This study had a clever design: the authors examined the liver findings from overweight/obese children (n=168) who underwent renal ultrasounds to help determine the frequency of hepatic steatosis. Quantification of the hepatorenal index (HRI) by ultrasound has been shown to provide moderate diagnostic performance for detecting hepatic steatosis in children. (Ref: Frankland MP et al. Diagnostic performance of ultrasound hepatorenal index for the diagnosis of hepatic steatosis in children. Pediatr Radiol. 2022; 52(7): 1306-1313)
This design helped avoid a selection bias present in most studies which have examined ultrasonography in children with elevated liver enzymes. The authors did try to correlate the imaging findings with blood tests. Serum laboratory data were available for 50 patients at a mean interval of 115 days (0–366) from the ultrasound examination.
Key findings:
91 (54%) patients had an abnormally elevated HRI (>1.75). An abnormally elevated HRI was present in 58% (50/86) of patients with overweight and 50% (41/82) of patients with obesity
Of the 12 patients with abnormal ALT, 5 (42%) had an abnormal ultrasound HRI and 7 (58%) had a normal ultrasound HRI
Discussion points:
“MASLD can occur at a very young age and should be considered in at-risk patients. Importantly, only 21% (5/24) of the patients with imaging evidence of steatosis and available labs had elevated ALT and 58% (7/12) of patients with an elevated ALT did not have imaging evidence of steatosis, suggesting that ALT may not be a useful biomarker for MASLD screening at this age.”
My take: Hepatic steatosis is likely present in about half of children with early onset overweight/obesity. ALT values are often normal in this cohort.
Methods: In this single-center, observational study, the authors deployed an anonymized survey of outcomes that was completed by 107 parents of children with BA who were younger than age 12 years. A detailed assessment of general neurodevelopment (Mullens Scale of Early Learning and Vineland Adaptive Behavior Scale) was carried out in 50 infants younger than 5 years old, and emerging autistic traits (Autism Diagnostic Observation Schedule) were assessed in those eligible. There were 93 matched controls.
Key findings:
Neurodevelopmental concerns were raised by 37% of parents
47% of children required support from at least 1 service (such as speech and language therapy physiotherapy, play therapy, or seen a clinical psychologist), and a further 42% (n = 45) had used more than 1 service. The most accessed service was speech and language therapy (20%, n = 10)
A clinical or research diagnosis of autism was made in 30% of 35 children >2 years old
Early surgical intervention and faster clearance of jaundice after surgery was associated with better general neurodevelopmental outcomes (F = 2.428, P = .042) but not with the presence of emerging autistic traits
My take: High levels of neurodevelopmental difficulties occur in children with BA.
I am not an expert on autism. However, I am concerned about the administration’s recent recommendations regarding acetaminophen and autism. Even scientists who have suggested a possible link have NOT recommended stopping the use of acetaminophen during pregnancy.
It is well-recognized that autism is related to multiple factors, both genetic and potential environmental factors. The use of acetaminophen, even if linked to autism, could represent an epiphenomenon in which a primary disorder (like a fever or infection) is responsible for subsequent neurodevelopmental problems rather than the medicine itself. While there has been growing concern about the increasing frequency of autism, much of this relates to changes in the definition of autism over various periods.
I recommend the following recent sources of information on this topic:
Editorial Board Wall Street Journal, 9/23/25: Trump, Tylenol and the Plaintiffs Bar “The acetaminophen link to autism is based on weak evidence pushed by RFK Jr. and his legal allies.”
“Today’s announcement by HHS is not backed by the full body of scientific evidence and dangerously simplifies the many and complex causes of neurologic challenges in children. It is highly unsettling that our federal health agencies are willing to make an announcement that will affect the health and well-being of millions of people without the backing of reliable data.
“In more than two decades of research on the use of acetaminophen in pregnancy, not a single reputable study has successfully concluded that the use of acetaminophen in any trimester of pregnancy causes neurodevelopmental disorders in children. In fact, the two highest-quality studies on this subject—one of which was published in JAMA last year—found no significant associations between use of acetaminophen during pregnancy and children’s risk of autism, ADHD, or intellectual disability.
