

NEJM Presidential Candidate Health Proposals
Full text: My Vision for Universal, Quality, Affordable Health Care –NEJM
From NEJM: The editors invited the Democratic and Republican presidential nominees, Hillary Clinton and Donald Trump, to answer the following question for Journal readers: What specific changes in policy do you support to improve access to care, improve quality of care, and control health care costs for our nation? Secretary Clinton responded. Mr. Trump did not respond.
The main topics in Hillary Clinton’s commentary include expanding insurance coverage through the affordable care act (i.e. Obamacare), improve affordability in health care with proposals that affect both insurance companies and pharmaceutical companies, improve access to primary care/community care, and to continue to promote innovation/research.
FDA Expands Use of Cystic Fibrosis Medication
Molecular Panels for Identifying Etiology with Acute GI Symptoms
A recent study (MR Nicholson et al. J Pediatr 2016; 176; 50-6) examined the use of multiplex molecular testing to determine the etiology of acute gastroenteritis in children. It is interesting that little has been published about this increasingly common practice of sending a 12 to 15 panel PCR assay when faced with acute GI symptoms, mainly diarrhea.
This study was a prospective population-based study of children <6 years with acute gastroenteritis (2008-2011).
Findings:
- 70.4 % (152/216) samples tested positive for a pathogen, with norovirus the most frequent (n=78, 36.1%). Clostridium difficile was next at 16.2% (n=35).
- 22.7% (n=49) tested positive for more than 1 pathogen including 25 with a C difficile detection
- In this study, the authors noted C difficile colonization in 8% of healthy children aged 0-51 months and in 14% of children <12 months
Implications of this study and this technology:
- Prior to this technology, traditional approaches typically identified less than 15% of the cases of acute gastroenteritis. Thus, this new technology increases the likelihood of a definitive diagnosis.
- Multiple pathogens, particularly with C difficile, illustrate how this new technology will present some difficulties with interpretation. C difficile has very high rates of colonization in infants (anywhere from 25-80%) without AGE symptoms and lower rates of colonization in toddlers. High colonization/detection has been noted in inflammatory bowel disease patients (17%) and pediatric oncology patients (30-55%).
- For C difficile, molecular testing is much less likely to correlate with clinical disease than toxin-based assays. “A recent study in adults found that virtually all CDI-related complications occurred in patients with a positive toxin immunoassay.” (JAMA Intern Med 2015; 175: 1792-801)
My take: These panels are helpful in identifying infectious etiologies of AGE and may help prevent unnecessary endoscopic procedures. Due to their limitations, careful selection of which patients to test and cautious interpretation of the results are needed.
Related blog posts:
- Overdiagnosis of Clostridium difficile with PCR Assays | gutsandgrowth
- Closer to Star Trek Medicine GutsAndGrowth

Sunset from Bar Harbor, ME
One of 340,000 Followers of NEJM
A recent editorial (EW Campion et al. NEJM 2016; 375: 993-4) made a few worthwhile points and shows how NEJM has been successful and innovative over 20 years of using the web and social media.
- This has allowed more widespread access to its content, even by resource-poor countries.
- The use of the web has facilitated quick distribution of multiple resources for outbreaks like Ebola and Zika.
- Currently, every article back to 1812 is available online (over 173,000 with more than 570,000 pages)
- NEJM has 340,000 twitter followers and 1.3 million followers on facebook
- Despite the importance of NEJM, as well as other healthcare media, important caution is needed.
“We do need to be wary of challenges and dangers that the new media have created. On the Internet, speed and simplicity often displace depth and quality, especially on complex subjects. Our privacy is increasingly vulnerable. Misinformation, misrepresentation, and piracy are common. There are health scams and even sham medical conferences and fake medical journals.”
My take: Careful use of internet resources has been incredibly helpful. But, beware of the inherent hazards that have accompanied these advances.
Related blog posts:
- Why I blog | gutsandgrowth
- Why Social Media is Important for Doctors | gutsandgrowth
- Incorporating Social Media into Medicine | gutsandgrowth
- Personal Look at 20 Years of Doctoring (Part 2) | gutsandgrowth

Balancing Rock, Bar Harbor
Antipsychotic Agent, Olanzapine, Helps in Reducing Chemotherapy-Induced Nausea/Vomiting
Briefly noted: RM Navari et al. NEJM 2016; 375: 134-42. Olanzapine (marketed as Zyprexa), compared with placebo, in combination with dexamethasone, aprepitant (or fosaprepitant) and a 5-hydroxytryptomaine type 3 antagonist (eg palonosetron, ondansetron, or granisetron) helped reduced nausea/vomiting. Among a total of 380 patients, 74% in the olanzapine group had no nausea/vomiting compared with 45% in the placebo group in the first 24 hours. In the 1st 120 hours, the rates of no nausea/vomiting were 37% vs. 22%. A “complete response,” defined as no emesis episodes and no rescue medications, occurred in 64% vs 41% in the 1st 120 hours. The most concerning side effect reported was severe sedation which was reported in 5%.

Arthur Ravenel Jr Bridge
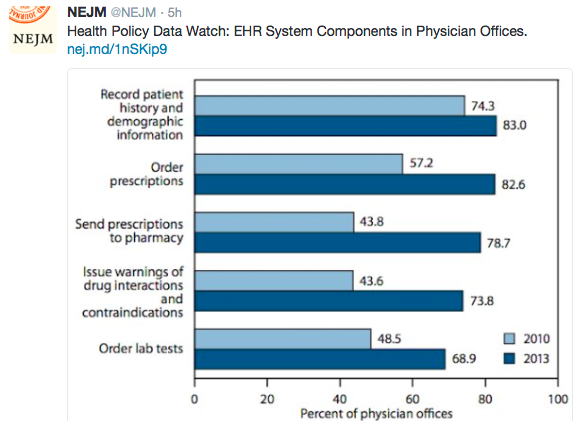
Image Only: EMR Uptake
Image
Increased Intestinal Blood Flow with Bolus Feedings in Very Low Birth Weight Infants
From Journal of Pediatrics: V Bozzetti et al. DOI: http://dx.doi.org/10.1016/j.jpeds.2016.05.031
Objective
To detect changes in splanchnic perfusion and oxygenation induced by 2 different feeding regimens in infants with intrauterine growth restriction (IUGR) and those without IUGR.
Study design
This was a randomized trial in 40 very low birth weight infants. When an enteral intake of 100 mL/kg/day was achieved, patients with IUGR and those without IUGR were randomized into 2 groups. Group A (n = 20) received a feed by bolus (in 10 minutes), then, after at least 3 hours, received the same amount of formula by continuous nutrition over 3 hours. Group B (n = 20) received a feed administered continuously over 3 hours, followed by a bolus administration (in 10 minutes) of the same amount of formula after at least 3 hours. On the day of randomization, intestinal and cerebral regional oximetry was measured via near-infrared spectroscopy and Doppler ultrasound (US) of the superior mesenteric artery was performed. Examinations were performed before the feed and at 30 minutes after the feed by bolus and before the feed, at 30 minutes after the start of the feed, and at 30 minutes after the end of the feed for the 3-hour continuous feed.
Results
Superior mesenteric artery Doppler US showed significantly higher perfusion values after the bolus feeds than after the continuous feeds. Near-infrared spectroscopy values remained stable before and after feeds. Infants with IUGR and those without IUGR showed the same perfusion and oxygenation patterns.
Conclusion
According to our Doppler US results, bolus feeding is more effective than continuous feeding in increasing splanchnic perfusion.
Related blog posts:
- Which is Safer –Drip Feeds or Bolus Feeds in Healthy … – gutsandgrowth
- Continuous versus Bolus Feeds GutsandGrowth

Iceberg Lake, Glacier Natl Park
FDA Gives Ustekinumab (Stelara) Approval for Crohn’s
Here’s a link summarizing FDA approval: Medscape: FDA Clears Ustekinumab (Stelara) for Crohn’s Disease
An excerpt:
The US Food and Drug Administration (FDA) has approved ustekinumab (Stelara, Janssen Biotech, Inc) for the treatment of moderately to severely active Crohn’s disease in patients aged 18 years or older.
Specifically, the interleukin-12/23 inhibitor is indicated for Crohn’s patients who have failed or were intolerant to immunomodulator or corticosteroid therapy but who never failed treatment with a tumor necrosis factor (TNF) blocker or who failed or were intolerant to treatment with one or more TNF blockers, according to a company news release.
Ustekinumab is already approved in the United States for treatment of patients with plaque psoriasis and psoriatic arthritis…The clinical development program for ustekinumab for Crohn’s disease included more than 1300 patients across three pivotal phase 3 studies, which served as the primary basis for FDA approval.
In clinical studies of patients who were either new to, experienced with, or failed anti-TNF therapy, between 34% and 56% of patients experienced symptom relief in the 6 weeks after receiving a one-time intravenous induction dose of ustekinumab. “Noticeable improvement was observed as early as 3 weeks,” the company said.
Most patients who responded to induction dosing and who continued ustekinumab treatment with subcutaneous maintenance doses every 8 weeks were in remission at the end of 44 weeks (52 weeks from initiation of the induction dose), the company said.
Full prescribing information and a medication guide are available online.
The Indispensable Physician
A recent pair of commentaries (RM Wachter, L Goldman. NEJM 2016; 375: 1009-1011, R Gunderman. NEJM 2016; 375; 1011-13) provides some insight into what has been gained and what has been lost with the proliferation of hospitalist care in the past 20 years.
The growth of hospitalist care has developed due to numerous factors:
- evidence of cost savings/better outcomes
- need for rapid evaluation of acutely ill patients/repeated evaluations which would be disruptive to efficient outpatient physician practices
Decline of comprehensive care:
- at times of extreme vulnerability when admitted to the hospital, patients have a physician assigned to them who they have probably never met. This has led to a diminishment of the patient-physician relationship.
- increasing number of physicians creates opportunities for miscommunication, particularly on admission and discharge, but also at every step of hospital care during “handoffs”
The second commentary, in particular, challenges the way medicine is evolving. This article stresses the central role of the physician as opposed to the hospital filling that role.
“The reality is that medicine can be practiced without hospitals, but hospitals cannot function without physicians.”
The goal of developing personal relationships with our patients is often at odds with work-life balance. Thus, having hospitalists and other ways of having cross-coverage, when we are unavailable, often conflict with being able to provide the best care.
My take (from 2nd commentary): “The true core of good medicine is not an institution but a relationship — a relationship between two human beings.”
Related blog posts:
- “Weekend Effect” –From the Other Side of the Bed | gutsandgrowth Are hospitals really Focused on patients or their physicians/employees?
- “I’ve Got the Best Doctor” | gutsandgrowth
- Better Discharge Planning Needed | gutsandgrowth
- Increasing Rates of Professional Burnout | gutsandgrowth
- “It is never boring to be a physician” | gutsandgrowth

Glacier Nat’l Park
