

Recently, one of our allergy-immunology colleagues, Dr. Kiran Patel, from Emory presented an update on GI Diseases from an allergist viewpoint at one of our GI clinical education meetings. With his permission, many of the slides are noted below. The slides present a good deal of information, though a lot of nuance and further details were provided by Dr. Patel.
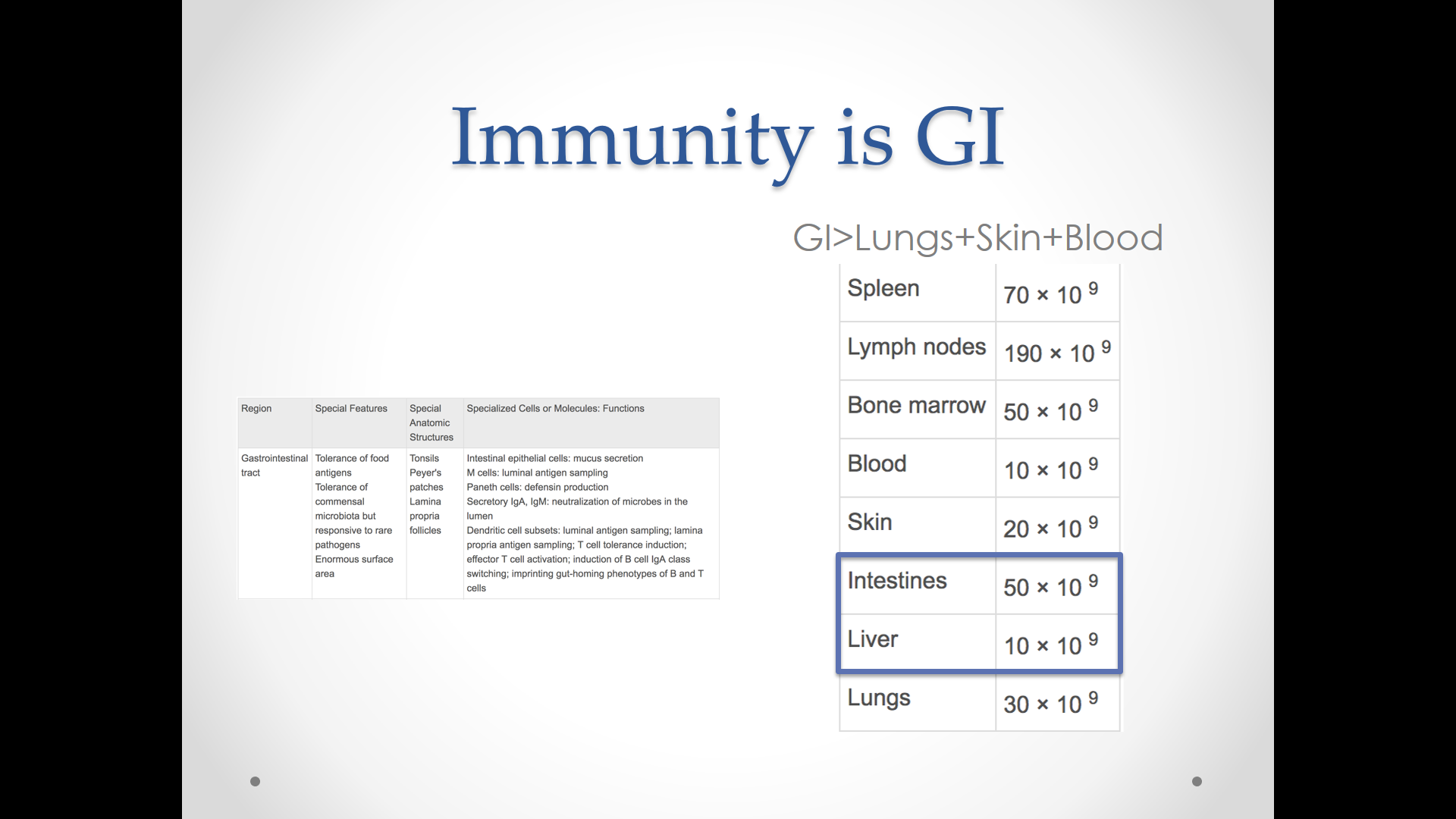
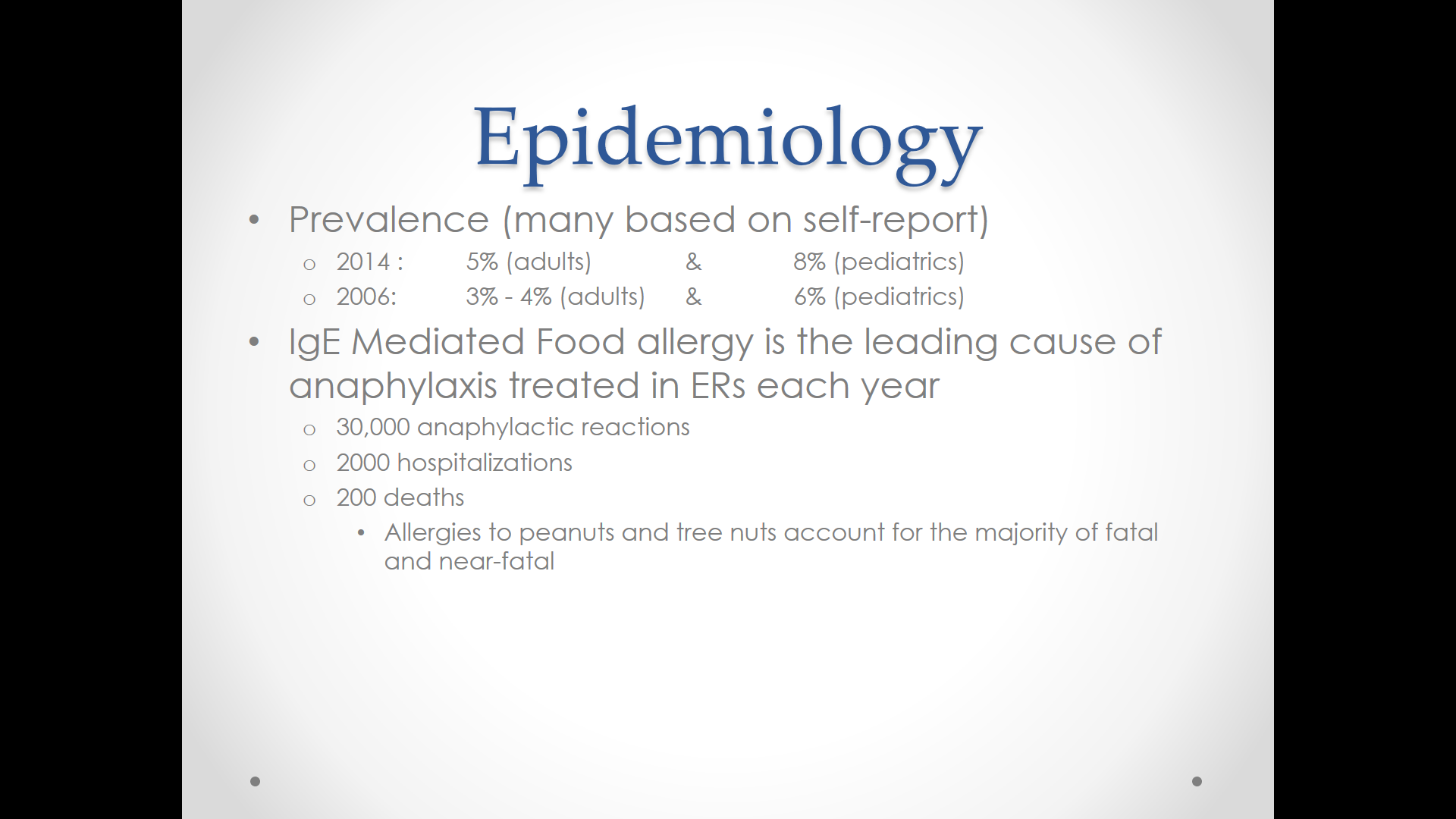
Next few slides discuss typical GI food allergies. It is not surprising that a lot of allergies manifest with GI symptoms given the amount of immune cells in the intestines and frequent interactions with foods and antigens.