“Acetaminophen is one of the few options available to pregnant patients to treat pain and fever, which can be harmful to pregnant people when left untreated. Maternal fever, headaches as an early sign of preeclampsia, and pain are all managed with the therapeutic use of acetaminophen, making acetaminophen essential to the people who need it. The conditions people use acetaminophen to treat during pregnancy are far more dangerous than any theoretical risks and can create severe morbidity and mortality for the pregnant person and the fetus.”
From KFF News:
In August, Bauer and her colleagues published an analysis of 46 previous studies on Tylenol, autism, and attention-deficit/hyperactivity disorder. Many found no link between the drug and the conditions, while some suggested Tylenol might occasionally exacerbate other potential causes of autism, such as genetics.
Bauer, an epidemiologist at the University of Massachusetts-Lowell, and her team called for more judicious use of the drug until the science is settled.
Autism experts at the Centers for Disease Control and Prevention were neither consulted for the White House’s long-awaited autism announcement nor asked to review a draft of the findings and recommendations…
If prenatal Tylenol has any association, which it may not, it would help account for only a fraction of cases, she said. Further, research has not deeply examined Tylenol risks in young children, and manyrigorous studies refute a link between vaccines and autism.
Bauer worries such statements will cut both ways: People may put themselves at risk to avoid vaccines and Tylenol, the only safe painkiller for use during pregnancy. And she frets that scientists might outright reject her team’s measured concerns about Tylenol in a backlash against misleading remarks from Trump and other members of his “Make America Healthy Again” movement….
Helen Tager-Flusberg, director of the Center for Autism Research Excellence at Boston University, called Trump’s comments dangerous. Fevers can harm the mother and the developing fetus, she said, adding that fevers are more strongly associated with autism than Tylenol…
Several medical and scientificassociations have called for Kennedy’s removal or resignation. Many scientists are skeptical of what he says because much of it has been misleading or wrong. For example, he’s said HIV isn’t the only cause of AIDS (it is), that antidepressant drugs cause mass shootings (they don’t), that older adults don’t have severe autism (some do), that the measles vaccine causes brain swelling (it doesn’t), that covid vaccines were the deadliest vaccines ever made (they aren’t), that vaccines aren’t safety-tested (they are), and that vaccines contribute to autism (they don’t).
From the Wall Street Journal:
Washington Post Editorial:
From TIME article: “Despite what we are now hearing from the most powerful health offices in the nation, the science on acetaminophen and autism remains unsettled. What is not unsettled is the damage done when politics masquerades as medicine. Every false certainty erodes the trust that holds the fragile bridge between patients and their doctors. Break that trust, and no study, no drug, no vaccine will be enough to save lives when the next real crisis comes. When politicians play doctor, it’s families who will pay the price.”
My take: Thinking about the damage from this press conference, I was reminded of a scene from the movie “Doubt.” In the movie Doubt, Father Flynn (played by Philip Seymour Hoffman) tells a parable about an old priest instructing a woman who has been gossiping to take a pillow, cut it open on her roof, and then return to gather up all the feathers. When she tells him it can’t be done because “the wind took them all over,” the priest responds: “And that… is gossip!”
The spreading of damaging rumors and lies, which is being done by leaders of this country, is impossible to contain or undo once released, and its impact is far-reaching and destructive.
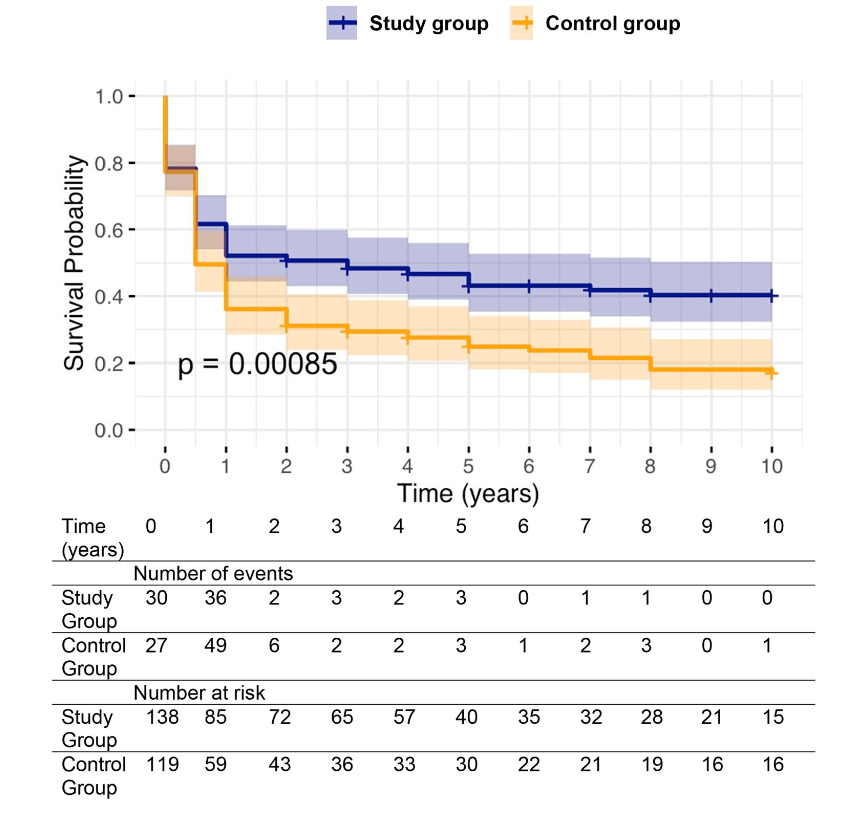
Background: After the START trial in 2014, it seemed that enthusiasm for post-operative steroids for biliary atresia had waned. The START study did not find that steroids improved outcomes after Kasai hepatoportoenterostomy (HPE). Subsequently, though, there have been observational reports of using steroids in a customized fashion to improve outcomes. Langreen et al add to this literature by examining their use of rectal budesonide (2 mg) for 3 months in a retrospective cohort (n=142) with a historical control (n=137). Jaundice-free native liver survival (jfNLS) was assessed at 6 months, 2 years, 5 years, and 10 years post-Kasai.
Key findings:
Improvements were noted in jfNLS at 6 months (53% vs. 39%) , 2 years (45% vs. 22%), 5 years (40% vs. 23%) and 10 years (32% vs. 13%)
These benefits were exclusive to patients with nonsyndromic BA
No serious adverse effects were identified with budesonide
Rationale for rectal budesonide: The authors note that “a single dose of budesonide foam contains about 2 mg of budesonide, equivalent to 25 mg of prednisolone or 20 mg of methylprednisolone…In our series, no serious steroid associated adverse effects were recorded, possibly due to the first pass after rectal administration.”
Limitations: “The retrospective nature of our data analysis allows for variability in the follow‐up protocols, potential biases (historical control group, change of surgeons) and confounding factors cannot be entirely ruled out.”
Kaplan–Meier curve comparing native liver survival between the study and control groups over a 10‐year follow‐up.. Study group—blue. Control group—orange.
My take: The START study with 140 participants was well-designed and did not find a benefit with systemic steroids. However small differences in outcomes can be difficult to identify. Rectal budesonide may improve outcomes. A randomized, double-blind, placebo-controlled trial would be more definitive.
LT is resource-intensive and costly, with expenditures rising dramatically in recent years. Factors contributing to this increase in cost include expanded transplant criteria (higher risk recipients), utilization of marginal organs, and broader organ distribution, resulting in significant logistical expenses
Advanced technologies like organ perfusion devices, while promising better outcomes, further inflate costs due to their high price and market monopolization
Despite rising costs, reimbursement has remained largely stagnant, putting financial strain on transplant programs, and threatening their sustainability. “In fact, there has been an observed decline (−32%) in adjusted reimbursement of LT by Medicare over the past decade.62“
“According to the latest annual SRTR report, patients aged 65 or older undergoing LT accounted for 21.9% of transplants in 2022, up from 14.6% a decade prior.18 One study looking at the cost burden of hospitalizations associated with liver transplants from 2016 to 2019 found mean costs increasing by nearly $10,000 per hospitalization in the group aged >65 over the study period”
“Increasing numbers of patients are being transplanted for steatotic liver disease… LT associated with metabolic dysfunction–associated steatotic liver disease has been demonstrated to be associated with higher costs, largely attributable to longer posttransplant lengths of stay.21–23 Similarly, LT associated with AH/ALD is very expensive—at 1 transplant program, net revenue from LT admission to 90 days after LT was −5.0% for AH compared to +1.4% for acute-on-chronic liver failure.24“
Organ distribution:
“In 2019, the OPTN implemented further changes in liver allocation from a regional-based system to an acuity circle model. This model was intended to create a more equitable allocation system and to reduce waitlist mortality for patients across the United States…This has been associated with a 77% increase in fly-out costs, amounting to an increase in $47,010,190 across all LT centers by recent estimates.4“
“1 study found that the cost for private jets ranged from $6850 to $27,350 depending on the distance traveled.29 In this same study, commercial flights, as opposed to private jets, were found to be safe and only around 10% of the cost.”
Perfusion devices:
“The FDA’s approval of organ perfusion and preservation devices has ushered in a new era in organ transplantation, enabling medical teams to extend the geographical reach for organ procurement. These devices enhance the utilization of organs that may have previously been discarded… It has been suggested that the average cost of using normothermic regional perfusion for DCD organs is around $10,000 per donor, compared to the $40,000–$80,000 per donor for use of NMP [normothermic machine perfusion].”
My take: Transplant centers are getting squeezed financially. In addition, ~25% of liver transplant patients experience a high financial burden. Pretty soon, along with checking organs for suitability, it may be necessary to assess liver transplant centers for viability.
Methods: This was a a multicenter, retrospective, observational study of fidaxomicin treatment for primary or recurrent CDI in children ages 12 months to 18 years old identified from 2013 to 2021 at 5 centers. Inclusion criteria were active CDI, defined as ≥3 watery stools in 24 hours and a positive laboratory test (toxin enzyme immunoassay positivity and/or polymerase chain reaction [PCR] positivity). Cure was defined as resolution of symptoms.
Patient characteristics:
Of the 95 patients included in this study, 84 (88%) were treated with fidaxomicin for a recurrent CDI, and 82 (86%) had at least one medical or surgical comorbidity.
38 (40%) patients had 4 or more CDI prior to fidaxomicin.
22 (23%) had prior FMT.
29 (31%) had IBD
Key findings:
By day 14 (end of treatment): 50 patients (52.6%) had a clinical cure and an additional 29 (30.5%) had improvement of symptoms. Thus, 17% did not respond to treatment.
Among 79 patients who responded to fidaxomicin treatment, 17 (21.5%) had a clinical and microbiologically confirmed recurrence of CDI by day 60, likely representing relapse.
Patients with inflammatory bowel disease were less likely to achieve clinical cure at day 14 (OR 0.27). 9 of 29 were considered treatment failures.
If the patient’s with IBD are excluded (n=66), there were only 7 (11%) treatment failures
Discussion points:
“Our clinical experience is that approval for coverage by insurers often is restricted to those with recurrent CDI, and the cost of fidaxomicin may limit availability for use as primary therapy.”
“CDI in IBD is a major clinical conundrum as the symptoms of the 2 disorders can overlap, and a positive C. difficile test is not always indicative of its active pathologic role…Therefore, patients who undergo treatment for CDI without response likely have an alternative cause of symptoms…. Current guidelines recommend reassessing symptoms in patients with IBD being treated for CDI at day 3 or 4 of the treatment course in order to consider escalation of IBD therapy in those who are not responding clinically to antimicrobial therapy.”
My take (borrowed from the authors): “More extensive studies are necessary to understand how to position fidaxomicin in the treatment algorithm for pediatric CDI.”
Methods: Single-center, retrospective study of children (4–21 years old, n=191) with biopsy-proven Celiac disease (CeD) who were evaluated for DGBI based on Rome IV criteria. Patients who were adherent to a GFD, demonstrated tissue transglutaminase immunoglobulin A (TTG IgA) decline, and had at least one visit 9–24-months after diagnosis with a pediatric gastroenterologist. For this study, sustained TTG IgA decline required at least two declining TTG IgA values, a 90% decline from baseline, or normalization of TTG IgA.
Key findings:
43% (n = 83) met Rome IV DGBI diagnostic criteria.
Functional constipation (27/83, 33%) and functional abdominal pain (24/83, 29%) were the most common DGBI
Abdominal pain, constipation, and vomiting at initial presentation as well as comorbid joint hypermobility, headaches, and chronic musculoskeletal pain increased risk of developing DGBI after serological decline
Discussion Points:
“The prevalence reported here is similar to a study of adults with CeD who were adherent to a GFD that reported over 50% met criteria for a functional gastrointestinal disorder19 and is higher than previously reported pediatric prevalence rates”
“The majority of patients who met DGBI criteria did so through having the persistence of the same gastrointestinal symptoms that were present at CeD diagnosis. This raises the question as to whether the symptoms at presentation were due to CeD, DGBI, or both”
“Clinicians could consider discussing that while symptoms related to CeD should improve on a GFD, some symptoms may persist, especially if they have an increased likelihood of having a comorbid DGBI. Such counseling may prevent the misattribution of persistent symptoms to ongoing gluten exposure and mitigate hypervigilance”
“Having complete villous blunting on diagnostic biopsy increased the likelihood of having a DGBI. Intuitively, it is possible that complete villous blunting can lead to greater nerve sensitization and subsequently higher rates of DGBI. It is also possible that complete villous blunting is slower to recover”
My take: Given the overlap of DGBI symptoms with CeD, diagnosing DGBI in patients with CeD can be challenging. However, DGBI is much more likely to contribute to lingering symptoms than refractory CeD.
As a practical matter, the high frequency of ongoing GI symptoms despite use of a GFD provides another drawback to relying on a no-biopsy diagnosis. A no-biopsy diagnosis introduces greater uncertainty in the diagnosis and does not allow for a histologic comparison if a subsequent evaluation is needed.
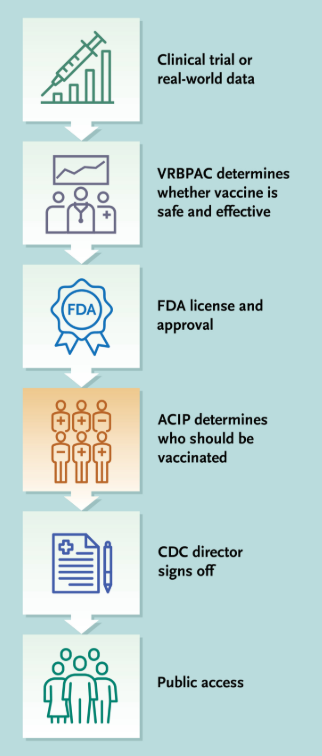
This commentary was published on 7/30/25 and was written by the 17 voting members of the ACIP who were dismissed.
Key points:
For over 60 years, the Advisory Committee on Immunization Practices (ACIP), which comprised a diverse group of nonpartisan specialists, has advised the Centers for Disease Control and Prevention (CDC) on vaccine recommendations based on science and intensive review of evidence. The abrupt dismantling of the rigorously vetted process and the replacement of the Committee with an inexperienced and biased panel has engendered fundamental distrust in the Committee’s vital work…The government has abruptly changed vaccine policy through social media postings and publications in news media.
**VRBPAC denotes FDA’s Vaccines and Related Biological Products Advisory Committee
The ACIP has been an independent committee of vaccine scientists and clinicians that has relied on a process called the Evidence to Recommendations framework. This deliberative framework calls for a review of the strength of evidence around a variety of factors, including the magnitude of the public health problem, potential benefits and harms, values, acceptability, resource use, equity, and feasibility.
Previously, the ACIP had well-defined and stringent conflict of interest standards. Voting members had to disclose and actively manage any actual or apparent conflicts of interest before and throughout their tenure… ACIP members disclosed any potential conflicts during each vote and could not vote on issues where they had an ongoing conflict.
ACIP recommendations have many implications. For example, government-run medical systems such as the Veterans Health Administration may be able to provide only vaccines consistent with ACIP recommendations…For children who are uninsured, underinsured, Medicaid-eligible, American Indian, or Alaska Native, the Vaccines for Children program pays only for ACIP-recommended vaccines; about half of children in the United States get their vaccines through this program.
The nation now faces a scenario in which the rigor and discipline of these vaccine recommendation processes are rapidly eroding…Three major issues are of particular concern: the quality and availability of data; straightforward guidance for providers and the public; and insurance coverage and vaccine access, uptake, and equity.
The absence of a cohesive federal policy produced by means of an evidence-based, expert-informed process creates the very real potential for conflicting messaging from within the Department of Health and Human Services (DHHS) or in relation to messages from nongovernmental agencies, such as professional organizations. This lack of coordination is likely to cause confusion for providers and the public, vaccine-administration errors, decreased uptake of vaccines, and further erosion of an already damaged public trust. It is also likely that in this milieu, misinformation will flourish.
The ACIP cannot be replaced, but it may be possible to limit the damage. In this vacuum, it is urgent that other organizations step forward to reassert an evidence-based, expert approach to vaccine recommendations to bring the nation back from the precipice of uncontrolled spread of infectious diseases and needless deaths.
My take: The advice from governmental agencies has been compromised. With regard to vaccines, instead of a transparent process with expertise, we are left with partisan recommendations with questionable credibility.
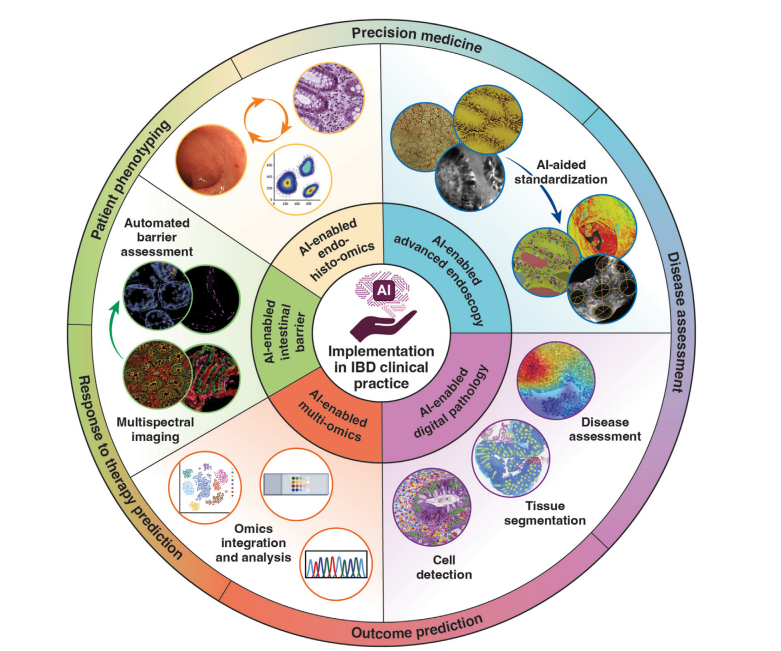
This month’s Gastroenterology issue is devoted solely to the use/expected uses as well as risks of artificial intelligence (AI) for gastroenterology and hepatology.
“AI is reshaping the landscape of gastroenterology and hepatology with the promise of better, faster, more objective, and standardized care of delivery. However, behind the algorithms lies a more insidious risk: the erosion of trust in human providers…Information risk …include both error commission (ie, when the models generate false statements, introduce nonsensical concepts, or fabricate sources) and error omission (ie, summaries that omit critical information)…
When AI becomes the center of care, patients may perceive their doctors as intermediaries…diminishing the therapeutic effect of the patient-physician relationship…This arrangement can dilute clinical training, increase physician burnout, and lead to medicolegal implications…Other risks include perpetuating bias from nonrepresentative training data and amplifying uncertainty of AI due to lack of real-world validation…
We hope that AI systems will allow us to spend more, not less, time with patients and empower us to provide personalized care by leveraging high-quality multimodal data.”
Most of the articles are behind a paywall in this issue. There are five that are open access articles:
My take: These articles provide a good deal of information about the applications and risks of AI. In my view, physicians will be needed more than ever to help interpret/manage the huge amount of information available.
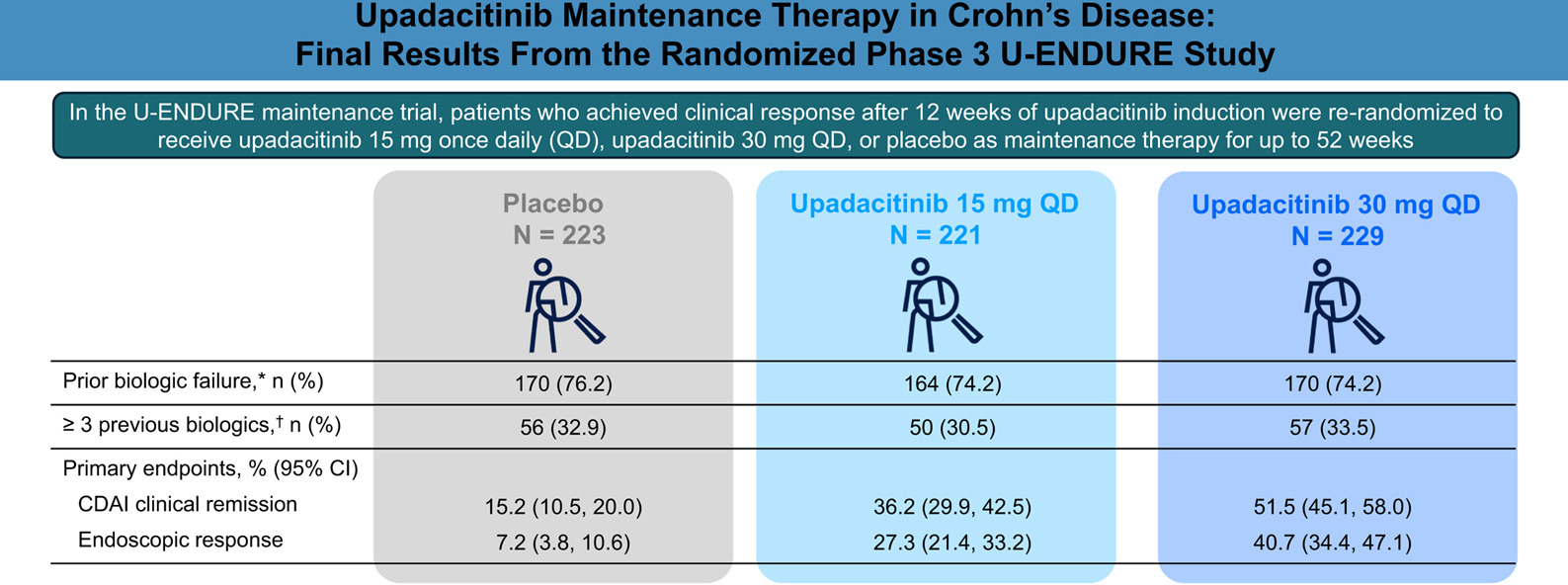
Methods: Clinical responders to 12 weeks of upadacitinib 45 mg once daily (QD) induction were randomized (1:1:1) to receive upadacitinib 15 mg QD (n = 221), upadacitinib 30 mg QD (n = 229), or placebo (n = 223) as maintenance therapy for 52 weeks
**This study presents data from the entire cohort (n=673); a previous report from ENDURE-3 analyzed data on 502 patients (though findings were nearly identical). EV Loftus et al. N Engl J Med 2023; 388:1966-1980 (Related post: Landmark Study: Oral Biologic for Crohn’s –Upadacitinib)
Key findings:
At week 52, more upadacitinib-treated vs placebo patients achieved CDAI clinical remission (upadacitinib 15 mg, 36.2% and upadacitinib 30 mg, 51.5% vs placebo, 15.2%)
The rates of endoscopic response were 27.3% for upadacitinib 15 mg and 40.7% for upadacitinib 30 mg vs 7.2% for placebo
Herpes zoster infections occurred more frequently in the upadacitinib groups compared with placebo; all were nonserious, and most involved a single dermatome
In U-ENDURE, no dose-dependent risk for MACE, VTE, or malignancy (excluding NMSC) was observed during the 52-week maintenance period
My take: Upadacitinib is a effective in a good number of patients with with moderately to severely active Crohn’s disease who have been refractory to other advanced therapies.