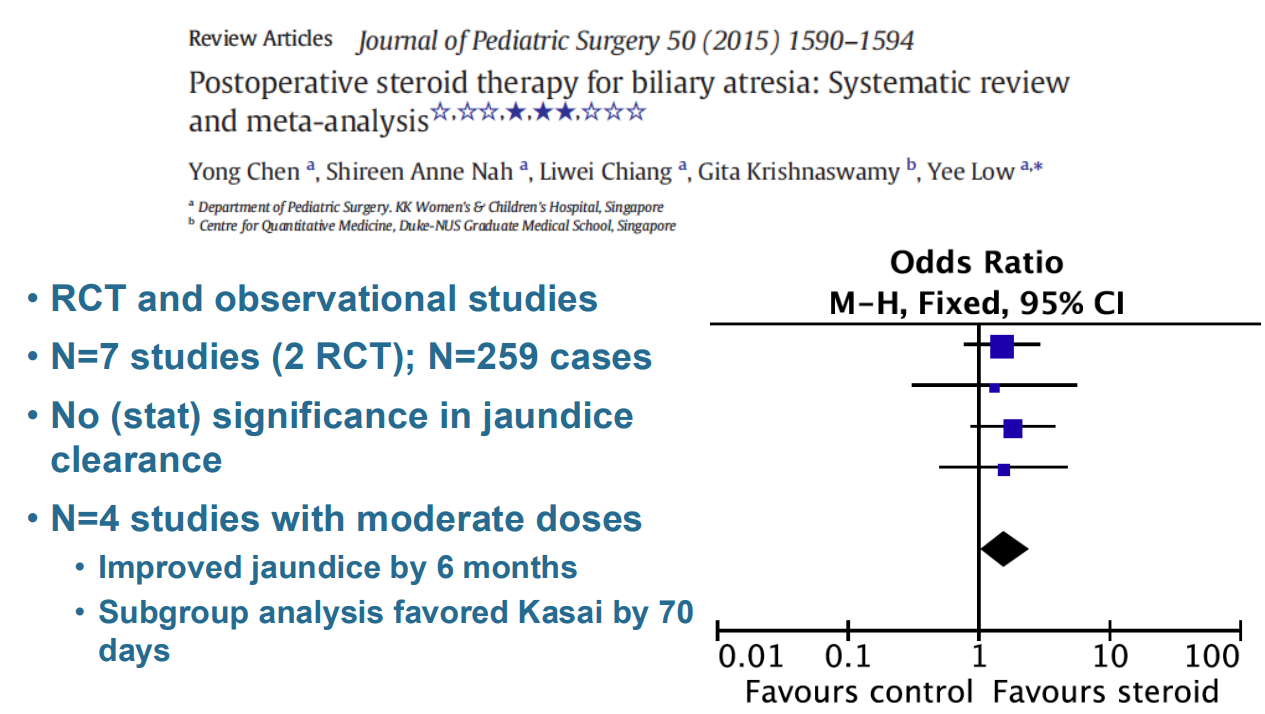
Hepatoportoenterostomy (HPE) (aka Kasai procedure) is effective in about half of patients. The remainder develop complications that include recurrent cholangitis, portal hypertension, and cirrhosis which may lead to the need for liver transplantation
10-year survival rates for liver transplantation are >85%.
