The author notes that increasingly there are long waits to get appointments to see pediatricians. In addition, pediatricians rely on a referral network (e.g. pediatric subspecialists, psychologists, psychiatrists) and there are shortages and delays in getting seen in these fields as well.
An excerpt:
There aren’t enough pediatricians right now, and because of that, some kids are unable to get the care they need…
Approximately 30 percent of pediatric training programs failed to fill their available residency slots, leaving 252 positions vacant — a notable increase from just 88 vacant spots last year. This isn’t a minor hiccup; it’s a warning for the future of pediatric care in the United States…Last year, a National Academies of Sciences, Engineering and Medicine committee published a report on the future of the pediatric work force and the issue of shortages, especially in rural areas. It underscored the fragmentation in care coordination between pediatric primary care and specialty care exacerbated by geographic barriers and inadequate financial support.
The elephant in the exam room, though, is that pediatricians earn less than specialists in almost every other medical field in the United States. A key reason is that so many children live in poverty and therefore qualify for Medicaid, which pays far less for care than private insurance and even less than Medicare.
We need immediate action to address this crisis and find ways to attract more graduates to pediatrics. Our children are the future, but we sure don’t act like it when it comes to health care.
My take: Most pediatric physicians chose pediatrics to work with families and children. At this time, growing debt and pay inequity are factors causing many to choose other areas in medicine and needs to be addressed.
RM Touyz et al. NEJM 2024; 390: 1998-2009. Magnesium Disorders
Magnesium “is present in all cells in all organisms from plants to higher mammals and is indispensable for health and life because it is an essential cofactor for ATP, the cellular source of energy…All ATPase reactions require Mg2+–ATP, including those involved in RNA and DNA functions…Magnesium is involved in the control of neuromuscular function, regulation of cardiac rhythm.”
Key points:
“Hypomagnesemia is present in 3 to 10% of the general population, but its prevalence is increased among persons with type 2 diabetes and hospitalized patients.”
“Hypomagnesemia is usually associated with other electrolyte derangements, including hypocalcemia, hypokalemia, and metabolic alkalosis, and refractory hypokalemia” (& refractory hypocalcemia) is often responsive to treatment only after the magnesium concentration has been normalized.
“Patients with hypomagnesemia often present with nonspecific symptoms, such as lethargy, muscle cramps, or muscle weakness, and thus the diagnosis of magnesium deficiency may be overlooked.”
“Many drug classes, such as antibiotics, diuretics, biologic agents, immunosuppressants (including tacrolimus and rapamycin), proton-pump inhibitors, and chemotherapies, cause renal magnesium loss and hypomagnesemia.”
“Long-term use of PPIs causes magnesium deficiency in approximately 20% of patients receiving them, and these effects are dose-dependent. PPIs reduce intestinal magnesium uptake.”
“Dietary sources rich in magnesium include cereals, beans, nuts, and green vegetables (magnesium is the central core of chlorophyll). Of the total dietary magnesium consumed, 30 to 40% is absorbed in the intestine.”
“Magnesium is a key component of bone — 60% of the total magnesium in the body is stored in this compartment.” Adequate magnesium intake can reduce fractures and osteopenia.
The intestines-bone-kidney axis regulate magnesium. “Hypomagnesemia may result from inadequate dietary intake, increased gastrointestinal loss, reduced renal reabsorption, or redistribution of magnesium from the extracellular to the intracellular space.” Rarely, hypomagnesemia is related to genetic causes.
Magnesium replacement is the basis for managing hypomagnesemia. “The most effectively absorbed forms are organic salts (magnesium citrate, aspartate, glycinate, gluconate, and lactate) rather than inorganic salts (magnesium chloride, carbonate, and oxide). However, a common side effect of oral magnesium supplementation is diarrhea, which poses a challenge for oral replacement.”
Intravenous magnesium (magnesium sulfate) is given for more severe deficiency and often therapeutically for torsades de pointes, acute asthma exacerbations, and preeclampsia or eclampsia.
This article is geared to adult medicine. Children less frequently have hypomagnesemia which is likely related to less frequent comorbidities.
My take: In pediatric patients taking PPIs as long-term therapy, checking magnesium levels is important particularly if there are multiple medications which could affect levels and if there are other comorbidities (e.g. renal disease).
Key findings: This small retrospective pediatric study included 31 patients with a mean age of 7.8 years with 74 serum Mg levels. Only 2 patients, of adult age, had Mg levels below the normal reference limit of 1.6 mg/dL
This retrospective study examined 546 children with esophageal atresia (EA) who underwent 1,473 surveillance endoscopies (2004-2023). The authors defined a hiatal hernia as at least 1 cm of gastric folds present above the level of the diaphragmatic pinch. “Actionable findings” were any finding that prompted a change in management.
Key findings:
A total of 770 endoscopies (52.2%) in 394 unique patients (72.2%) had actionable pathology
The most common actionable finding was esophagitis which lead to escalation of therapy (484 endoscopies in 32.9% of patients). However, de-escalation of therapy was common as well; this occurred in 233 patients (after 310 endoscopies)
Barrett’s esophagus (intestinal metaplasia) was identified in 7 unique patients (1.3%) at a median age of 11.3 years. 6 of 7 patients with Barrett’s were receiving acid suppression at time of diagnosis
Actionable findings leading to surgical intervention were found in 55 children (30 refractory reflux and 25 tracheoesophageal fistulas).
Significant predictors of actionable pathology included increasing age, long gap atresia, and hiatal hernia.
Symptoms were not predictive of actionable findings, except dysphagia (OR 5.80), which was associated with stricture.
Acid suppression was associated with a reduced odds of actionable findings (OR 0.78); however, there was still a high rate of actionable findings in this group. 51% of endoscopies while a patient had been receiving acid suppression had actionable findings.
Fundoplication was NOT associated with protection against actionable findings (OR 1.42)
Table 2 notes that 52 (3.5%) patients had eosinophilic esophagitis therapy escalated. Infrequently, non-esophageal diseases were identified: Celiac in 3 patients (0.2%), Crohn’s disease in 2 patients (0.1%), eosinophilic gastritis and/or duodenitis in 2 (0.1%), and H pylori in 4 patients (0.3%).
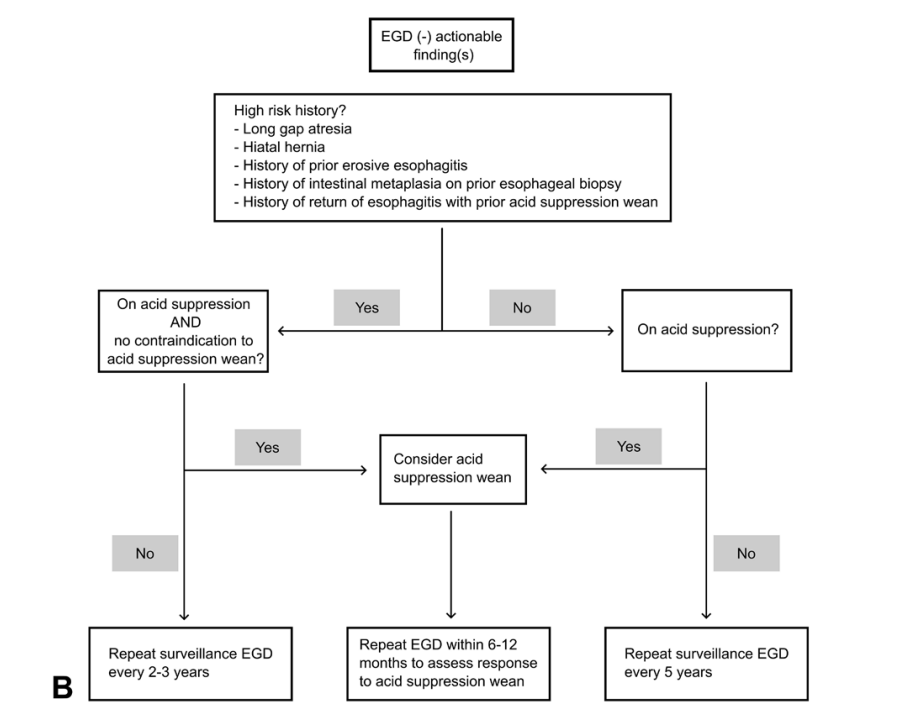
Proposed Management Algorithms:
Discussion Points (from authors):
Take multiple levels of esophageal biopsies: “Any surveillance esophagogastroduodenoscopy (EGD) should at minimum include 2 to 3 levels of esophageal biopsies”