This next slide points out that four of the most common food allergens (cow’s milk, egg, soy, and wheat) are frequently outgrown, whereas with peanuts, tree nuts, fish, and shellfish, it is uncommon to outgrow these allergies..

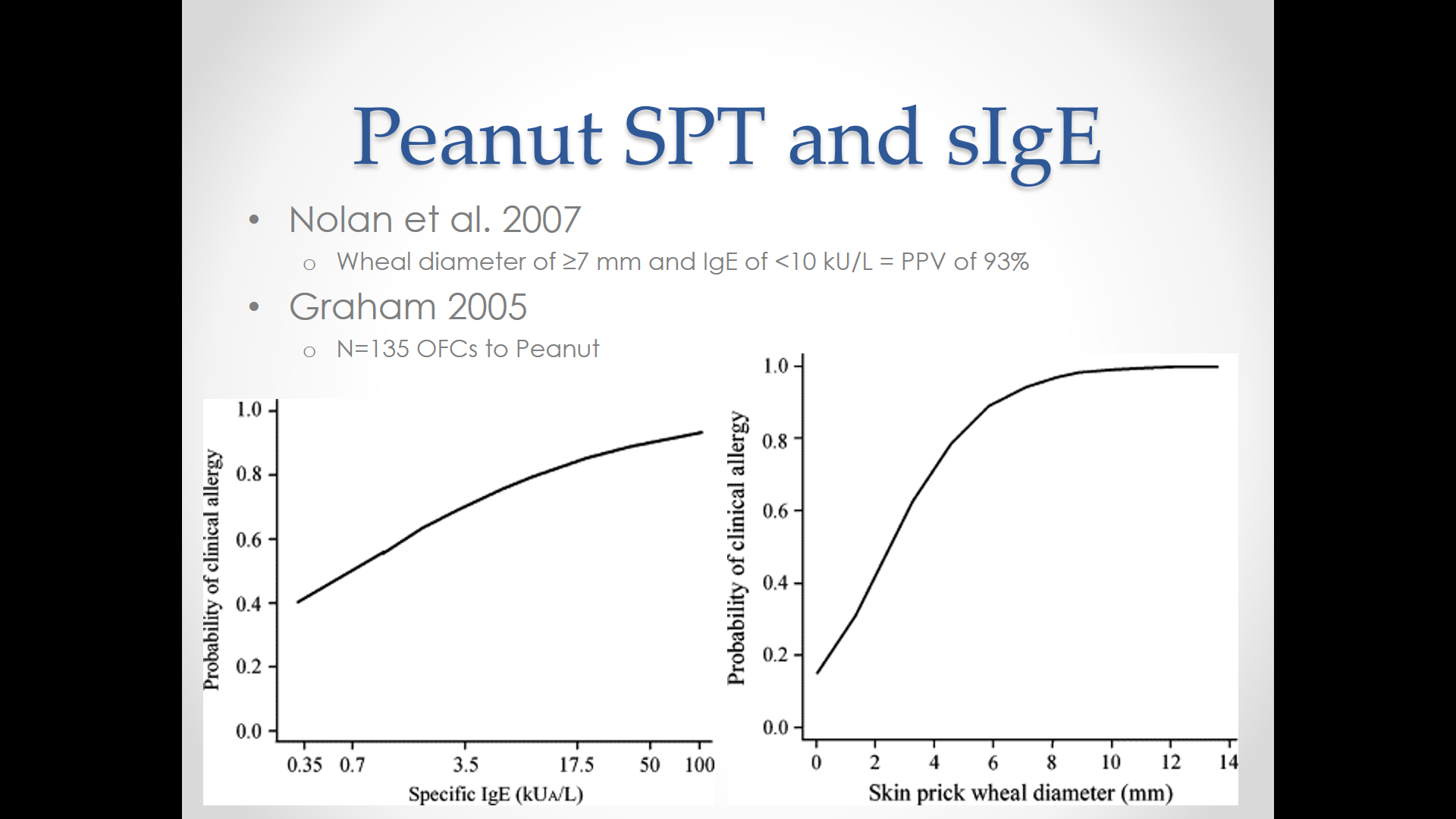
The next slide discusses potential evaluation. While the slide states that the positive predictive value of skin prick tests and serum-based IgE tests may be as high as 50%; in fact, when broad panels of allergy tests are ordered, the positive predictive value can be quite low.