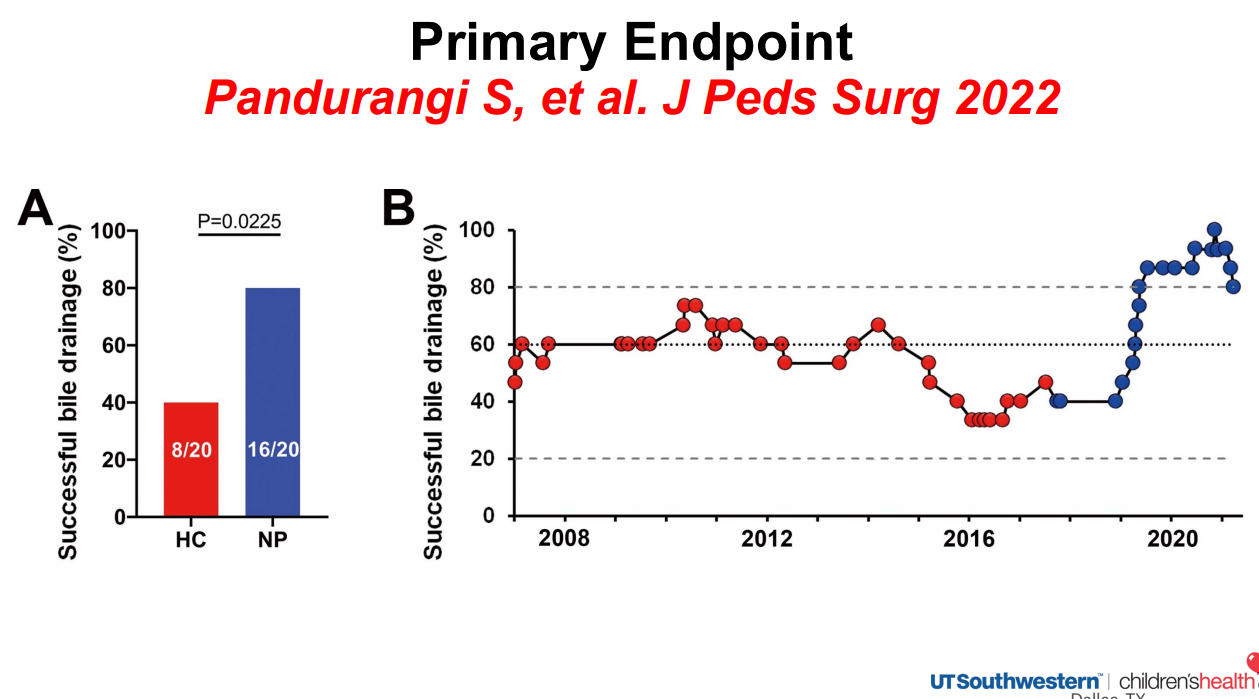
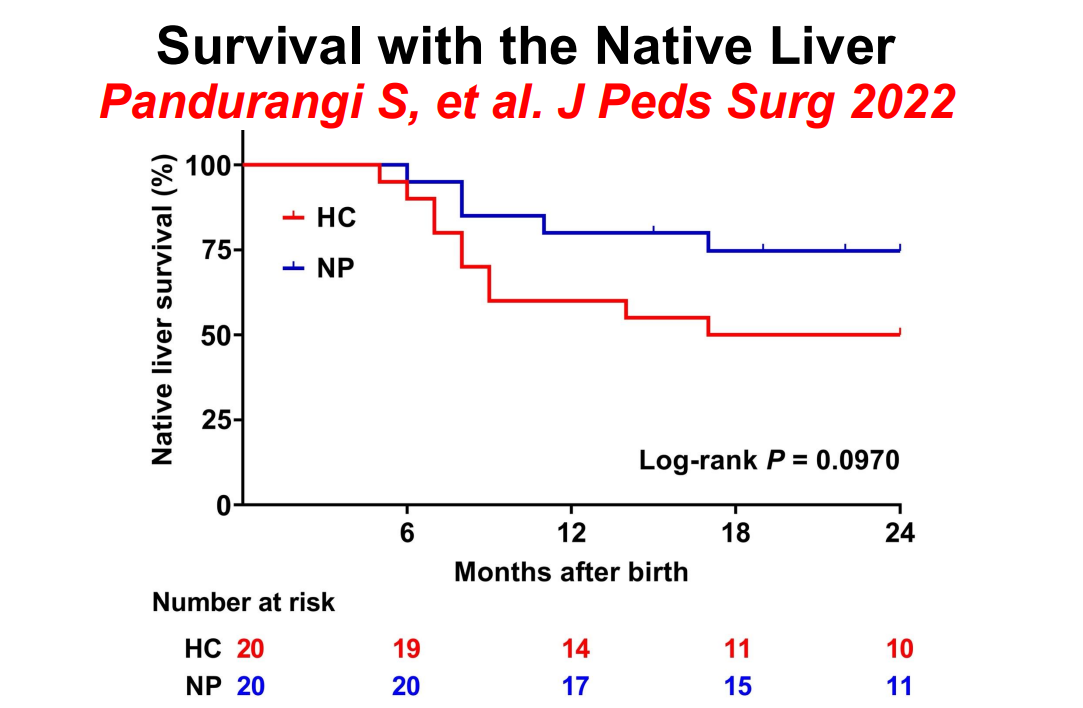
Historical controls in red and new protocol in blue
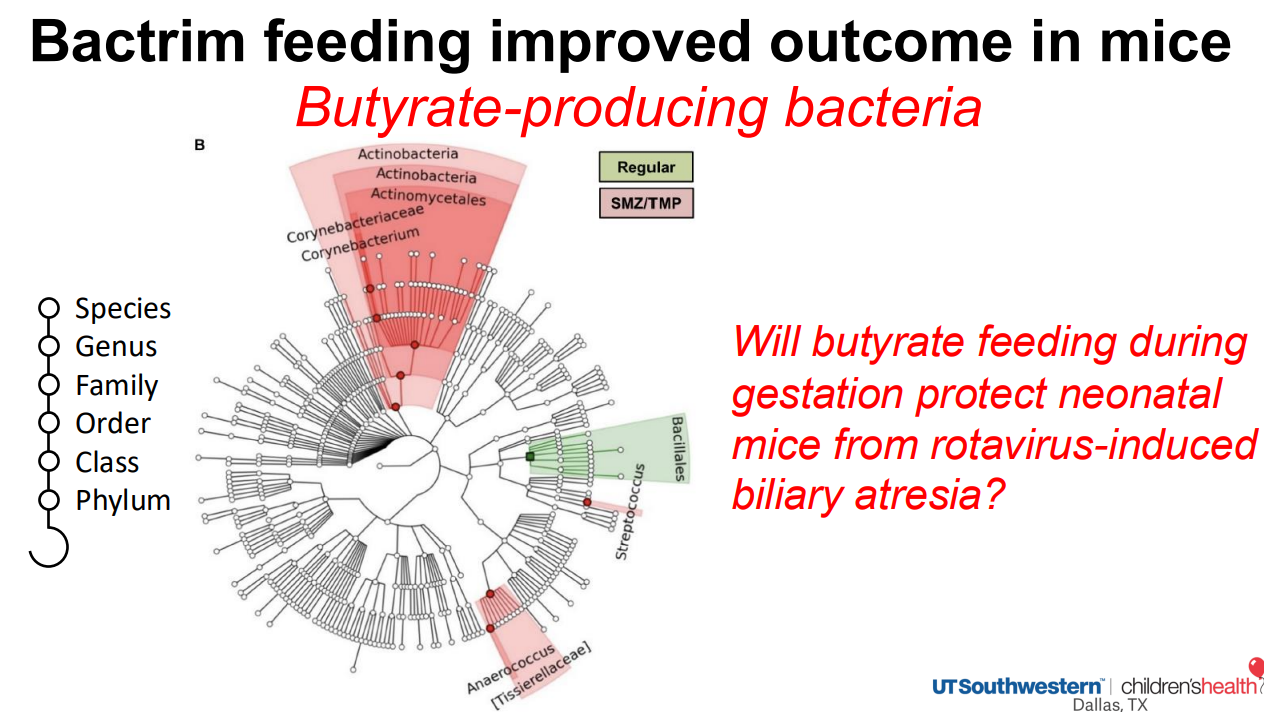
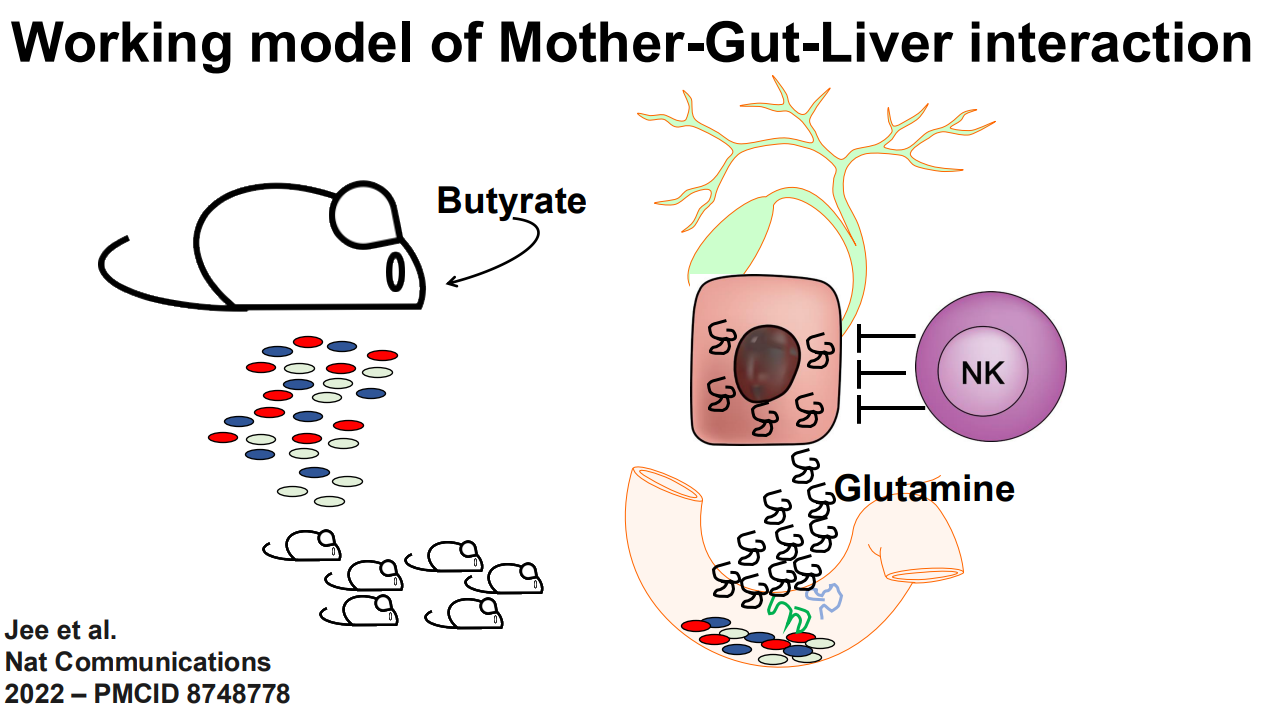
The role of the microbiome is being explored as a factor in the predisposition to BA
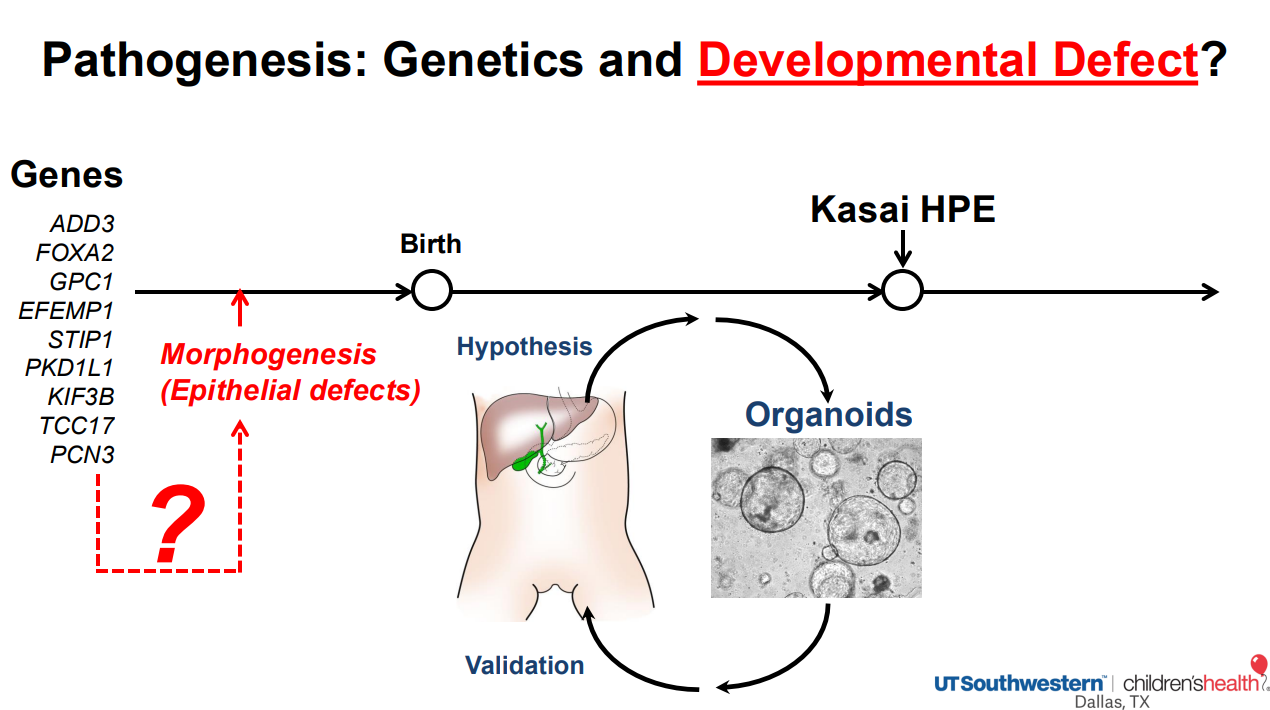
Biliary atresia organoid studies: Biliary atresia organoids had decreased expression of genes related to EGF signaling and FGF2 signaling. When treated with EGF+FGF2, biliary atresia organoids