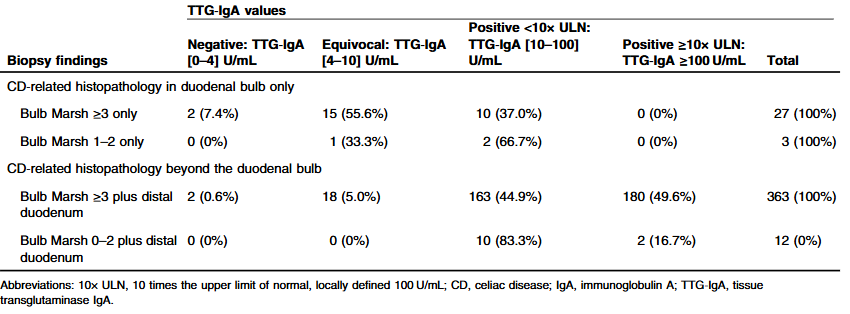
Methods: There were 405 cases included in this retrospective study (mean age = 9.6 years). TTG-IgA values were considered negative if <4 U/mL, equivocal between 4 and 10 U/mL inclusively, and positive if >10 U/mL. At the authors’ institution, TTG‐IgA ≥10× ULN corresponds to ≥100 U/mL.
Key findings:
Bulb-restricted CD was present in 7.4% of cases
TTG-IgA was negative or equivocal in 60.0% of bulb-restricted CD, compared to 5.3% of distal duodenal CD (odds ratio [OR] = 26.6
No bulb-restricted CD cases attained TTG-IgA ≥10× ULN, compared to 48.5% of distal duodenal CD
My take: This study confirms and quantitates what most clinicians have experienced. Isolated duodenal bulb pathology is associated with lower celiac titer abnormalities.
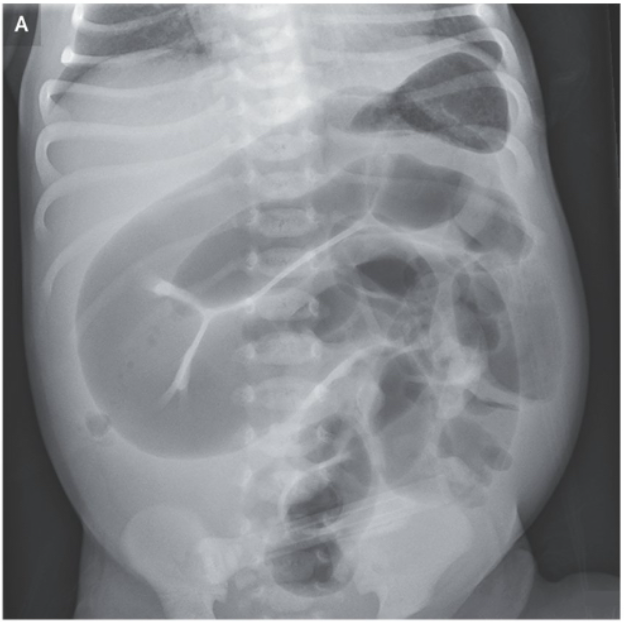
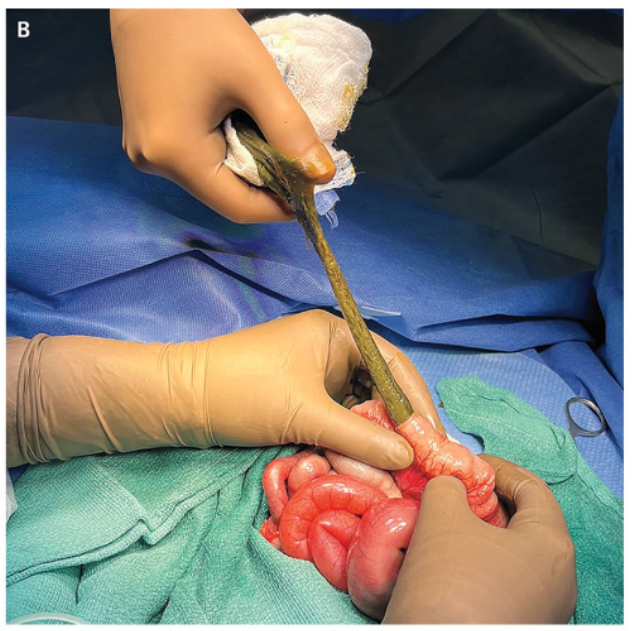
A Le-Nguyen. N Engl J Med 2025;392:1215. Meconium Ileus
An abdominal radiograph had shown dilated loops of small intestine (Panel A). Owing to concern for intestinal malrotation with midgut volvulus, an urgent laparotomy was performed. Considerable distention of the small bowel by thick meconium — rather than midgut volvulus — was identified. An enterotomy for evacuation of meconium was performed (Panel B). On postoperative genetic testing, the baby was found to be homozygous for a mutation in CFTR, the gene encoding cystic fibrosis transmembrane conductance regulator… The condition is associated with a very high risk of cystic fibrosis, so genetic testing is warranted in all cases. Uncomplicated cases are typically managed with serial enemas.
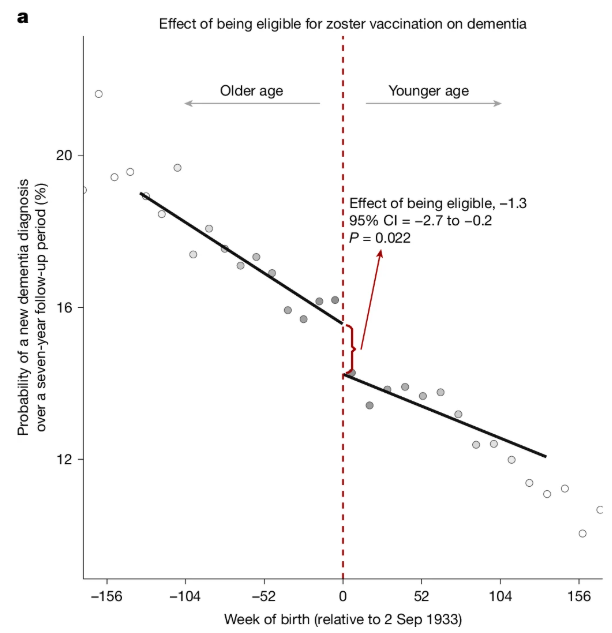
It’s been shown that reactivation of the chickenpox virus can lead to the accumulation of aberrant proteins associated with Alzheimer’s…
The new research, published Wednesday in Nature, analyzed data from more than 280,000 older adults in Wales and found that people who received the original shingles live virus vaccine were 20% less likely to develop dementia of any type than those who were not vaccinated...
The new study was possible because of an unusual public health policy in Wales that provided a “natural experiment” to explore the potential impact of the vaccine on dementia risk. With the rollout of the vaccine on Sept. 1, 2013, in Wales, shots were offered to people who were 79 on that date but not given to people who had turned 80.That allowed the German and Stanford University researchers to compare two groups of people with similar health characteristics who differed only by one week in age...
Bolstering the case for the shingles vaccine protecting against dementia were the findings from a study published in Nature Medicine in 2024 that analyzed medical records from more than 100,000 patients. That analysis suggested the newer shingles vaccine was associated with even better protection against dementia.
Two recent commentaries discuss some of the problems for aspiring physicians:
RP Walensky, LD Walensky. NEJM 2025; 392: 1251-1254. Application Overload — A Call to Reduce the Burden of Applying to Medical School
DB Holt, EA Elster. NEJM 2025; 392: 1249-1251. Rethinking Shadowing for Aspiring Physicians
In the first article, the authors detail the burden associated with the common-place high-volume applications to medical schools.
“The cost is approximately $150 per school for application fees, plus $345 for taking the MCAT and having the score distributed through AMCAS. These fees are waived for qualifying low-income applicants (as primarily defined by household income below 400% of the national poverty level) who apply to the AAMC Fee Assistance Program and provide the required financial documentation.2 After submitting the primary application, applicants face a flood of secondary applications, some requiring up to eight additional essays. Even when the essay prompts are similar to those from other schools, the instructions often specify different lengths. One premedical student posted on social media the findings of his review of 54 medical schools’ secondary applications: he identified 222 different prompts, which he provided to help applicants get a jumpstart on their frenzied essay writing.3..
Between 2013 and 2023, … the total number of applications and the average number of applications per student increased dramatically — by 40% (from 690,281 to 966,947) and 28% (from 14.4 to 18.4), respectively. Despite the disproportionate escalation in applications submitted, the success rate (matriculants divided by applicants) remained flat (range, 36 to 44%).”
The authors recommend limiting applications to 10 to 12 medical school applications per applicant. This would benefit students as well as faculty burdens.
“The secondary-application process also needs to be reined in. Medical schools could adopt standardized secondary essays… Under this model, a student applying to 10 schools would complete a maximum of 13 secondary essays — 3 standardized and 1 customized essay per school — rather than the current norm of 60 to 80 essays (e.g., 20 secondary applications with 3 to 4 distinct essays each).”
My take: In Charlie and the Chocolate Factory, there are only five golden tickets. If everyone buys twice as many Wonka bars, it is a lot more expensive and perhaps more time-consuming. For medical school applicants, applying to 20 or more programs does not help if almost everyone is doing this. It does disadvantage the minority who do not have the financial means or available time to complete this arduous task.
In the second commentary, the article details the problems with shadowing experiences.
“Medical school admission in the United States remains intensely competitive. In 2024, according to the Association of American Medical Colleges (AAMC), prospective students submitted an average of 18 applications apiece…Many medical school admissions committees consider shadowing a physician to be an essential clinical experience for professional identity formation, so nearly all applicants now do some shadowing: 95% of respondents to the 2024 AAMC Matriculating Student Questionnaire (MSQ) said they’d spent time observing a physician at work.1…
Premedical students are spending more time shadowing — sometimes hundreds to thousands of hours, which often necessitate taking a “gap year” between college and medical school at a financial cost…Three quarters of medical school applicants report taking time off before medical school, 50% taking 1 to 2 years and 25% taking 3 or more years...
These additional years delay entry into the workforce and result in higher levels of debt than moving more quickly toward potential earnings as a physician; one lost year of a physician’s salary (an average of $265,000) would result in an estimated net loss of $2 million by retirement if the money were invested at a 7% return…
Although medical schools consider clinical experiences other than shadowing, a review of our own data suggests that applicants who have shadowed physicians for more than 50 hours are more likely than their peers to be admitted — and more likely to come from higher-income families.“
The authors point out that unstructured observation is of unclear benefit. A course from Stanford, that far fewer hours (11-20 hrs) was sufficient for more than 90% of students “to decide whether medicine was the right career for them….The current emphasis on shadowing not only contributes to a longer and more expensive medical education pathway but also discourages nontraditional applicants and pursuit of genuine interests in other areas that make for well-rounded physicians.”
My take: The pathway to medical school has become more time-consuming and expensive. At the same time, it is doubtful that lengthy shadowing experiences or extensive numbers of applications are benefiting aspiring students.
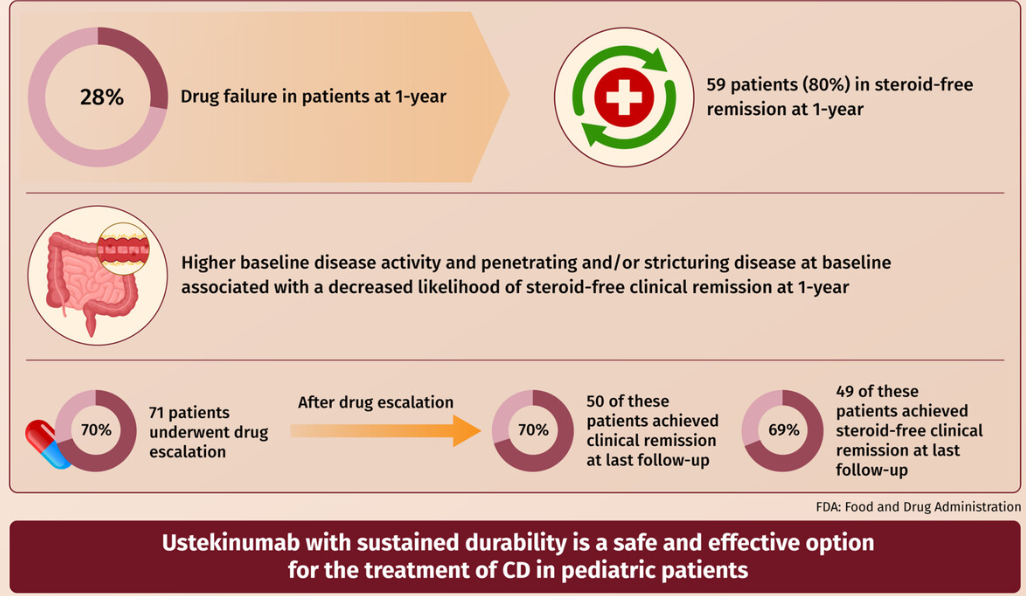
EB Mitchell et al. JPGN 2025;80:653–663. Ustekinumab is safe and effective in pediatric patients with Crohn’s disease
This was a retrospective longitudinal cohort study of 101 children with CD treated with ustekinumab from two large centers between 2015 and 2020. The median follow-up time on ustekinumab was 16.6 months.
Key findings:
Fifty-nine patients were in steroid-free clinical remission at 1 year.
Higher baseline disease activity (odds ratio [OR]: 0.91 (p = 0.01) and stricturing/penetrating disease phenotype (OR: 0.14 p = 0.02) were associated with decreased likelihood of steroid-free clinical remission at 1-year
Ustekinumab drug escalation occurred in 70% of patients, and after escalation, 50 (70%) achieved clinical remission, and 49 (69%) achieved steroid-free remission at the last follow-up
Adverse events were rare and did not require therapy discontinuation
My take: More pediatric data showing efficacy for ustekinumab is important. My sense, though, is that newer IL-23 specific agents are going to eclipse ustekinumab in pediatrics as they are doing in adults.
Z Gaibee et al. N Engl J Med 2025;392:1297-1309. The Genetic Architecture of Congenital Diarrhea and Enteropathy
Background:”Congenital diarrhea and enteropathies (CODEs) are a group of rare disorders that primarily affect the function of intestinal epithelial cells, leading to infantile-onset diarrhea and poor growth. Molecular defects in CODEs can be classified into six categories: epithelial trafficking and polarity, immune-cell-regulation, nutrient and electrolyte transport, enteroendocrine-cell development, nutrient metabolism, and other. CODEs are associated with substantial morbidity and mortality. Patients often receive lifelong fluid and nutritional management. Genetic causes include pathogenic variants in MYO5B (microvillus inclusion disease), EPCAM (tufting enteropathy), NEUROG3 (enteric anendocrinosis), DGAT1 (protein-losing enteropathy), and SLC9A3 (congenital sodium diarrhea). Treatment options are currently limited. However, an understanding of some of the genetic causes of CODEs has led to targeted therapies such as dietary treatments and the development of preclinical pharmacologic treatments.”
Methods: In this case series with 129 infants, the authors analyzed the exomes or genomes of infants with suspected monogenic congenital diarrheal disorders. Using cell and zebrafish models, we tested the effects of variants in newly implicated genes.
Key findings:
Causal genetic variants were identified in 62 infants (48%). This included a new founder NEUROG3 variant
Using cell and zebrafish models, the authors uncovered and functionally characterized three novel genes associated with CODEs: GRWD1, MYO1A, and MON1A
My take: Exome sequencing is an important part of the evaluation of infants with CODEs
Dr. Craig Friesen gave our group an excellent update on food allergy and disorders of brain-gut interaction (DGBIs). His main disclosure was that he is not an allergist. My notes below may contain errors in transcription and in omission. Along with my notes, I have included many of his slides.
Key points:
Food allergies are common affecting 6-10% of the population. In infants, milk and egg are common allergens. Nut allergies are more frequently seen in children
There are likely hundreds of genes that can predispose towards allergies
Food exposures, especially in the 4-6 month range, have been associated with a lower risk of food allergies
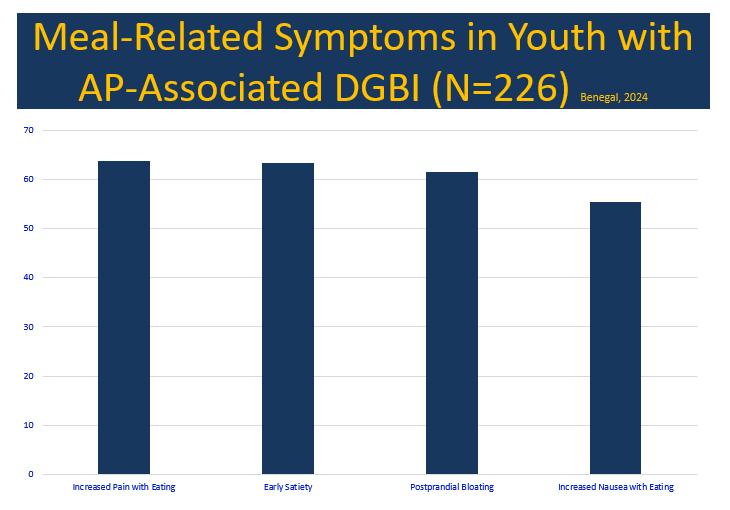
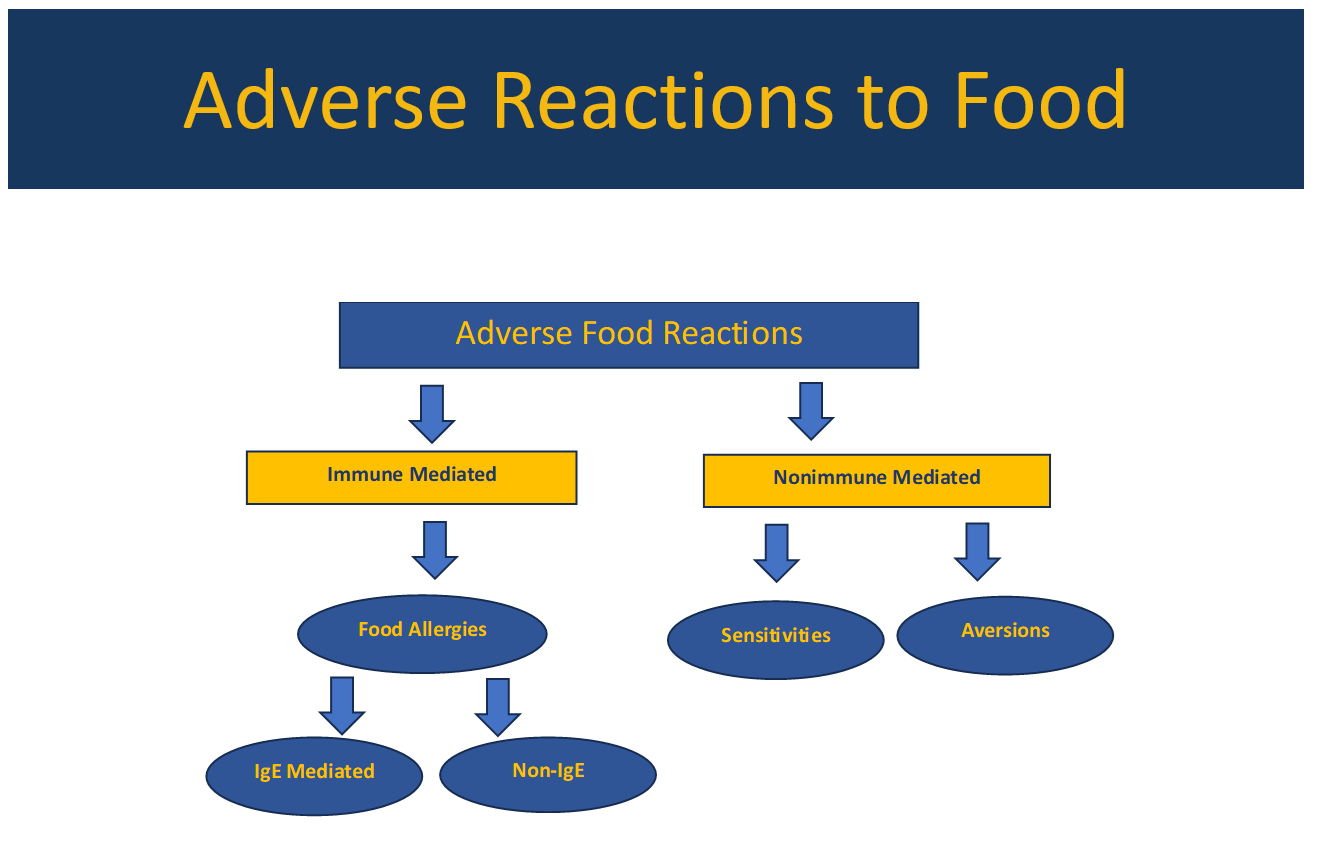
Food trigger symptoms are present in most patients with DGBIs; however, the lines between immune mechanisms and non-immune mechanisms are often blurry
Food allergy testing (skin prick testing, IgE-based blood tests) is not recommended in the absence of systemic symptoms due to poor specificity (perhaps ~10%). Obtaining a careful history is a very important part of determining allergies. Double-blind challenges, which are rarely done, are still considered “gold standard” for diagnosis
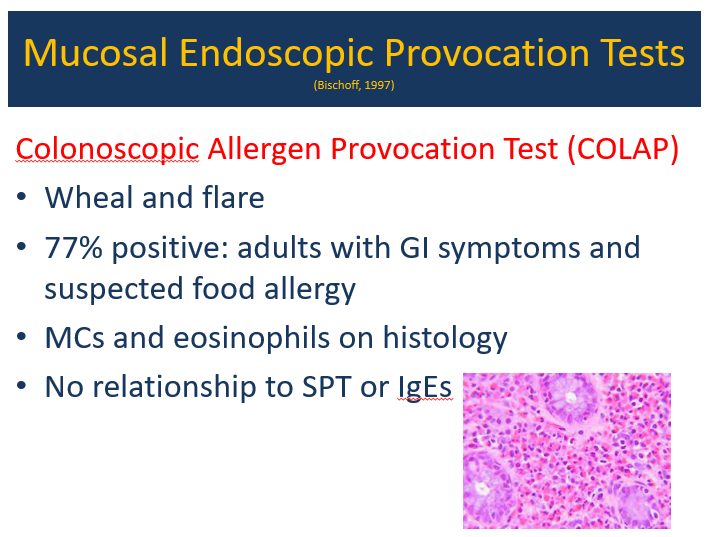
Mucosal endoscopic provocation (research tool) often discloses localized immune reaction; it does not correlate with skin prick testing or IgE-based blood tests
After prior sensitization/food allergies, stressful conditions may create similar symptoms as allergic exposures. This can be mediated by histamine and tryptase/mast cells
It is rare for food allergen restriction to “fix” a DGBI. Occasionally, food allergies may be part of the problem. Dietary restrictions may lead to weight loss and contribute to ARFID
IgG-based allergy testing (widely available) is not recommended; IgG antibodies are usually indicative of tolerance
Environmental pollen counts are associated with increased DGBI symptoms, increased mucosal eosinophils, and less sleep
Environmental allergen testing can sometimes be helpful in identifying cross-reacting foods
Alpha-gal syndrome. Consider testing in those with symptoms triggered by meat ingestion, and those with refractory symptoms. In pediatric patients, often no rash is identified and many will ‘outgrow’ allergy
Oral immunotherapy can be effective in improving tolerance for allergic foods; however, up to 70% will redevelop intolerance
When mucosal eosinophilia is identified, there are a number of potential treatments including dietary restrictions, mast cell stabilizers, antihistamines, and steroids
Is There a Way to Prove Which Dietary Factors Trigger IBS? RE: A Fritscher-Ravens et al. Gastroenterol 2019; 157: 109-18 –confocal laser endomicroscopy (CLE) for “real-time detection and quantification of changes in intestinal tissues” related to food challenges
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
Methods: Lifetime radiation-induced cancer incidence and 90% uncertainty limits (UL) were estimated by age, sex, and CT category using National Cancer Institute software based on the National Research Council’s Biological Effects of Ionizing Radiation VII (BEIR VII) models and projected to the US population using scaled examination counts.
Key findings:
Ninety-three million CT examinations were performed in 61 510 000 patients in the United States in 2023, including an estimated 3,069,000 CTs (3.3%) in 2,570,000 children (4.2%) and 89,931,000 CTs (96.7%) in 58,940,000 adults (95.8%)
In this risk model, the 93 million CT examinations performed in 62 million patients in 2023 were projected to result in approximately 103,000 future cancers
Estimated radiation-induced cancer risks were higher in children and adolescents, yet higher CT utilization in adults accounted for most (93,000) radiation-induced cancers
“If current practices persist, CT-associated cancer could eventually account for 5% of all new cancer diagnoses annually”
Discussion: “The projected number of radiation-induced cancers in this analysis is 3 to 4 times higher than the earlier assessment of CT exposure for several reasons”
CT use is 30% higher today than in 2007
Dose modeling in this study accounted for multiphase scanning
Substantially higher organ doses in this study were reconstructed using newer dosimetry methods
More granular CT categories reflecting imaging indications that have important dose differences
“Many of the model assumptions were conservative” and could underestimate the risk
My take (borrowed from authors): “Even very small cancer risks will lead to a significant number of future cancers given the tremendous volume of CT use in the United States…CT could be responsible for approximately 5% of cancers diagnosed each year. This would place CT on par with other significant risk factors, such as alcohol consumption (5.4%) and excess body weight (7.6%)”