Related blog posts:
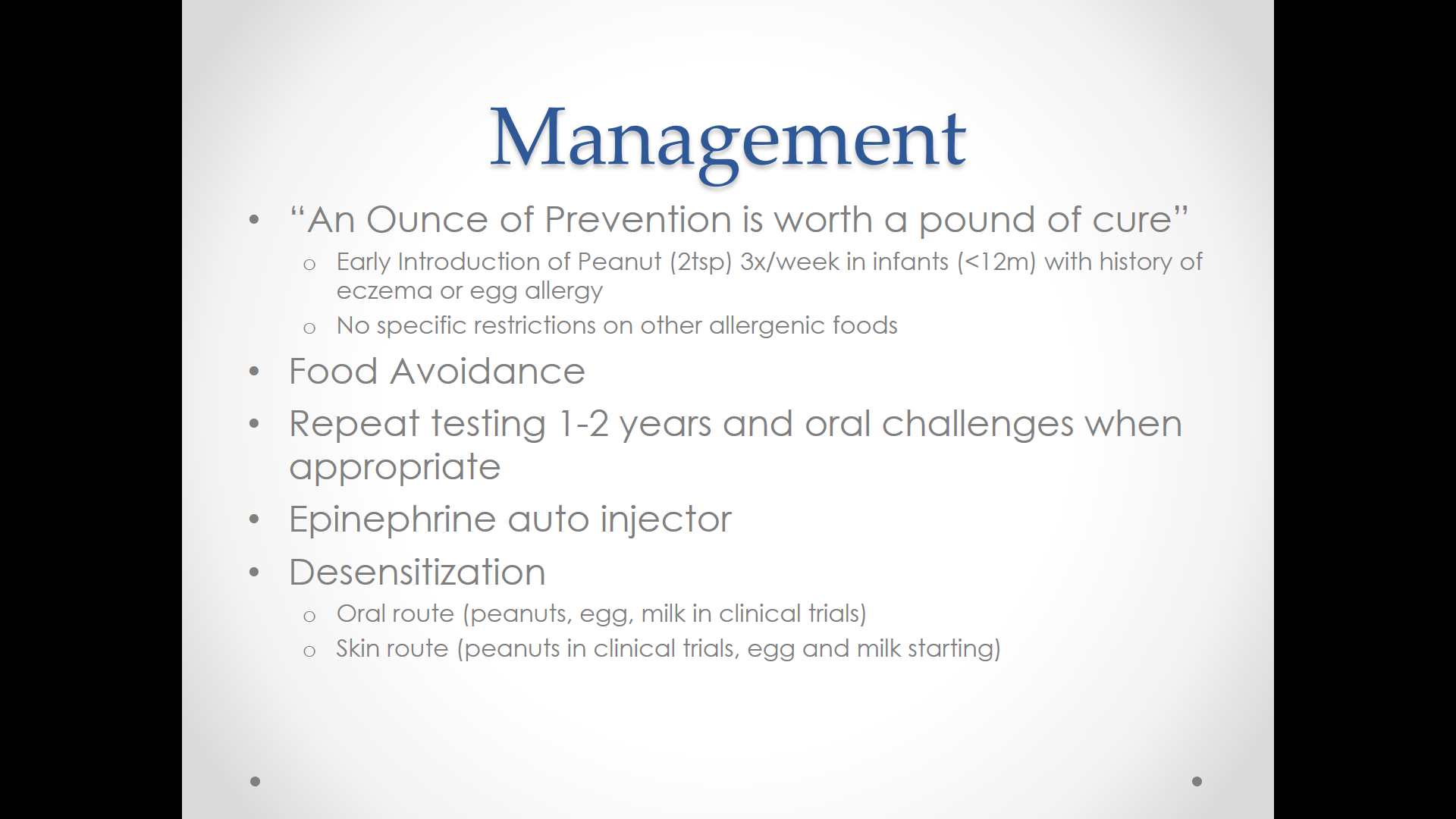
Dr. Patel did discuss the LEAP study and the LEAP-ON study which overall indicate that early antigen introduction is likely to reduce food allergies. Related blog posts:
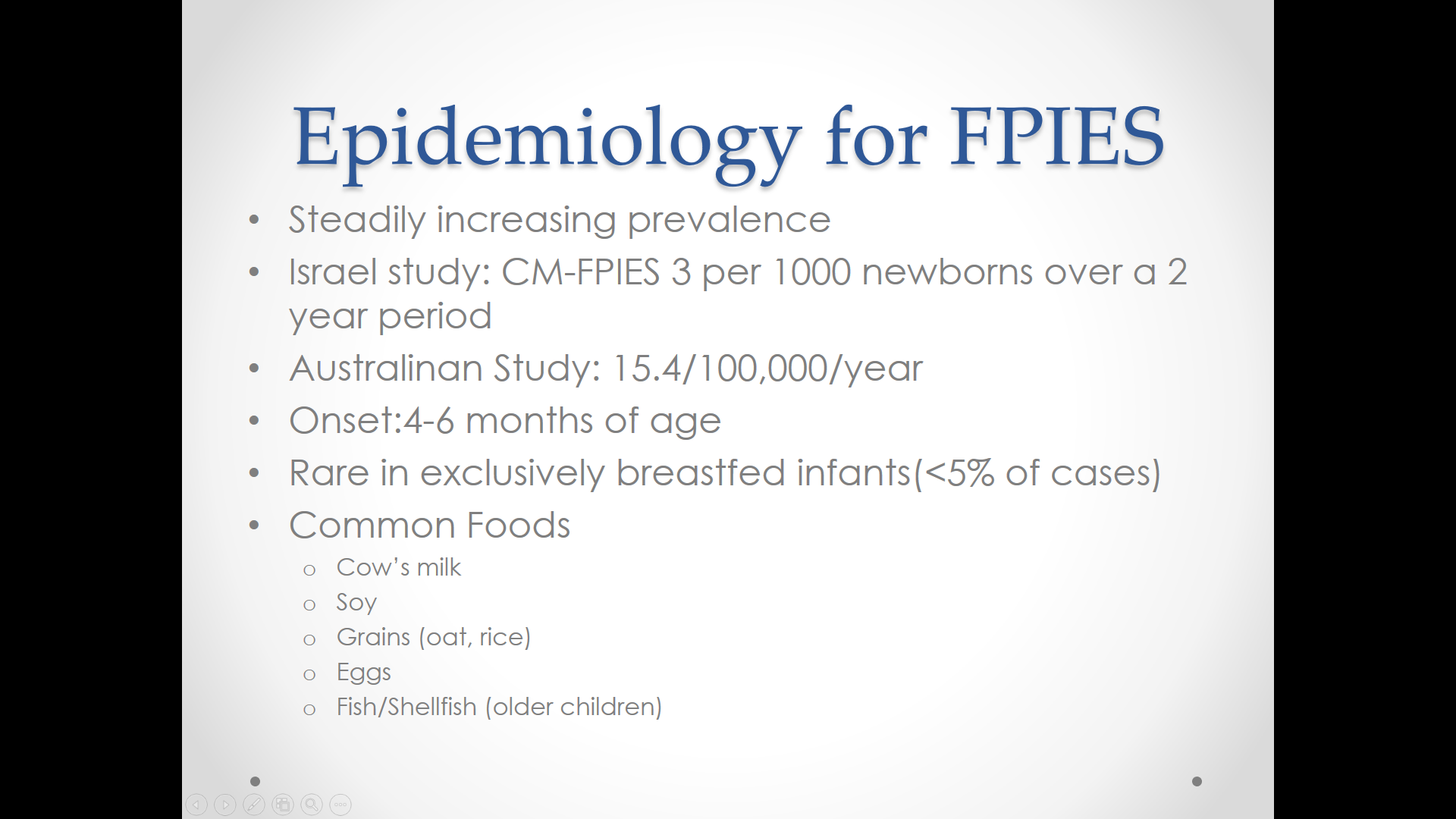
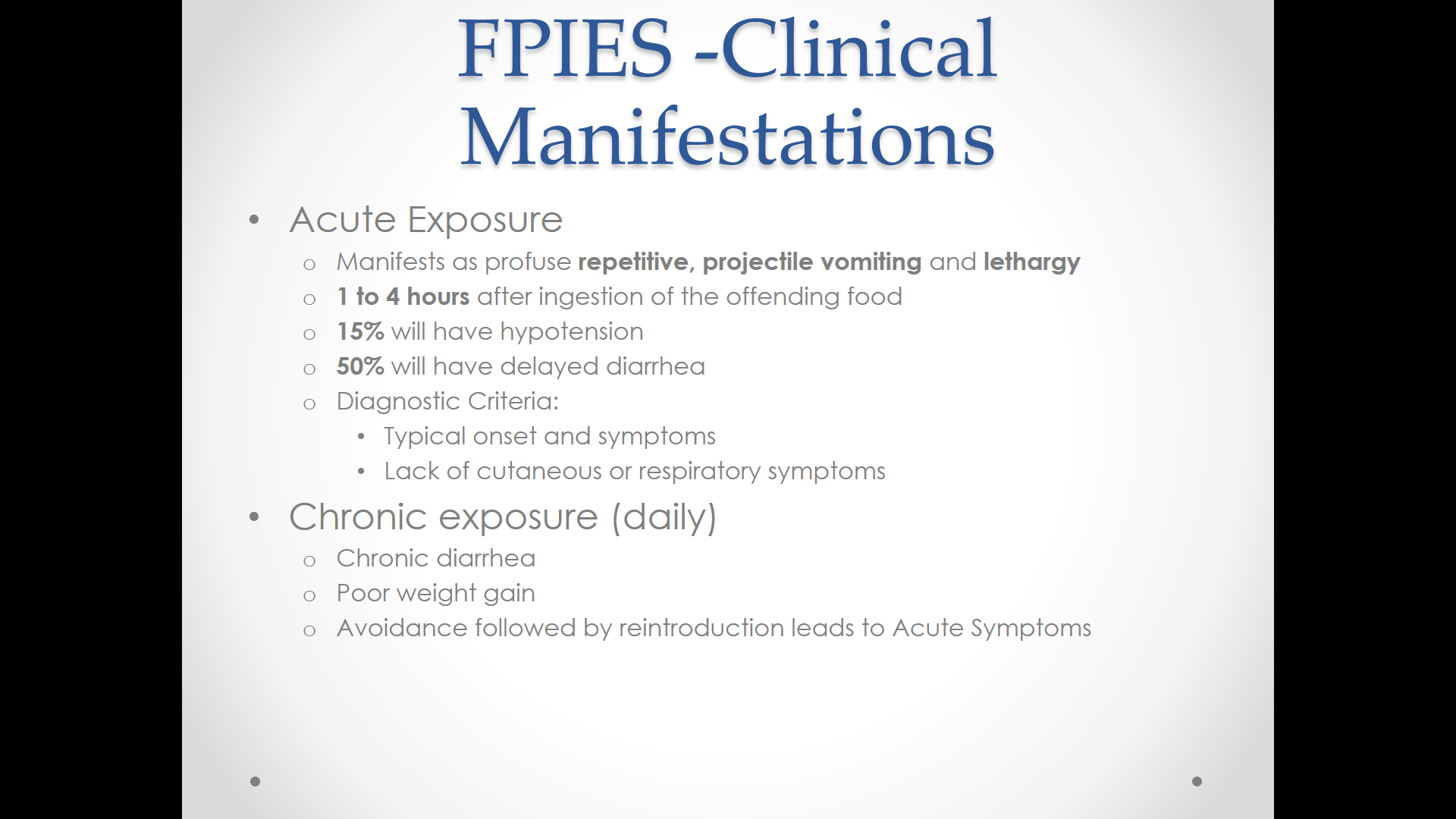
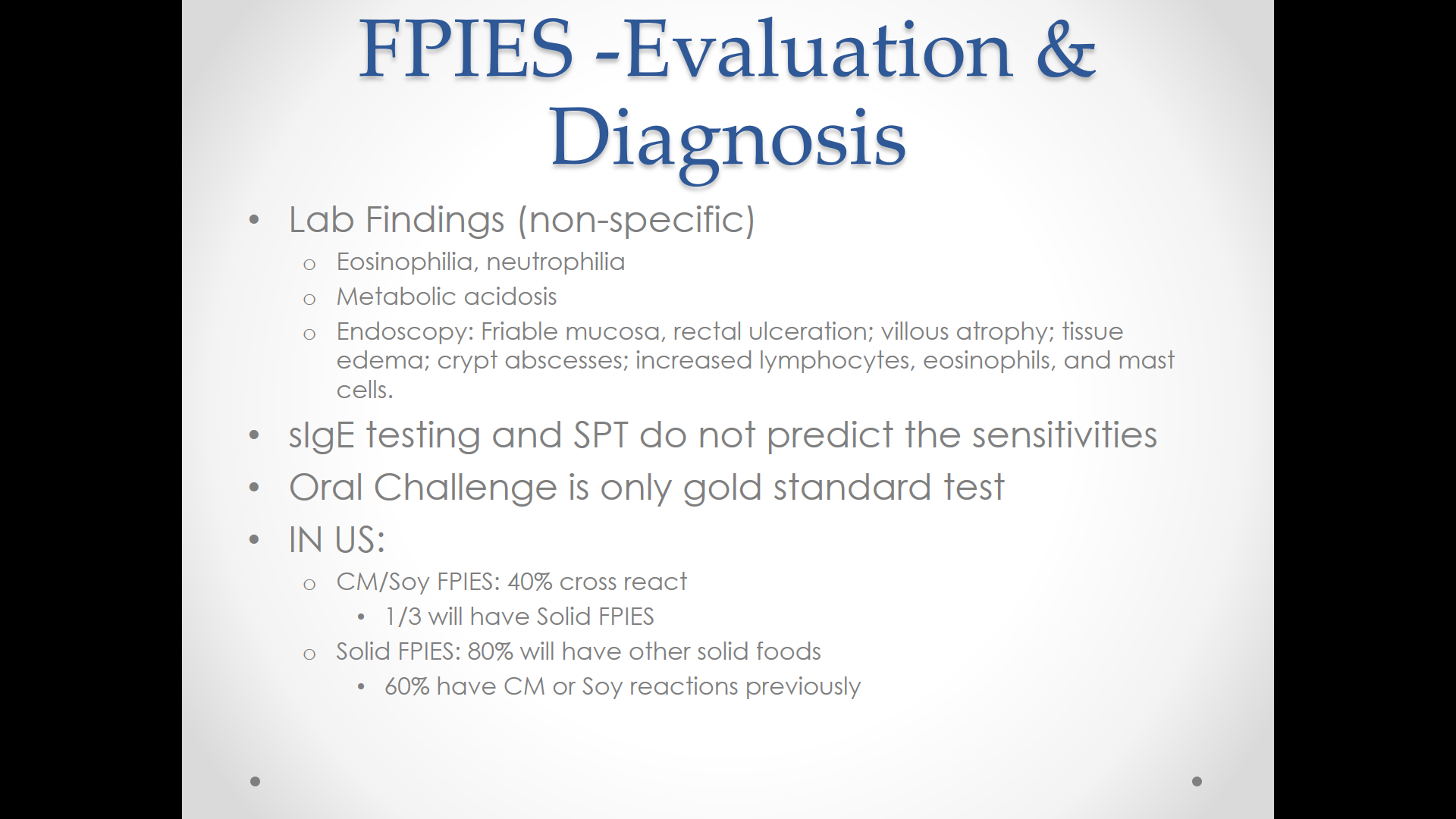
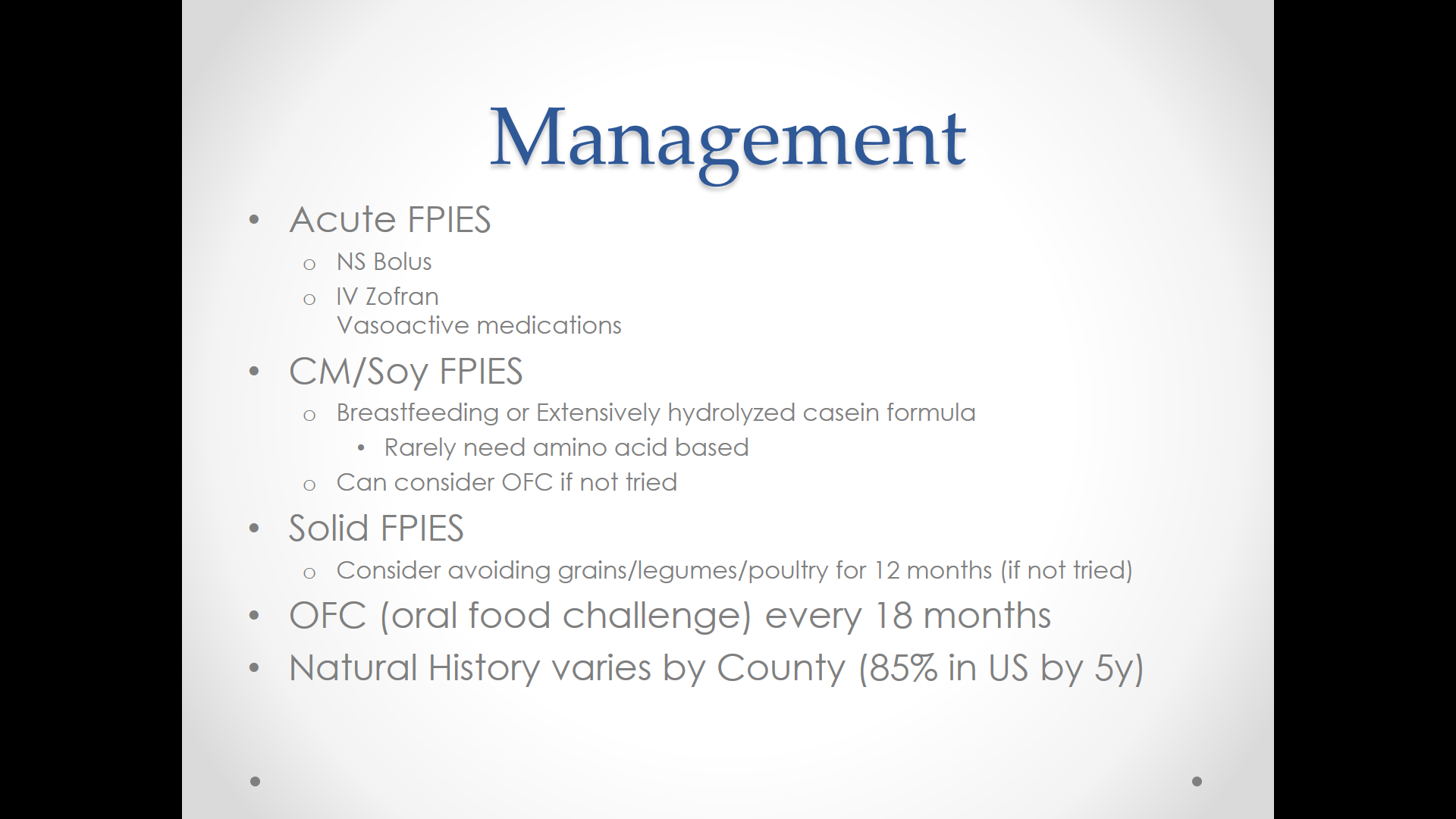