expressed differentiation markers, which restored polarity (Reference: Hepatology 2022 Jan;75(1):89-103. doi: 10.1002/hep.32107. Biliary organoids uncover delayed epithelial development and barrier function in biliary atresia). Thus, these organoids can help understand the underlying pathogenesis and may lead to improved treatments
More recently, compared to normal liver organoids, the epithelium of BA organoids was fragmented and peribiliary glands (PBGs) were small, had abnormal intercellular junction (ZO1 expression), and expressed markers of epithelial-mesenchymal transition (EMT), with a prominent expression of TGF-β3. Upon TGF-β inhibition, EMT decreased in the diseased epithelium, the population of PBGs increased, and ZO1 expression improved. In vivo, TGF-β inhibition suppressed the BA phenotype and substantially decreased liver fibrosis in neonatal mice. Thus, the modulation of TGF-β-dependent EMT regulates bile duct epithelial development and influences the susceptibility of neonates to biliary injuries. (Reference: Nat Commun 2025 Jul 17;16:6575. doi: 10.1038/s41467-025-61442-5. Open Access! Cellular crosstalk mediated by TGF-β drives epithelial-mesenchymal transition in patient-derived multi-compartment biliary organoids)
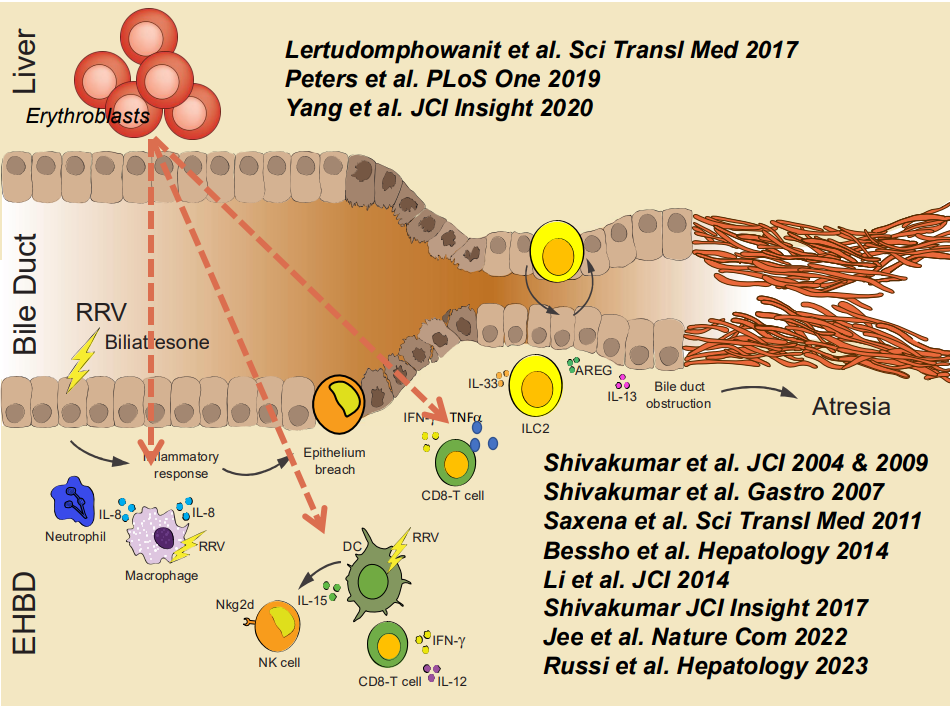
RRV (rhesus rotavirus) can create an experimental model of BA in the mouse. In this mouse model, ILC2 cells (innate lymphoid cells in yellow) play a role in bile duct proliferation, possible attempt at recanalizing damaged bile ducts
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition