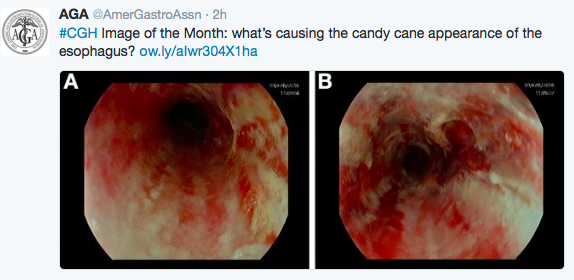
In this picture of a ‘candy cane appearance’ of the esophagus, the 19 year old patient subsequently admitted to drinking boiling hot tea. A complete recovery was noted.

In this picture of a ‘candy cane appearance’ of the esophagus, the 19 year old patient subsequently admitted to drinking boiling hot tea. A complete recovery was noted.
Newsflash: Advertising usually works! That’s the quick conclusion from two studies that looked closer at the influence of food advertising on children.
The first study recruited 209 children aged 4-8 years and asked them to rate their taste preferences for 3 matched food pairs, presented with or without a brand equity character displayed on packaging. Key finding: “Children were significantly more likely to show a preference for foods with a brand equity character displayed on the packaging.” Thus, the authors conclude that these characters promote unhealthy food choices (foods high in fat, salt, and sugar) in children.
As an aside, the reverse of this type of branding happened with Obamacare: Jimmy Kimmel Obamacare vs Affordable Care Act
So how do televised food commercials work to change children’s preferences? The second study examined 23 children aged 8-14 years with functional magnetic resonance imaging while they were making food choices. Children assessed 60 food items. Key finding: After commercials, children placed significantly more importance on taste of these food items. “The ventromedial prefrontal cortex, a reward valuation brain region, showed increased activity during food choices after watching food commercials compared with after watching nonfood commericals.”
My take: Watching food commercials probably increases the likelihood of consumption of a less healthy diet.
Related blog posts:

Berry College, 42 ft Wood Wheel
Gut Microbial Diversity is Reduced in Smokers with Crohn’s Disease. JL Opstelten et al. Inflamm Bowel Dis 2016; 22: 2070-77. This study compared stools from 21 nonsmoking patients with Crohn’s disease (CD) with 21 smokers with CD. Smoking was accompanied by a reduced relative abundance of multiple genera. My take: It is unclear whether smoking’s effect on the microbiome directly contributes to worsened outcomes or whether the changes in the microbiome are only an epiphenomenon. Regardless, smoking increases the likelihood of worse outcomes in CD.
A Systematic Review on Infliximab and Adalimumab Drug Monitoring Levels, Clinical Outcomes and Assay. F Silva-Ferreira et al. Inflamm Bowel Dis 2016; 22: 2289-2301. This review selected 20 studies from an initial query of 1654 articles. Key points:
“Is it good to try to live as moral a life as possible –a saintly life? Or does a life like that lack some crucial human quality? …Is it presumptuous, even blasphemous, for a person to imagine that he can transfigure the world –or to belive that it really matters what he does in his life when he’s only a tiny flickering speck in a vast universe?”
—Strangers Drowning, Larissa Macfarquhar
Frequently I think about the question of what I want to accomplish in my role as a physician. Sometimes the answer is to get home at a reasonable hour that day. However, when looking past the day-to-day, I definitely strive for more, even if I am only a tiny fleck in the universe.
I like to think that I’ve tried to help families that see me as best as I can. I try to make sure that I am not overbooked so that I have enough time to think about problems carefully and perhaps have an opportunity to make a connection/have a conversation with families who come to see me.
So much of what I do everyday becomes fairly routine, particularly when in the office. For a family who has a child with severe stomach pain and is missing school, this is a critical problem. Yet, I may see several similar children each day of the week. I know that the child will improve, but I don’t know exactly how long it will take and how difficult it will be.
Most of the problems that I see are alarming for parents, including the following:
Yet, very few patients who come to our office need to be admitted to the hospital. Most of the time, some fairly routine advice and/or treatment will resolve (or at least improve) these problems.
In clinical care, what really stands out for me is when a rare medical problem is quickly identified and treated. I was delighted recently when I helped establish a diagnosis of chronic granulomatous disease in one child when he was seen at his first encounter with me. In the previous week, I identified a child with familial Mediterranean fever. Both of these problems are extremely rare and can be difficult to diagnose.
But truly, how often does it matter if a child sees me compared with another pediatric gastroenterologist? My suspicion is that most of the time it does not matter; though this opinion may be due to the fact that I’ve had the chance to work with some truly terrific colleagues. So while it is gratifying to help families, I am often thinking about what I can do to accomplish more. I am sure others struggle with the same issue of trying to do meaningful work. Some may leave a legacy through their focus on research, teaching or charity.
In some ways, I have considered my participation in the AAP, my blog, my role at the hospital, and (at times) research/teaching as important opportunities for different types of work to keep everyday a little more exciting and to make a useful contribution.
What are you trying to accomplish?
Related blog posts:

Sunrise at Spruce Point, Maine
From NPR: Can A Vegan Diet Give You All You Need? German Nutritionists Say ‘Nein’
An excerpt:
“With a pure plant-based diet, it is difficult or impossible to attain an adequate supply of some nutrients,” states the German Nutrition Society’s new position on the vegan diet. “The most critical nutrient is B-12,” which is found in eggs and meat. The group says if you follow a vegan diet, you should take supplements to protect against deficiencies.
According to the German nutritionists, other “potentially critical nutrients” that may be a challenge to get in a vegan diet include omega-3s — found in fatty fish — as well as minerals such as calcium, iron, iodine, zinc and selenium. So the group recommends that vegans get advice from a nutrition counselor and be “regularly checked by a physician.” In addition, the society recommends against a vegan diet for pregnant women, women who are breast-feeding, children and adolescents…
“B-12 only comes from animal products,” says Cimperman. “It’s necessary for proper red blood cell formation, as well as normal neurological function.”
Many foods — including some breakfast cereals, as well as some nondairy creamers and milks — are fortified with B-12. So it’s possible to get all the nutrition you need this way, if you eat enough of these fortified foods regularly.
But to make sure you’re covering all your bases, “I would recommend [taking] a standard multivitamin,” Cimperman says. It’s a good insurance policy for vegans.

Pat O’Brien’s Patio, New Orleans



![]()


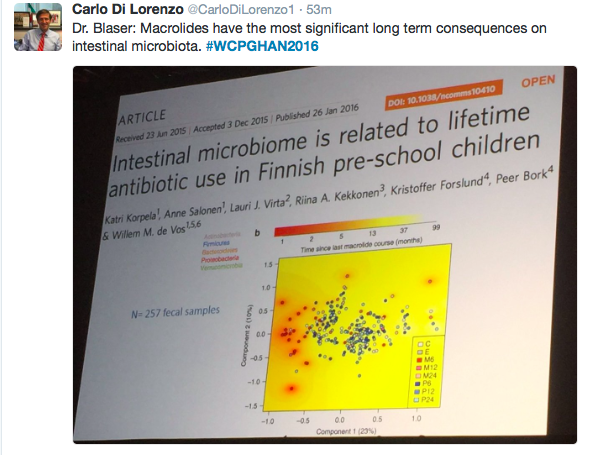
Here are some more provocative tweets from World Congress of Pediatric Gastroenterology Hepatology and Nutrition:
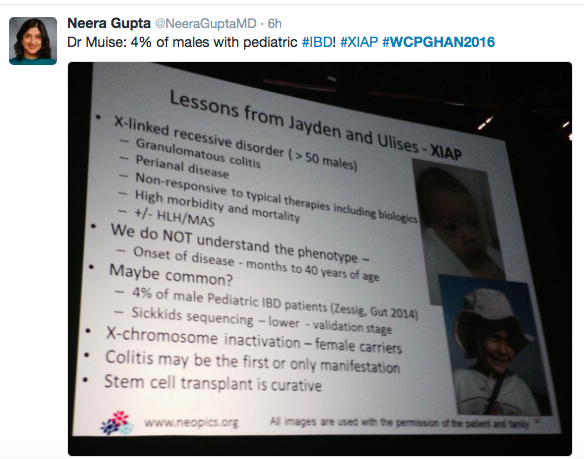
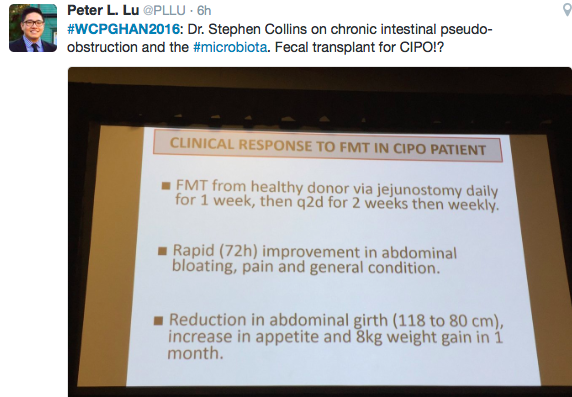



For those who are not attending this year’s national/international GI meeting, I’ve compiled some of the best tweets. These tweets are from 10/6/16.




A recent commentary (G Cholankeril et al. Gastroenterol 2016; 151: 382-86) provides a succinct summary regarding the trends in liver transplantation multiple listing and its implications on notions of utility and justice.
Key points:
Regional distribution:
My take: Under the current system, liver transplant candidates capable of travelling/multiple listing, are rewarded with earlier liver transplantation & higher likelihood of receiving a liver transplant. Thus, until inequities in organ distribution are better addressed, patient’s may need to consider telling their transplant team: ‘Need Liver, Will Travel’
Related blog posts:

Public Art, New Orleans

