This retrospective trial included thirty three patients with Crohn’s disease (CD) receiving maintenance ustekinumab (UST). The simplified Magnetic Resonance Index of Activity (sMARIA) and biomarkers were correlated with UST levels. The authors utilized a homologous mobility shift assay (HMSA) (Prometheus) for their UST levels.
Key findings:
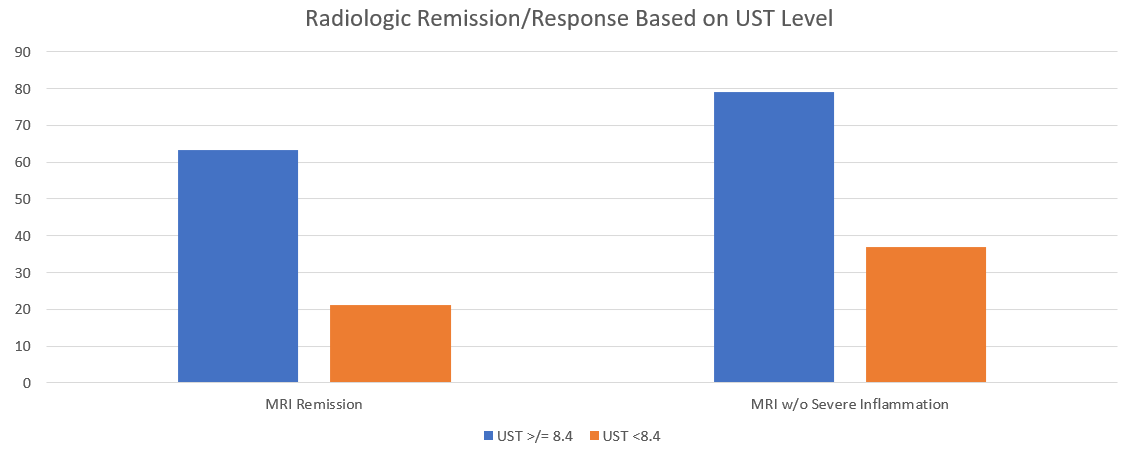
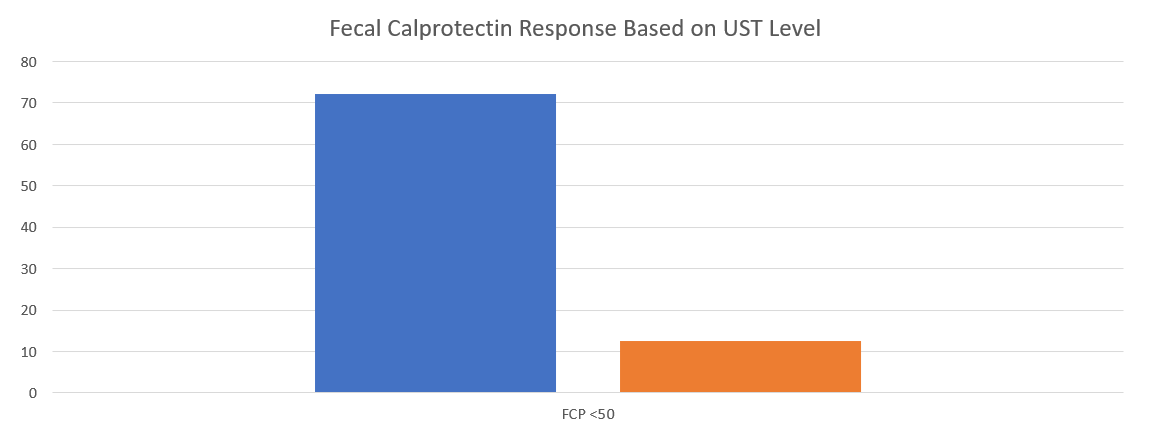
With UST level greater or equal to 8.4, radiologic remission was seen in 63% compared to 21% in those with levels <8.4. Similarly, the absence of severe inflammation was seen in 78.9% of those with higher levels compared with only 36.8% in those with levels below 8.4. Both findings were clinically-significant P=.01With UST levels greater or equal to 6.1, FCP less than 50 was seen in 72.2% compared to only 12.5% in those with a level less than 6.1. P<.01
My take: This study show the need for higher levels of UST to achieve optimal outcomes. Levels of at least 8.4 appear to be a good target.
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
In this study, ChatGPT answers to questions about colonoscopy were compared to publicly available webpages of 3 randomly selected hospitals from the top-20 list of the US News & World Report Best Hospitals for Gastroenterology and GI Surgery.