Acid suppression recommendations: “Barrett’s esophagus is proposed to be an absolute contraindication to acid suppression wean; relative contraindications to weaning acid suppression include earlier erosive esophagitis, earlier failed acid suppression discontinuation attempt(s) with rebound esophagitis, or hiatal hernia; if acid suppression is weaned in these high-risk situations, we believe close follow-up endoscopy is warranted to assess for rebound pathology [which happened in nearly 20%].” And, “our practice is to empirically de-escalate acid suppression in children without contraindications to doing so when there is no gross esophagitis and biopsies show no or minimal inflammation (generally less than 5 eosinophils per high powered field).”
Consider doing endoscopy off acid suppression for approximately three months: “To maximize the information yield from the initial endoscopy, a patient may first wean off acid suppression approximately 3 months before endoscopy to permit evaluation for both anatomy and esophagitis off acid suppression. Subsequent surveillance is performed according to our algorithm and within at most 6 to 12 months of any acid suppression changes.”
The authors do not generally recommend pH-Impedance. “There are no consensus “normal” values for pH-impedance reflux parameters in either healthy or EA children, and pH-impedance has failed to show any predictive correlation with actual esophagitis in multiple pediatric studies. In particular, children with EA with “normal” numbers of reflux events cannot adequately clear their refluxate in the context of poor esophageal motility and can still develop reflux injury. pH-impedance tracings in EA require manual review by an experienced reader, with automated analysis being highly unreliable in the setting of low baseline impedance values.”
Limitations: 1. Some of the actionable findings may have been expected based on prior endoscopies (e.g. prior stricture) and could influence value of symptoms like dysphagia. 2. This population was skewed to patients with more severe EA as it is a subspecialty center. One indicator was that their group had 24% with long-gap EA compared to an overall expected rate of 10% in the general EA population 3. Retrospective study 4. Many of the patients were not truly “surveillance” endoscopies but were done due to reported symptoms
My take: It’s unfortunate that this article did not get published in a more mainstream pediatric journal (e.g. JPGN, J Pediatr, Pediatrics) or a more mainstream gastroenterology journal (eg. Gastroenterol, Clin Gastroenterol Hepatol, AJG) as this article provides a lot of great data and useful advice. More than 70% of subjects had actionable findings during the course of their follow-up, including more than 40% of 1 year-olds.
The algorithms above suggest that at minimum, EA patients should have endoscopy every 5 years (likely starting between 12-18 months). More frequent endoscopy (every 2-3 years) may be worthwhile in those with risk factors (e.g. long gap EA, hiatal hernia, and prior esophagitis) and follow-up endoscopy is needed sooner if change in therapy (stricture dilation, esophagitis treatment or treatment de-escalation).
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
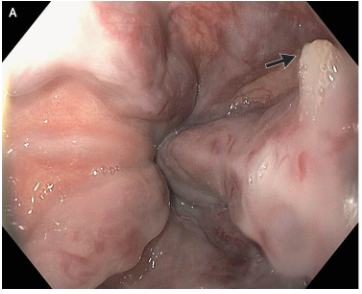
M Najem, E Dong. N Engl J Med 2024;390: e47. Esophageal Varices, White-Nipple Sign, and Portal Hypertensive Gastropathy
This case reported on a 66 year old with cirrhosis and variceal bleeding. “One varix had a “white-nipple sign” (Panel A, arrow), which indicates recent variceal hemorrhage and results from the formation of a fibrin plug at the site of a resolved thrombus.”
“Though not widely mentioned as a stigma of recent variceal hemorrhage, this finding was first reported by Chung and Lewis in 1984 [4]. They described it as a white nipple on top of a varix protruding into the lumen and noted its presence in up to 5% of cases of variceal bleeding. It was thought to represent a platelet-fibrin plug at the site of recent variceal rupture. They noted that dislodgement would be accompanied by jet-like bleeding and called it ‘Mount St. Helens’ sign’ due its volcanic-like eruption…As Chung and Lewis [4] initially suggested, it should ‘alert the endoscopist to take urgent measures to avert a disaster’. Recognizing it as such, attempts to dislodge the lesion must be avoided and endoscopic therapy should be undertaken.”
#NASPGHAN19 Liver Symposium (excellent presentation by Dr. Romero on varices in children and portal hypertension)
Time to Adjust the Knowledge Doubling Curve in Hepatology For Platelets in the setting of cirrhosis: “Given the low risk of bleeding of many common procedures, potential risks of platelet transfusion, lack of evidence that elevating the platelet count reduces bleeding risk, and ability to use effective interventions, including transfusion and hemostasis if bleeding occurs, it is reasonable to perform both low‐ and high‐risk procedures without prophylactically correcting the platelet count...An individualized approach to patients with severe thrombocytopenia before procedures is recommended because of the lack of definitive evidence for safety and efficacy of interventions intended to increase platelet counts in patients with cirrhosis.” The authors note in Table 4, that the AASLD does not have a specific threshold for platelets, whereas other societies have used values of >30 or >50.
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
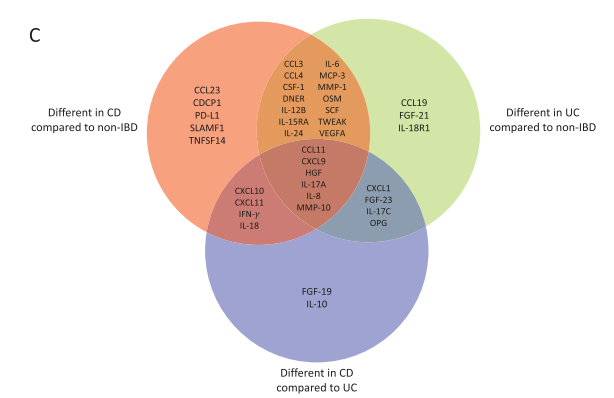
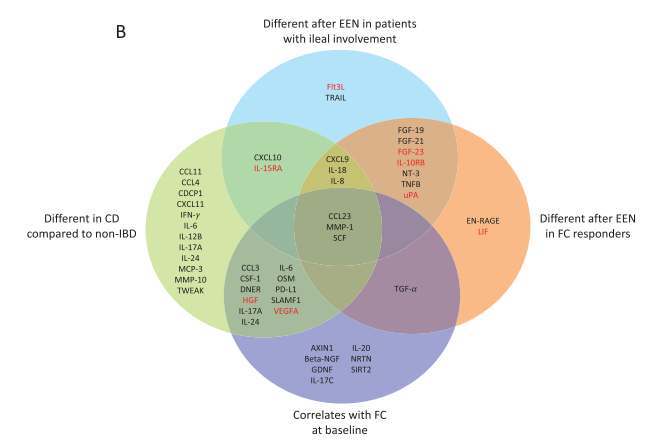
Background/Methods: The authors characterized the plasma levels of inflammation-related proteins (IRPs) in children with CD and ulcerative colitis (UC) compared with noninflammatory controls (non-IBD) and explored the effect of EEN in children with CD. Population included children with CD (n = 53), UC (n = 11), and non-IBD (n = 19). For 18 children with active CD, IRPs were measured before and after 8 weeks of EEN.
Key findings:
Compared with non-IBD, patients with active UC and CD had different levels of 27 (24 raised, 3 decreased) and 29 (26 raised, 3 decreased) IRPs, respectively.
Exclusive enteral nutrition modified the levels of 19 IRPs (13 increased, 6 decreased including CCL23, interleukin-24, interleukin-6, and MMP-1).
More pronounced changes in IRP profile were observed in patients with ileal involvement and a ≥50% decrease in fecal calprotectin during EEN.
The discussion notes that “these profiles also helped to uncover some of the underlining pathological mechanisms, with CD demonstrating enhanced levels of IRPs related to IFN-γ and Th1-associated pathways, whereas in UC we observed an enrichment in IRPs related to Th17 pathways.”
My take (borrowed from authors): Inflammation-related protein profiles could help to stratify patients likely to respond to treatment with EEN.
, Venn diagram of the proteins found to be signifcantly different between each IBD subtype compared to non-IBD controls and between each IBD subtype.Venn diagram summarizing the main significant (P ≤ .05) differences or correlations found in IRPs. Proteins highlighted in red were shown to significantly interact with thiopurines
F Koutny et al. JPGN 2024;https://doi.org/10.1002/jpn3.12194. Open Access! Poorly controlled pediatric type 1 diabetes mellitus is a risk factor for metabolic dysfunction associated steatotic liver disease (MASLD): An observational study
Study population, n=32,325. Key finding: Inadequately controlled T1D (HgbA1c >11%) was associated with a higher hazard ratio ((HR: 1.54) of elevated ALT values compared to children with controlled T1D over an observation period extending up to 5.5 years. When both elevated HbA1c (>11%) and overweight were present, the HR was 2.71.
————————————————————————————————————————–
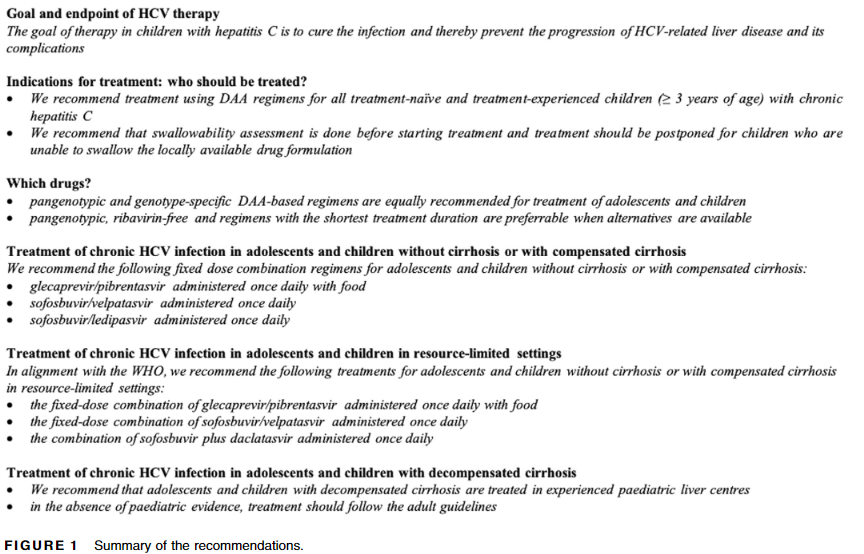
2. G Indolfi et al.JPGN 2024;78:957–972. ESPGHAN recommendations on treatment of chronic hepatitis C virus infection in adolescents and children including those living in resource-limited settings
Summary of Recommendations:
————————————————————————————————————————–
3. F Lacaille et al. JPGN 2024; 78:1374–1382. Awareness, referral and age at Kasai surgery for biliary atresia in Europe: A survey of the Quality-of-Care Task Force of ESPGHAN
Key finding: Data from 785 infants diagnosed with BA from 2015 to 2019 from 18 centers in 15 countries revealed a mean age at referral to tertiary center of 55 days (similar to results obtained in Europe 10–30 years earlier)
Methods: Using a population-based claims database in Japan, the authors identified patients who were prescribed a clarithromycin-based first regimen of Hp eradication between 2015 and 2018.
Key findings:
Among 54,055 patients, 568 (1.05%) developed gastric cancer (GC) during the follow-up period (mean, 3.65 years).
The cumulative incidence of GC was 1.64% at 3 years, 2.02% at 4 years, and 2.36% at 5 years in potassium-competitive acid blocker (PCAB) users and 0.71% at 3 years, 1.04% at 4 years, and 1.22% at 5 years in H2RA users.
Limitations: retrospective study with issues of selection bias and confounding.
In the discussion, the authors note PCABs are being used not only for Hp eradication but for peptic ulcers, reflux and several abdominal symptoms. “According to the results of our study, longer use of PCABs was particularly associated with the increased risk of GC after Hp eradication…it might be better to switch strong acid inhibitors including PCABs ad PPIs to H2RAs before reaching a lengthy prescription period (eg. more than 3 years).”
This multicenter, prospective, randomized controlled, noninferiority trial enrolled patients (n=516) with treatment naive H pylori infection from 5 clinical centers. All patients received vonoprazan at 20 mg 2/day. The high dose amoxicillin was 750 mg 4/day and the low dose 1000 mg 2/day.
Key findings:
The high-dose amoxicillin combination with vonoprazan regimen, for either 10 or 14 days, was effective and safe in eradicating H pylori, whereas the low-dose amoxicillin regimen for 10 days was less effective. The high-dose per protocol eradication rates were 90.9% vs 94.5 for 10 vs 14 days compared to 82.0% in the low-dose per protocol eradication rate (for 14 days).
My take: These studies indicate that PCABs are more effective at healing erosive esophagitis as well as H pylori gastritis. However, particularly in patients with Hp infection, the use of PCABs is associated with an increased risk of gastric cancer. The exact long-term risk of strong acid inhibition is unclear, especially in those without a history of Hp infection.
This study examined a prospective cohort linking data on breastfeeding on birth certificates (starting in 2016) to infant death rates. This included 9,711,567 live births and 20,632 post-perinatal infant deaths.
Key findings:
The overall adjusted OR for breastfeeding initiation with post-perinatal infant mortality was 0.67.
Table 1 provides a ton of information about demographics and associated outcomes: Better education was associated with lower post-perinatal (7-365 days) death rate per 1,000 births. College graduate rate was 0.91 compared to 3.43 for lower than high school. Age 30-34 was 1.53 compared to 3.87 for <20 years. Non-hispanic Asian, Non-Hispanic White, and Hispanic were 1.11, 1.79 and 1.58 and much better than Non-Hispanic Black which was 4.07. Smoking during pregnancy rate was 5.68 compared to 1.83 for non-smoking during pregnancy
Preterm infant had a much higher post-perinatal mortality rate: 7.97 vs 1.36 for term babies
One limitation that may contribute to an underestimate of the advantages of breastfeeding -this study determines only initiation of breastfeeding. Breastfeeding duration of >3 months has been associated with decreased infant mortality. In other words, in infants with longer breastfeeding, the advantages are likely to be more pronounced. Breastfeeding has been associated with lower rates of necrotizing enterocolitis and sudden unexpected infant deaths.
My take: Breastfeeding appears to confer health benefits to infants and mothers. Some of the improvements in infant mortality likely are due to the association of breastfeeding with other characteristics that reduce infant mortality including education, non- smoking during pregnancy, older mothers and race. The authors note that race is a “social construct, but the systemic or structural disadvantages associated with race contribute to health disparities…A Black infant is 2.4 times more likely to die before his or her first birthday in the U.S. than a White infant.”
Feeling Guilty about Stopping Breastfeeding?Geoff Der, a statistician at the University of Glasgow who has worked with the same data in previous studies, said that the findings in the present study were robust and the authors’ method for eliminating selection bias was powerful…“In a society with a clean water supply and modern formulas,” he said, “a woman who isn’t able to breast-feed shouldn’t be feeling guilty, and the likelihood that there’s any harm to the baby is pretty slim.”
Mural from Funk Zone in Santa BarbaraSanta Barbara Botanical Gardens
9698 participants in NHANES during the 2017-2020 cycle completed a transient elastography examination. After excluding patients less than 18 years, these were the key findings:
37.87% had steatotic liver disease
32.45% had MASLD
2.56% had MetALD
1.17% and ALD
Limitations: database study, lack of liver biopsy, reliance on self-reports of alcohol consumption
Methods: 336,866 adults aged ≥30 years were prospectively enrolled in a health screening program between 1997–2013
Key findings:
122,669 (36.4%) had MASLD. Over a mean follow-up of 15 years, 5562 new cases of cirrhosis and 2273 new cases of HCC were diagnosed.
Hazard ratios for HCC were 8.86 for MASLD with HBV or HCV, compared with non-SLD without HBV or HCV
Hazard ratios for HCC were 8.81 for HBV or HCV with non-SLD (SLD), and 1.52 for MASLD without HBV or HCV
My take: MASLD significantly increased cirrhosis and HCC risks; however the risk of HBV or HCV was much greater. The high prevalence rates of MASLD guarantees a huge need for liver disease management for the foreseeable future.
Background: “Coconut water (CW) possesses anti-inflammatory properties, can potentially manipulate the microbiome, is a rich source of dietary potassium,” and may be an effective treatment for mild to moderate ulcerative colitis (UC).
Methods: Along with standard medical therapy, four hundred mL of CW (200 mL 2/day) or placebo fluid was administered for 8 weeks to adults (CW, n = 49; placebo, n = 46) with mild to moderate UC
Key findings:
Clinical response (57.1% vs 28.3%; odds ratio [OR], 3.4), remission (53.1% vs 28.3%; OR, 2.9), and proportion of patients with fecal calprotectin (FCP) <150 μg/g (30.6% vs 6.5%; OR, 6.3) all significantly favored CW group
There was not a significant difference in endoscopic outcomes
The authors indicate CW may be a useful adjunct for mild to moderate colitis but should be avoided in those patients taking medications that affect potassium and those with chronic kidney disease.
My take: This would be a good study to repeat to confirm whether CW is helpful for colitis. Certainly too much CW (a high FODMAP beverage) can contribute to a laxative effect and elevated potassium in some people. If a person with colitis is stranded on an island, CW may help until a rescue arrives.
In this prospective observational real-world treatment registry…
Key findings:
Of 1515 adalimumab-treated patients, 763 (50.4%) were classified as responders at 6 months
Compared with nonresponders, responders were less likely to have moderate to severe symptoms (55.6% vs 33%), or require steroids (45.5% vs 17.3%) or opiates (6.6% vs 1.3%) at baseline
During follow-up evaluation, using stabilized inverse probability of treatment weighting, responders were 34% less likely to experience serious infections compared with nonresponders (hazard ratio, 0.66)
The study results are similar to a registry-based rheumatoid arthritis study by Strangfeld et al (Ann Rheu m Dis 2011; 70: 1914-1920), which showed effective treatment was associated with less steroid use and a decline int risk of serious infections.
My take: This study indicates that lack of control of CD increases the risk for complications and infections. So, while patients are concerned about medication adverse effects, the complications of foregoing treatment or ineffective treatment are usually more concerning.