The next few slides review Food Protein-Induced Enterocolitis Syndrome. Related blog posts:
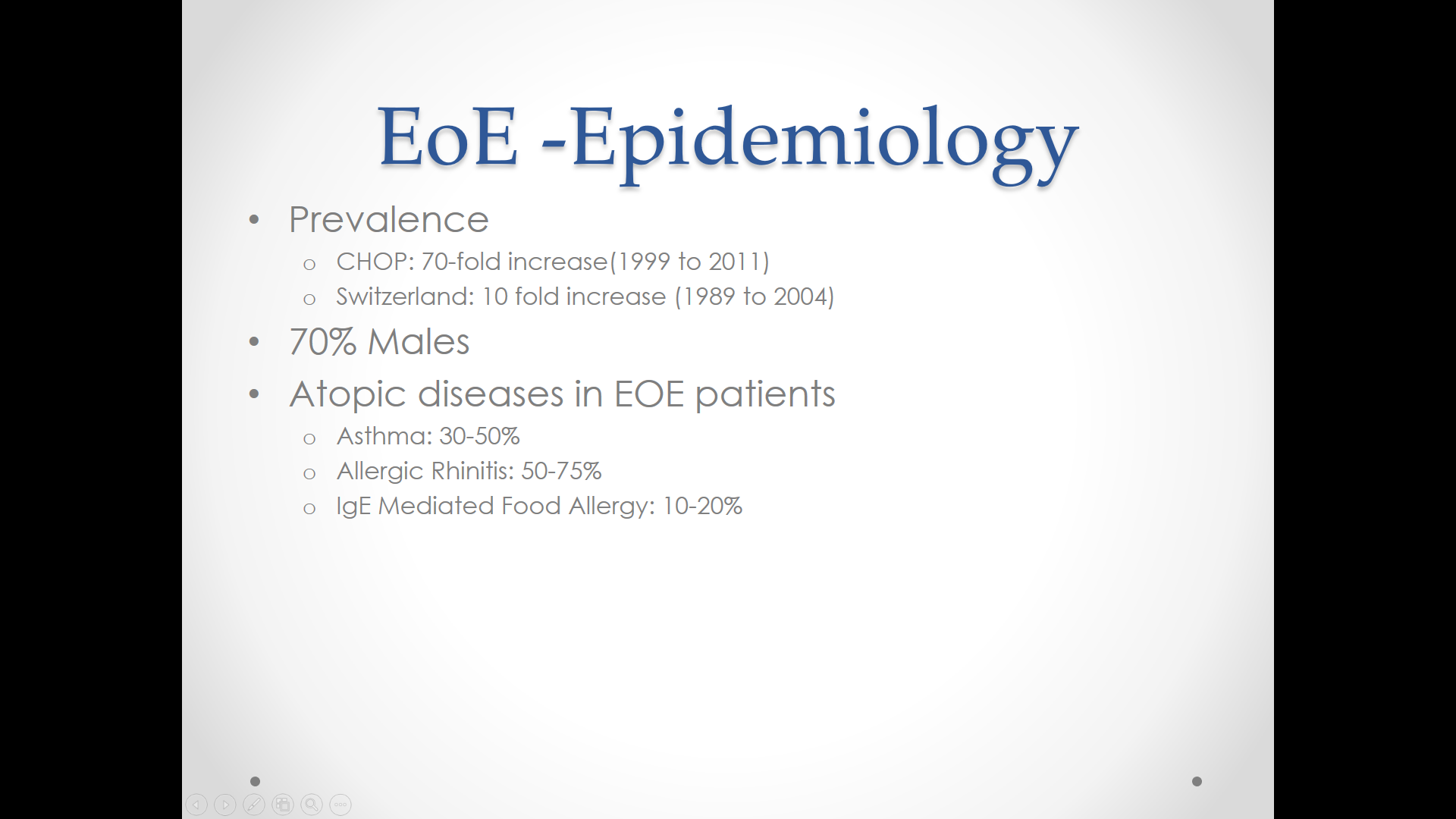
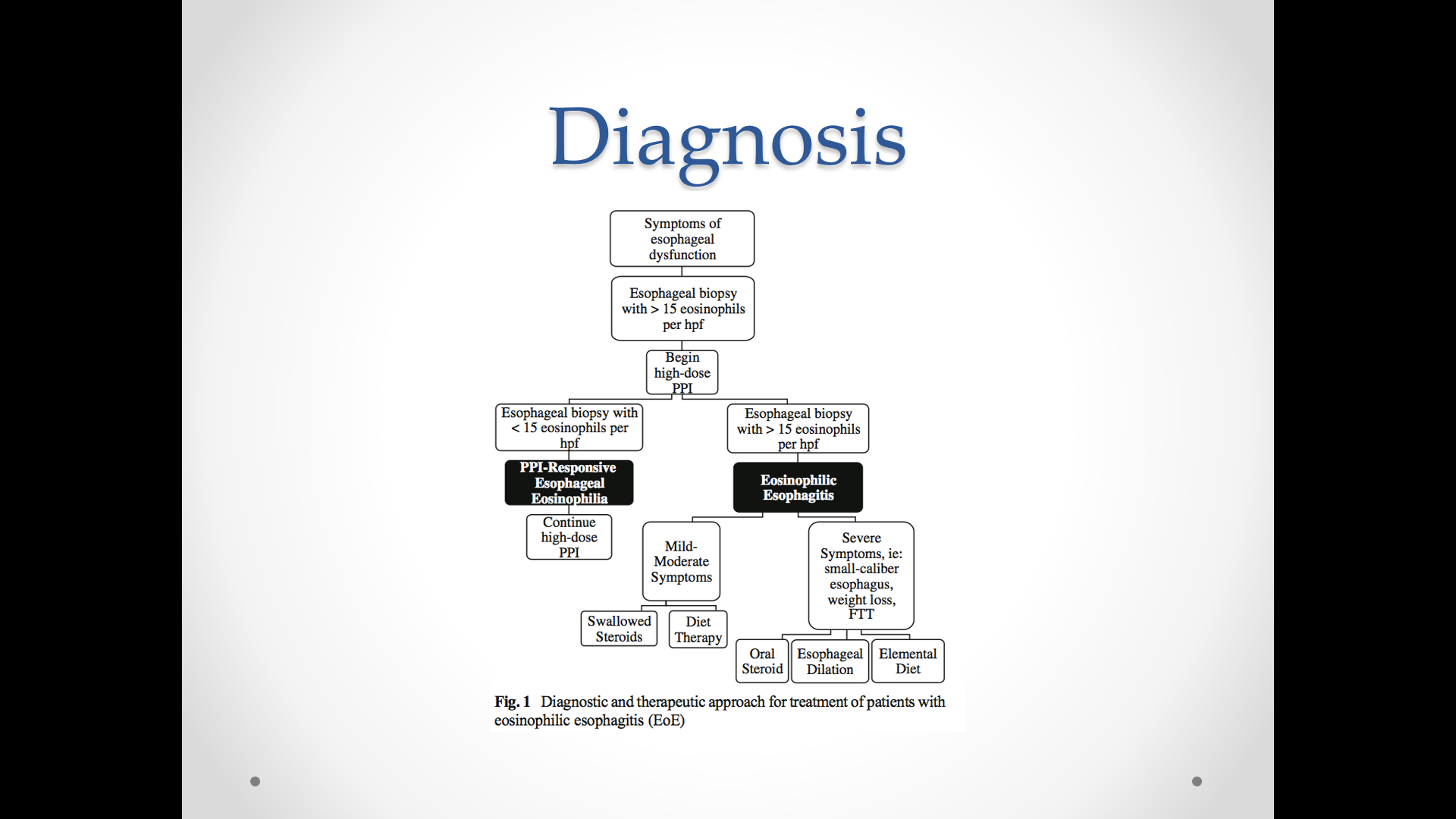
The next few slides discuss eosinophilic