A good 4 minute YouTube video: Brene Brown on Blame
Related blog post: Empathy vs. Sympathy


A recent randomized trial (YB Werner et al. NEJM 2019; 381: 2219-29) compared peroral endoscopic myotomy (POEM) and laparoscopic Heller’s myotomy (LHM) for idiopathic achalasia in 221 patients.
Key findings:
My take: This study demonstrates similar outcomes between POEM and LHM. As a practical matter, local expertise is likely a crucial component in choosing between these options.
Related blog posts:

Several years ago, a small study showed that bolus feeds were as well-tolerated in premature infants as drip feeds: Which is Safer -Drip Feeds of Bolus Feeds for Preterm Infants?
Now, a retrospective study (LB Mahoney, E Liu, R Rosen. JPGN 2019; 69: 678-81) found no difference in the rate of reflux in 18 children who were with gastrostomy-tube dependent.
In this study, 24-hour multichannel intraluminal impedance with pH monitoring (MII-pH) examine reflux events in children receiving exclusive enteral nutrition with a combination of daytime bolus feeds and overnight continuous feeds; each patient served as their own control. this included 6 with prior fundoplication.
Key finding:
The limitations in this study include the small sample size and retrospective design. The authors estimate that to achieve adequate power (80% power) to detect a risk ratio of 1.2 would require 211 patients.
My take: This study and other small studies challenge the assumption that drip feedings are safer. Though, until a larger prospective study is performed, we will not know.

Quebec City
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
A recent study (H Yamamoto et al. Liver Transplantation 2019; 25: 1561-70) provides data on the outcomes of infants who underwent liver transplantation (LT) in the United Kingdom (King’s College Hospital).
A total of 64 infants underwent LT (1989-2014) at a single institution. The authors compared “extra-small” (XS) infants in the first 3 months of life to “small” (S) who were 3-6 months of age.
Key findings:
Related blog posts:

Quebec City, Frontenac Hotel and Boardwalk (early in the day)
A recent retrospective study (N Ibrahimi et al. JPGN 2019; 69: 668-72) reviewed juvenile polyp characteristics over a 14 year period (2003-17) from 213 pediatric subjects who underwent 326 procedures. The authors state their review was intended for nonsyndromic juvenile polyps, though 23 of the patients had ≥5 polyps (which is incongruous with their presented methods of including children with less than 5 polyps).
Key findings:
It is possible that some of the ‘recurrent’ polyps were missed polyps, as polyps can be easily overlooked. I had a recent experience of removing numerous polyps (14) from a child recently and some were identified in part due repeated visualization of several colonic segments. The recent ESPGHAN position paper is useful in children with multiple polyps; their recommendations include: In a child with a single JP, a repeat colonoscopy is not routinely required. (Weak recommendation, very low quality of evidence).
My take: This report is notable for the following:
Related blog posts:

Quebec City
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
A recent NY Times commentary: “Where the Frauds Are Legal” details another group of problems with health care economics. These problems are on top of a long list of other problems which at their core relate to lack of price transparency/hidden charges and excessive charges for some services.
Here’s an excerpt:
Much of what we accept as legal in medical billing would be regarded as fraud in any other sector…
Medical Swag…Companies are permitted by insurers to bill for “durable medical equipment,” stuff you receive for home use when you’re in the hospital or doctors’ office. That yields some familiar marked-up charges, like the sling you can buy at Walgreens for $15 but for which you or your insurer get a bill for $120 after it is given to you at urgent care…
The Cover Charge…Trauma activation fees have been allowed since 2002, after 9/11, when the Trauma Center Association of America, an industry group, convinced regulators that they needed to be compensated for maintaining a state of “readiness.”…
Impostor Billing…We received bills from doctors my husband never met… for bedside treatment from people who never came anywhere near the bed to deliver the care…
The Drive-By…There was no significant health service given. Just an appearance and some boxes checked on a form. It’s a phenomenon called drive-by doctoring.
The Enforced Upgrade…[like meeting] in the emergency room [because clinic is closed]
Why do insurers pay? Partly because insurers have no way to know whether you got a particular item or service. But also because it’s not worth their time to investigate the millions of medical interactions they write checks for each day. Despite the advertised concern about your well-being, as one benefits manager enlightened me: They’re “too big to care about you.”…these are all everyday, normal experiences in today’s health care system, and they may be perfectly legal. If we want to tame the costs in our $3 trillion health system, we’ve got to rein in this behavior, which is fraud by any other name.
My take: I find it troubling to be a cog in a system that has such devious billing practices. This particularly relates to my interactions when providing hospital-based care. In our office, we have at least some measure of control and we can offer services like outpatient endoscopy at one-third of the cost compared to hospital-based endoscopy; similarly, our outpatient infusions are much more cost-effective than hospital-based infusions.
In terms of the health care system, my expectation is that there is not a strong enough incentive or empowerment for physicians to tackle rising health care costs (& low value care) and as such the industry will face a reckoning from outside forces.
Related blog posts:

A recent commentary (M Fralick, AS Kesselheim. NEJM 2019; 381: 1793-5) describes the U.S. Insulin Crisis.
Background:
Current Situation:
My take: Why does insulin cost 15 times more in the U.S. than Canada? These excess costs with insulin are occurring despite a great deal scrutiny; unfortunately, U.S. consumers are paying extra for a wide range of pharmaceuticals. Going from the Nobel discovery of insulin to our current state is a clear indication of the need to reform of our healthcare system.
Related blog posts:

Mural in Quebec City: La Fresque des Québécois




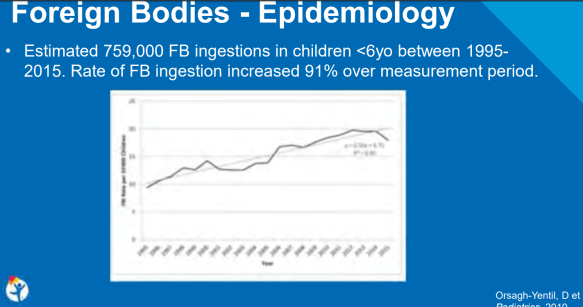
A recent retrospective study (D Orsagh-Yentis) Pediatrics 2019; 143: pii:320181988) examined children <6 years of age (n=759,054) and presentation to an emergency department in the U.S. for a foreign body ingestion (FBI) from 1995-2015. This study was reviewed at our recent national meeting by David Brumbaugh -related blog post: #NASPGHAN19 Postgraduate Course (Part 1) (Slides below).
Key findings:
Related blog posts:

From NY Times: ‘I Have a Ph.D. in Not Having Money’
An excerpt:
Medical school is expensive for everyone. But for low-income students, the hidden costs can be prohibitive…
American medical schools are the training grounds for a white-collar, high-income industry, but they select their students from predominantly high-income, and typically white, households…Between 1988 and 2017, more than three-quarters of American medical school students came from affluent households…
Students from low-income families who choose to apply to medical school find the path lined with financial obstacles. The application phase entails MCAT registration ($315) and preparation, application fees ($170 for the first school and $40 for each additional one), travel and attire for interviews (on average more than $200 per school). After enrollment, students are expected to purchase equipment and study aids. Each year brings new certification tests, with registration fees running upward of $600.
Aspiring doctors know that tuition is costly; the median educational debt held by medical school graduates in 2018 was $200,000, up 4 percent from the previous year. But less advertised are all the hidden costs of a medical education.