A terrific 12 page review of irritable bowel syndrome (IBS): AC Ford, BE Lacy, NJ Talley. NEJM 2017; 376: 2566-78.
Diagnosis of Irritable Bowel:
Testing: National guidelines recommend that for a patient who meets Rome IV criteria, “the physician should make a positive diagnosis of IBS without resorting to a battery of tests.” Nevertheless, many physicians obtain some workup. If a workup is undertaken, the authors state “consider limited testing (CBC, CRP level, celiac serological test, fecal calprotectin level)”
Rome IV criteria of IBS are reviewed in Table 1 and includes warning signs. Summary of Rome IV critieria from emedicine website on Irritable Bowel Syndrome: The Rome IV criteria for the diagnosis of irritable bowel syndrome require that patients have had recurrent abdominal pain on average at least 1 day per week during the previous 3 months that is associated with 2 or more of the following [2]:
-
Related to defecation (may be increased or unchanged by defecation)
-
Associated with a change in stool frequency
-
Associated with a change in stool form or appearance
The Rome IV criteria (May 2016) only require abdominal pain in defining this condition; “discomfort” is no longer a requirement owing to its nonspecificity, and the recurrent abdominal pain.
Supporting symptoms include the following:
Four bowel patterns may be seen with irritable bowel syndrome, and these remain in the Rome IV classification. These patterns include the following:
-
IBS-D (diarrhea predominant)
-
IBS-C (constipation predominant)
-
IBS-M (mixed diarrhea and constipation)
-
IBS-U (unclassified; the symptoms cannot be categorized into one of the above three subtypes)
Symptoms not consistent with irritable bowel syndrome should alert the clinician to the possibility of an organic pathology. Inconsistent symptoms include the following:
The authors provide a diagnostic algorithm which is straight-forward. The caption includes “tenderness is not increased by tensing abdominal wall muscles.” The inclusion of Carnett’s sign is a useful reminder to consider/exclude muscle wall etiologies.
Another important point is that bile-acid diarrhea occurs in a significant fraction of adults with the diarrhea subtype of IBS, more than 25% of cases in a meta-analysis; thus, a therapeutic trial of a bile acid sequestrant may be useful.
Pathophysiology:
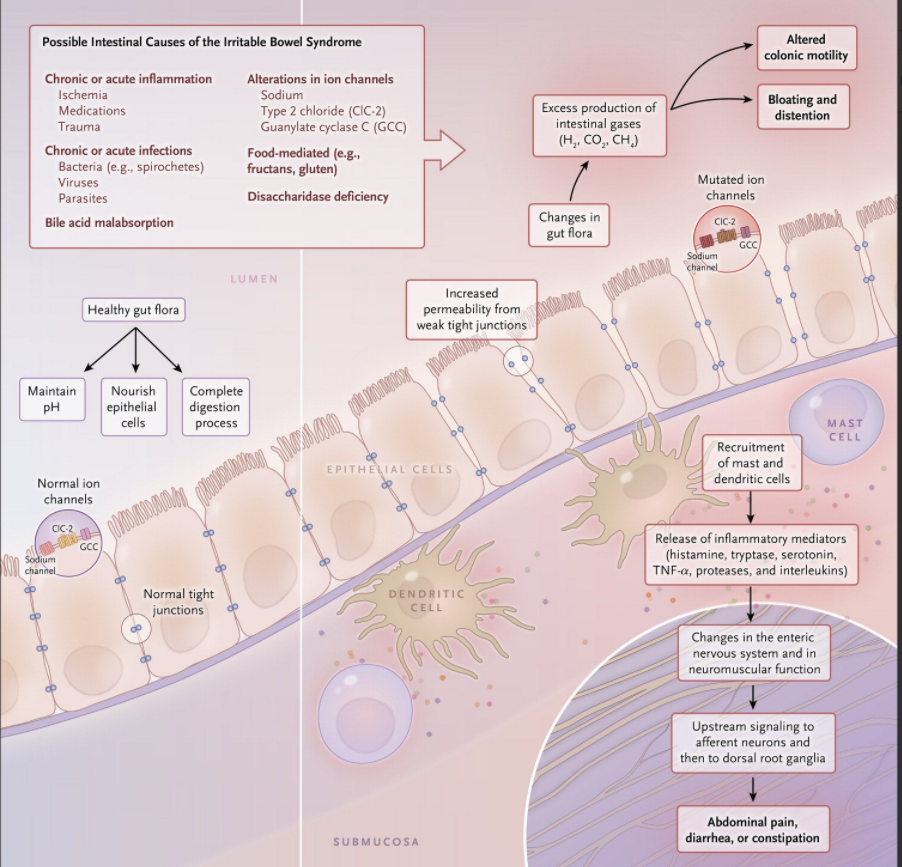
There are likely multiple pathways leading to IBS. In fact, Figure 2 lays out a Brain-Gut pathway as well as a Gut-Brain pathway. In the former, genetic predisposition and environmental factors/CNS alterations, could make one more susceptible to IBS after localized GI inflammation. In the later, changes in the GI tract induced by infection, inflammation, food antigens, and medications which could alter intestinal permeability and/or microbiome could result in changes in CNS function (eg. new-onset anxiety, depression or somatization). It is well-recognized that after gastrointestinal infections (bacterial, protozoal, viral), “IBS-type symptoms persist in 10 to 20% of infected patients.”

Image from NEJM twitter feed. It is noted that not all pathophysiological processes shown occur in all patients with IBS or in all IBS subtypes.