esophagitis (EoE). Allergy testing has not been very helpful in most patients with EoE. Related blog posts:
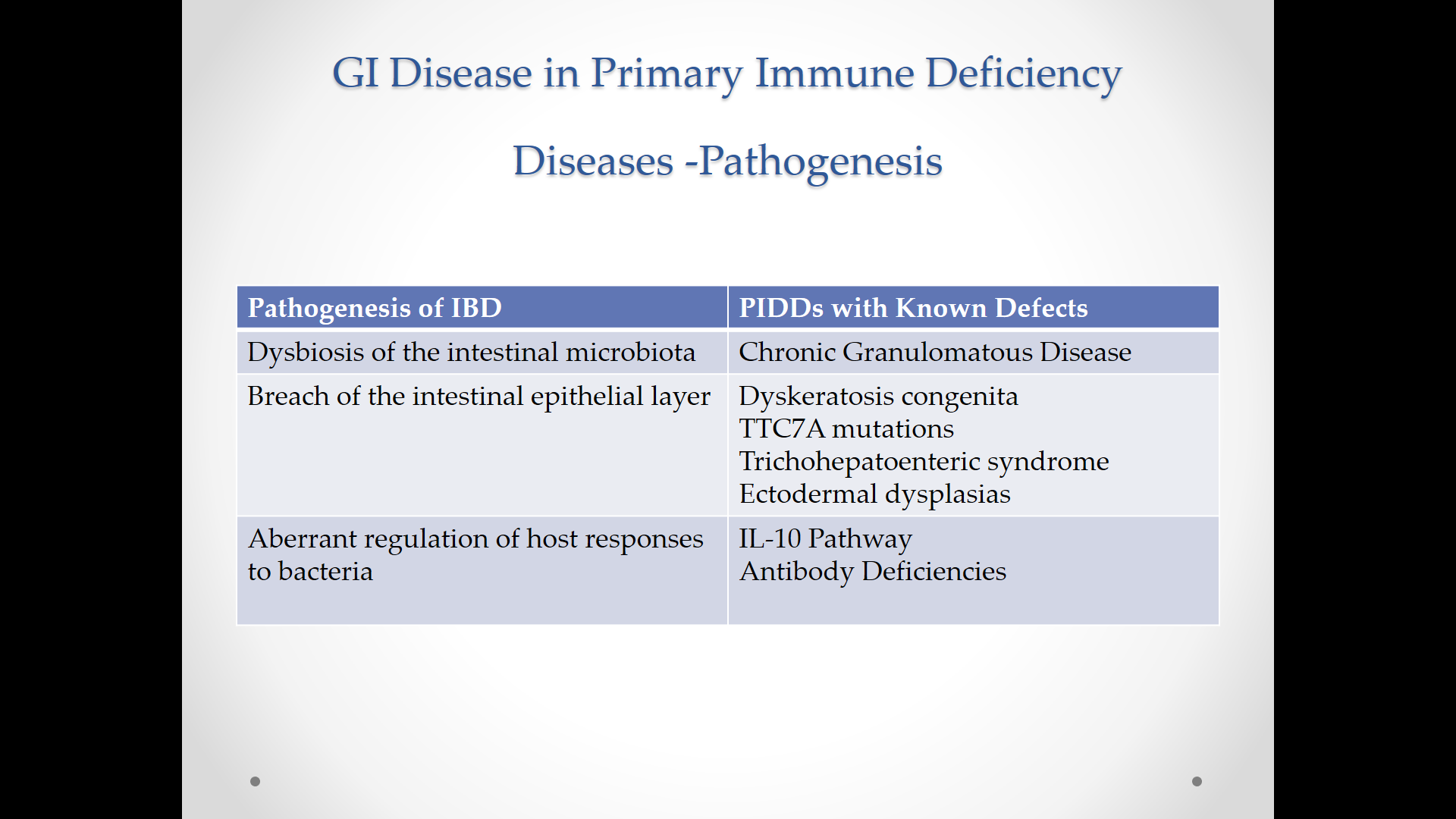
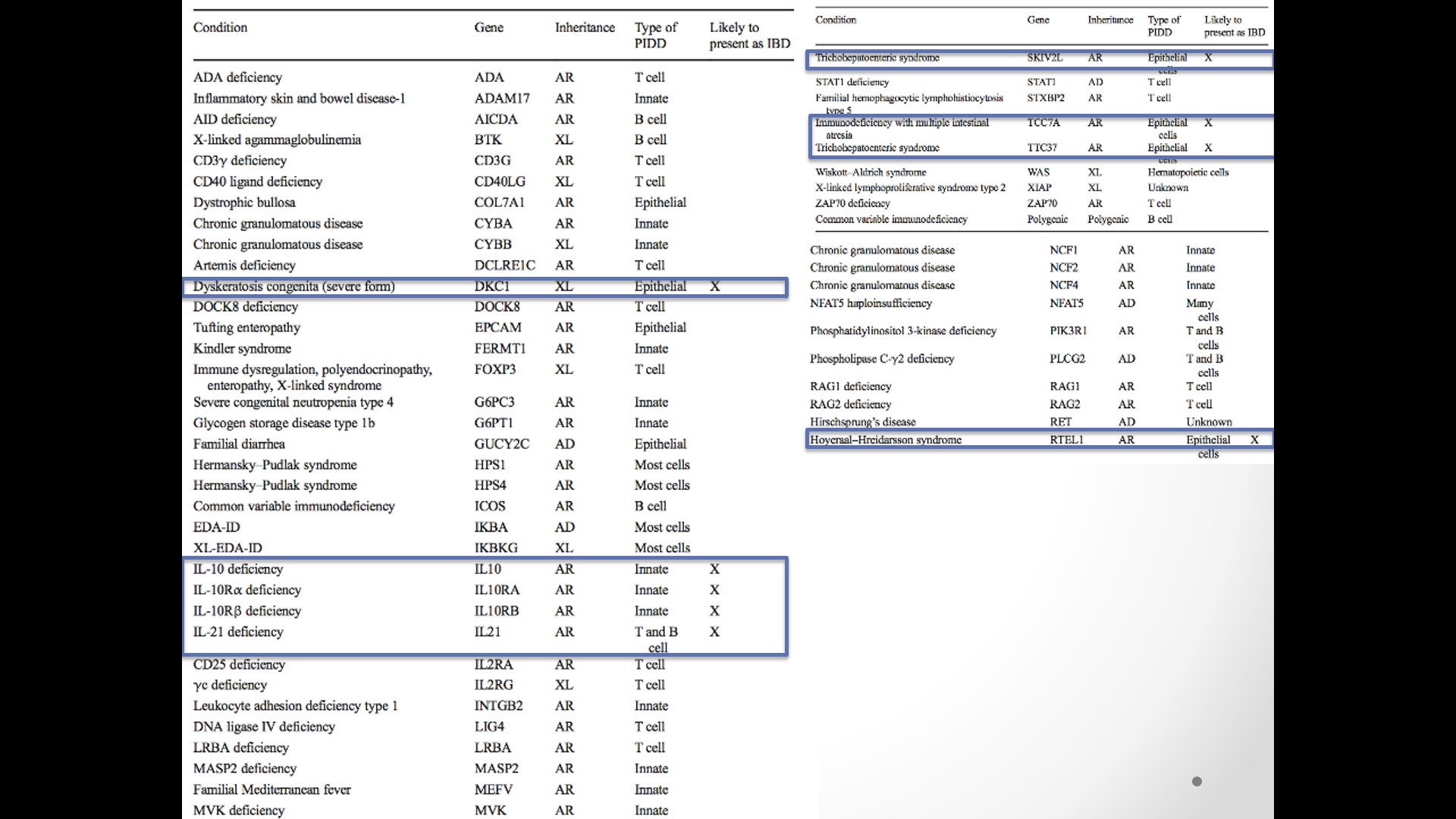
The last part of Dr. Patel’s talk focused on GI disease (eg. inflammatory bowel disease presentation) of primary immune deficiencies. In the bottom slide, the diseases that often present with GI symptoms are boxed.
Disclaimer: These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) and changes in diet should be confirmed by prescribing physician. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
In July, this blog reviewed a recent big study of primary sclerosing cholangitis (PSC) in adults with more than 7000 patients. A recent study in the pediatric age group enrolled 781 children from 36 institutions: MR Deneau et al. Hepatology 2017; 66: 518-27 (Congratulations to Nitika Gupta and Miriam Vos -in-town colleagues and contributing authors to this study.)
This retrospective study’s key findings:
The discussion notes that while pediatric PSC is a progressive disease, complications were slower to develop compared with adult-onset PSC. 10-year survival with native liver is typically lower in adults ~60% (vs 70% in this study). “Up to one third of adults with PSC may have esophageal varices within a year of diagnosis” compared with only 13% in this cohort. Dominant strictures are more common in adults, occurring in the majority within 5 years whereas this occurred in 16% of this cohort.
With regard to CCA, the authors note that current recommendations suggest starting to screen for CCA in patients over age 18 years with ultrasound and CA 19-9 at 6-12 month intervals. These studies “could reasonably be extended to PSC patients aged 15 and above and [for those requiring dilatation] of biliary strictures.”
My take: This large pediatric PSC study provides more clarity on the outcomes of patient’s with PSC and the associated conditions.
Related blog posts:

Steps at the High Museum
A recent retrospective study (PC Hopkins, N Yazigi, CM Nylund. J Pediatr 2017; 187: 253-7) provides an update on the recent incidence of biliary atresia in the US from 1997-2012. This study relied on coding for biliary atresia or Kasai hepatoportoenterostomy to identify cases using HCUP-KID database. This database provides a nationally representative sample of pediatric hospitalizations and captures ~96% of pediatric hospitalizations in the US.
Key findings:
My take: In my view, at this time, obtaining a blood test for direct bilirubin in the first two weeks of life will need to be adopted broadly if we are going to diagnose biliary atresia at an earlier age.
Related blog posts:

Dry Falls, Highlands NC

Dry Falls, Highlands NC
This retrospective study of 487 pediatric patients shows that it takes a long time to normalize celiac serology/anti-tissue transglutaminase antibody (TTG). The median time was 407 days for the 80.5% of patients that normalized their serology in the study time frame. The time was 364 days for those who were considered adherent to a gluten-free diet. Patients with type 1 diabetes were less likely to normalize their TTG levels. Faster normalization occurred in those with lower titers at baseline.
Related blog posts:
In this chart review, among 135 children, normal ESR and CRP were observed in 28% of children with Crohn disease and 42% of children with ulcerative colitis.
Related blog post: Do you really need both a ESR and CRP?
This guideline paper details 31 recommendations (some with multiple parts) for the evaluation and management of children with neurologic impairment. The recommendations include detailed evaluations including knee heights, skinfold thickness measures, DXA scan, routine micronutrient bloodwork, along with a low threshold for oropharyngeal dysphagia assessment. The paper has recommendations for evaluations of reflux, constipation, and dental problems. The authors suggest “considering use of enteral feeding if total oral feeding time exceeds 3 hours per day.”
Related blog post: Surgery for reflux works best for those who need it the least
A recent case report (V Cardenas et al. J Pediatr 2017; 186: 179-82) describes recurrent acute liver failure (ALF) in the setting of neuroblastoma amplified sequence deficiency (NBAS).
The case report describes a 2 yo who developed very elevated aminotransferases (ALT >14,000), hypoglycemia, severe coagulopathy (INR 4.5)), lactic acidosis (6.5 mmol/L) and hyperammonemia (282 μmol/L) following a febrile illness.
Genetic testing uncovered 2 variants in the NBAS gene consistent with NBAS deficiency.
Key points:
My take: NBAS deficiency, along with hemophagocytic lymphohistiocytosis (HLH), infections, and Kawasaki’s disease, needs to be considered in children with severe liver dysfunction associated with fevers.

A few years ago I saw a patient with a similar rash (BF Curtis et al. Gastroenterol 2017; 153: 355-6) and texted a picture to a dermatology colleague who quickly asked me whether my patient was using heating packs/heating pads on her abdomen.
This rash, termed, “erythema ab igne,” develops due to excessive heat exposure. Also, it has been called “toasted skin syndrome.” Over time, if heat is not continued to abdomen, in most cases, the skin reverts to normal in this benign asymptomatic condition.

A recent study (M Kasahara et al. Liver Transplantation 2017; 23: 1051-7, editorial 977-8) indicates improvement in survival among the smallest liver transplant patients. In this study of 12 patients less than 3 months of age, the cumulative 10-year patient and graft survival for both was 90.9%.
These patients received living donor liver transplantation. Living donors likely contributed to the excellent outcomes both in terms of enhancing the timing of transplantation and also with regard to size. Whole organs are not likely to fit well in these small abdomens. The size of the patients ranged from 2.8 kg (at 29 days) to 5.5 kg). 11 of 12 had fulminant hepatic failure with 6 of these cases being considered unknown etiology.
Limitation: This was a very small sample size.

A recent review (S Chang, B Shen, F Remzi. Gastroenterology & Hepatology 2017; 13: 466-75 Full text link: When Not to Pouch: Important Considerations for Patient Selection for Ileal Pouch-Anal Anastomosis) makes recommendations regarding Ileal pouch-anal anastomosis (IPAA) for Crohn’s disease and indeterminate colitis. Key points:
This review also discusses IPAA and other issues including obesity (which increases the likelihood of complications), sphincter dysfunction, elderly patients, and radiation therapy.
Of note, recent ESPGHAN IBD Porto Group guideline for surgical Crohn’s disease management in children (J Amil-Dias et al JPGN 2017; 64: 818-35) at first glance seems to be at odds with Chang et al recommendations:
To me, statement 8 should have been worded to include “except in limited circumstances.” As it stands now, it misleads those who do not carefully review the entire report.
My take: The report by Chang et al makes a strong case for its conclusion: “Although it is true that the diagnosis of CD is a potential contraindication to IPAA, patients with isolated Crohn’s colitis may thrive after pouch surgery. At this time, patients with isolated Crohn’s colitis (without perianal disease or small bowel involvement) have good pouch retention rates.” Their review prompted me to look more closely at the ESPGHAN IBD Porto Group guideline; their Statement 8 recommendation is, in fact, quite misleading.
Disclaimer: These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.

Keyhole view , looking into the Rotunda UVa, of Thomas Jefferson (or TJ for those in the know)

