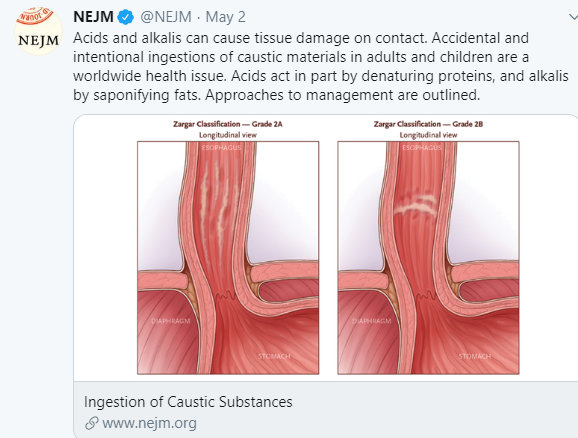
The week that the U.S. President suggested that using disinfectants to treat the coronavirus could be helpful, there was a spike in calls to poison control centers: Calls to poison control centers spike after Trump disinfectant comments. In addition, coincidentally, a review article was published: Ingestion of Caustic Substances (RS Hoffman et al. NEJM 2020; 382: 1739-48).
Background:
- Chevalier Jackson (1865-1958), an otolaryngologist and often called the ‘father of endoscopy,’ advocated for warning labels on bottles that contained caustic agents.
- U.S. Federal Caustic Poison Act 1927 mandated labeling and U.S. Poison Prevention Packaging Act 1970 mandated child-resistant containers
- Currently, poison control centers in the U.S. advise storage “up and away” of caustic agents (Great website for families: www.upandaway.org)
Epidemiology:
- Nearly 1000 children are hospitalized each year with caustic ingestions.
- In younger children, ingestions typically involve smaller amounts than in adolescents and adults (in which ingestions are usually deliberate attempts at self-harm)
Clinical Outcomes:
- GI: Caustics (both acid and alkali) may result in esophageal perforations with mediastinitis, as well as bowel perforation and bleeding. Esophageal strictures can develop weeks to months afterwards
- ENT: May compromise airway
- Eye/Skin: Splash may cause eye injuries and skin burns
Approach to Management:
The authors present an algorithm (Figure 1) –Key points:
- For adults and adolescents, when there are oropharyngeal findings with intentional ingestions, there is a high likelihood of gastroesophageal injury. In younger children, the presence of oropharyngeal findings is much less likely to be associated with gastroesophageal injury due to smaller ingested quantities.
- The authors advocate a selective approach towards endoscopy in young children. “For children with only vomiting or drooling and those who refuse to drink, overnight observation is routine, and endoscopy is performed only if symptoms persist and the child remains unable to take oral fluids” If there is vomiting and drooling or stridor alone, endoscopy is recommended.
- Endoscopy, when indicated, “should be performed in the first 24 to 48 hours.” Delayed endoscopy may increase the risk of perforation.
- Clinical attempts to empty the stomach can potentially increase injury. However, “use of water immediately after ingestion (usually at home) to irrigate adherent materials” may be useful if patient can swallow safely and breathe without difficulty.
Grading Esophageal Injury -Zargar Classification:
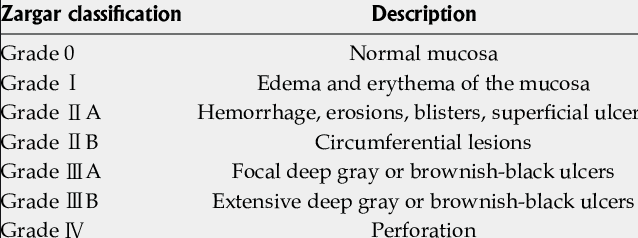
For patients too ill to undergo endoscopy, CT is an alternative
Use of Corticosteroids:
This issue is discussed at length. Though routine use of steroids failed to show benefit in several (underpowered) studies, the authors not that Usta et al (Pediatrics 2014; 133: E1518-24) “randomly assigned children with grade 2B esophageal injuries to 3 days of methylprednisolone ( 1 g per 1.73m2 of BSA per day) or placebo, plus 1 week of ceftriaxone and ranitidine…A significant benefit was reported in the methylprednisolone group.” Thus, “patients with grade 2B injuries, who have a high risk of progression to stricture and a low risk of perforation, are most likely to benefit from…glucocorticoid therapy.” The authors state this is in agreement with current guidelines (JPGN 2017; 64: 133-53).
Other Management:
- Consider placement of nasogastric tube at time of endoscopy
- Sucralfate has been shown to help with esophageal healing
- Mitomycin C has been studied and has some data indicating fewer dilatations were needed for caustic-induced strictures. Long-term risk of malignancy with mitomycin C is uncertain.
My take: Most children with caustic ingestions will not need endoscopy. Sucralfate is a useful adjunct. A subset of children may benefit from 3 days of methylprednisolone.
Related blog posts:
- Esophageal disorders: POEM and Mitomycin C
- Detergent Pod Ingestions -Is an Endoscopy Needed? | gutsandgrowth
- New caustic danger from detergent pods
- Great website for families: www.upandaway.org)
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition