S Machado et al. NEJM 2025;392:1310-1319. Association between Wealth and Mortality in the United States and Europe
Methods: This was a longitudinal, retrospective cohort study with 73,838 adults (mean [±SD] age, 65±9.8 years), a total of 13,802 (18.7%) died during a median follow-up of 10 years.
Key findings:
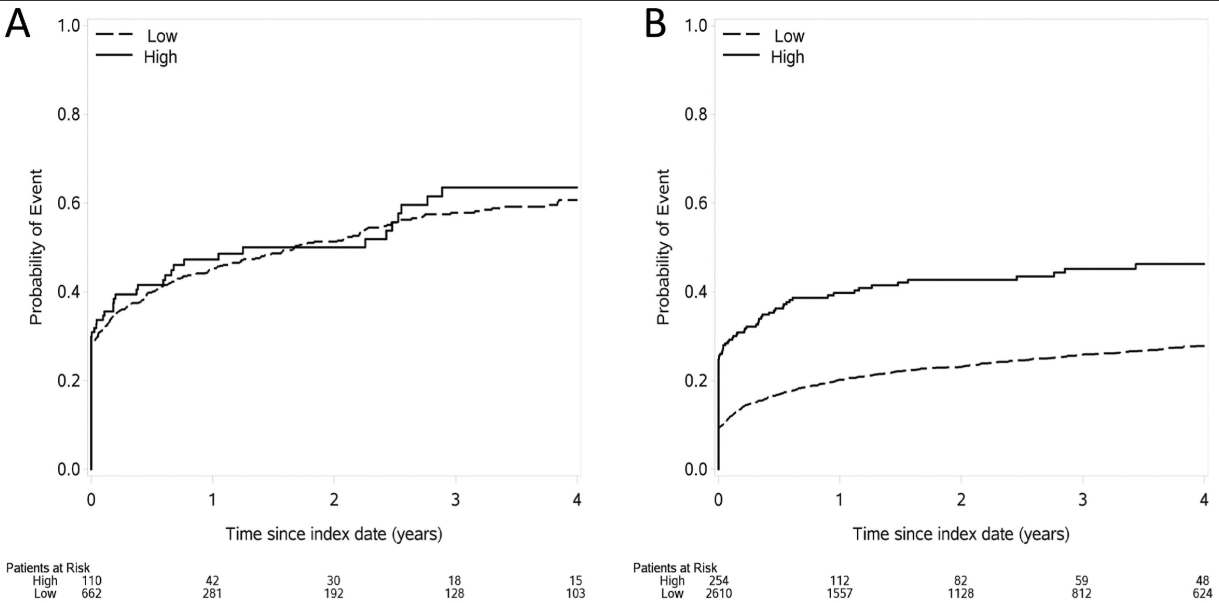
- The gap in survival between the top and bottom wealth quartiles was wider in the United States than in Europe
- The poorest Americans appeared to have the lowest survival among all wealth groups in the study sample
- Survival among the participants in the top wealth quartiles in northern and western Europe and southern Europe appeared to be higher than that among the wealthiest Americans
- Survival in the wealthiest U.S. quartile appeared to be similar to that in the poorest quartile in northern and western Europe

The countries in the Survey of Health, Ageing, and Retirement in Europe (SHARE) were split into the following three groups: northern and western Europe (Austria, Belgium, Denmark, France, Germany, the Netherlands, Sweden, and Switzerland), southern Europe (Italy, Portugal, and Spain), and eastern Europe (Czech Republic, Estonia, Hungary, Poland, and Slovenia). The shaded area in Panel A indicates the difference between quartile 4 (the wealthiest) and quartile 1 (the poorest) in the Health and Retirement Study (HRS); the same shaded area was added in Panels B, C, and D for the purposes of comparison. The median duration of follow-up was 10 years in both surveys, and the mean (±SD) age at baseline was 65±9.8 years.
In their discussion, the authors note that health care access should not be a factor for wealthy Americans. However, “systematic factors may influence longevity across social strata, such as diet; environment; behavioral, cultural, and social attitudes; and opportunities for social mobility.2,28,32,33 The poorest are most vulnerable to these systemic factors, but these factors are broad and probably affect the entirety of society.”
My take: This study indicates that mortality in the United States is higher than in Europe, even at higher wealth levels.
Commentary on this article from NBC News (4/2/25): Not even wealth is saving Americans from dying at rates seen among some of the poorest Europeans
“Fifty years ago, life expectancy in the U.S. and wealthy European countries was relatively similar. That began to change around 1980. As European life expectancy steadily increased, the U.S. struggled to keep pace — and its life expectancy even began declining in 2014…The wealthiest group in northern and western Europe had mortality rates about 35% lower than the wealthiest group in the U.S.”
Related blog posts:
- Ten Americas: Examining Health Disparities and Life Expectancy
- No Exaggeration: Too Many Children Are Dying in the U.S.
- Firearms: #1 Cause of Pediatric Deaths & Households with Guns =More Deaths
- New study finds 45,000 deaths annually linked to lack of health …
- U.S. Health System: ‘World Leader in Amputations’
- Life Expectancy Dropping in U.S. (post in 2023)
- Zip code or Genetic code -which is more important? gutsandgrowth
- “More Than Half a Million Extra Deaths” Every Year In U.S.