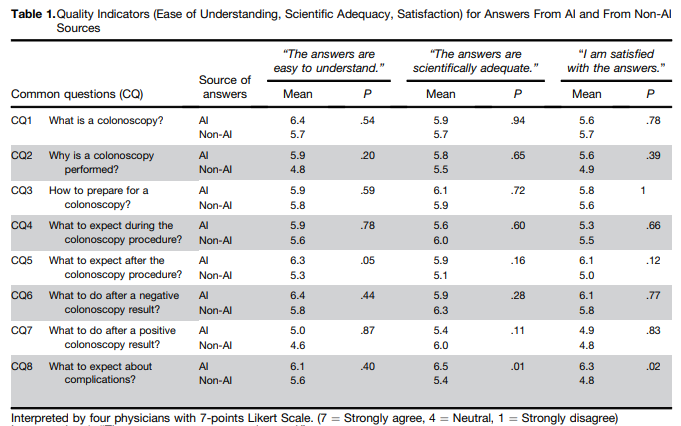
Methods: To objectively interpret the quality of ChatGPT-generated answers, 4 gastroenterologists (2 senior gastroenterologists and 2 fellows) rated 36 pairs of CQs and answers, randomly displayed, for the following quality indicators on a 7-point Likert scale: (1) ease of understanding, (2) scientific adequacy, and (3) satisfaction with the answer (Table 1) Raters were also requested to interpret whether the answers were AI generated or not.
Key findings:
ChatGPT answers were similar to non-AI answers, but had higher mean scores with regard to ease of understanding, scientific adequacy, and satisfaction.
The physician raters demonstrated only 48% accuracy in identifying ChatGPT generated answers
My take: This is yet another study, this time focused on gastroenterology, that show how physicians/patients may benefit from leveraging chatbots to improve communication.
The authors used data from ASPirin in Reducing Events in the Elderly (ASPREE), a randomized prospective trial of aspirin in the United States and Australia, including 18,934 community-based adults ≥65 years of all races/ethnicities (enrollment 2010-2014). Final cognitive testing was done in 2017. Key Findings:
Baseline PPI use vs nonuse was not associated with incident dementia (multivariable hazard ratio, 0.88, cognitive impairment without dementia (multivariable hazard ratio, 1.00), or with changes in overall cognitive test scores over time.
Also, no associations were observed between H2RA use and all cognitive endpoints.
My take: ” These data provide reassurance about the safety of long-term use of PPIs among older adults.” PPIs are unlikely to have negative effects on cognition.
In this retrospective study with 133 children (2008-2019), typical dosing of thiopurines: azathioprine 2-2.5 mg/kg/day and 6-mercaptopurine 1.5 mg/kg/day. Patients with previous or concomitant treatment with 5-ASA were allowed in the study. 62% (n=83) of the cohort had pancolitis. Key Findings:
Seventy-four patients (56%) had CS-free clinical remission at week 52 without rescue therapy
In the cohort in clinical remission, 67 and 51 patients had both CRP and calprotectin measurements at 1 year and end of follow-up. Sufficient biomarker response (CRP <1 mg/dL, calprotectin <250 mcg/g) was achieved by 44 (66%) and 44 (86%) at those two time points.
The likelihood of remaining free of rescue therapy among thiopurines-treated patients was 83%, 62%, 45%, and 37% at 1, 2, 3, and 4 years, respectively
8 of 133 (6%) stopped thiopurine therapy due to adverse effects
In their discussion, the authors make several points regarding efficacy and safety of thiopurines.
Many experts have advocated use of anti-TNF therapy agents for ulcerative colitis especially when 5-ASA medications are not effective.. This is based on higher efficacy and safety. With regard to safety, the authors note an “extremely low risk of lymphoma” citing a study from Israel in which children were followed until age of 30 years. No cases of hepatosplenic T-cell lymphoma were identified and the lymphoma rate was not statistically significant (O Atia et al. J Crohns Coliitis 2022; 16: 786-795 Open Access! Risk of Cancer in Paediatric onset Inflammatory Bowel Diseases: A Nation-wide Study From the epi-IIRN).
The authors note a recent review “rejected the hypothesis that initiation of biologic treatment later in the disease course correlates with lower response and remission rates in UC patients.”
Based on the efficacy and safety, the authors advocate for use of thiopurines “either early in the treatment course or as part of a de-escalation therapy…Thiopurines should be considered in the treatment of UC patients before the initiation of biologic drugs in most children.”
My take: In the U.S., it appears that thiopurine monotherapy, and even combination therapy, in pediatrics with IBD is used infrequently. Anti-TNF therapy with therapeutic drug monitoring is used routinely in patients if a 5-ASA is ineffective or not a good option. This article is a reminder that thiopurines are still a reasonable option. This would have been a good opportunity for a commentary in JPGN to add some context to this article regarding the role of these agents.
AGA guidelines for moderate-to-severe ulcerative colitis: “In adult outpatients with moderate to severe UC in remission, AGA makes no recommendation in favor of or against using biologic monotherapy or tofacitinib rather than thiopurine monotherapy for maintenance of remission.”
Most fundic gland polyps (FGPs) are small (0.1 to 1 cm) sessile polyps characterized histologically by cystic oxyntic glands with a mixture of parietal cells and chief cells.
Most FGPs are “sporadic” and associated with chronic PPI use. These are benign.
Syndromic FGPs are associated with familial adenomatous polyposis (FAP) and have a “0.6% lifetime risk of progressing to gastric carcinoma.” 73% of syndromic FGPs had low-grade dysplasia in one study.
Routine excision of FGPs is not recommended in the absence of high-risk features (see below)
In Figure 1, the authors outline an algorithm for surveillance:
Sporadic: If FGPs are thought to be sporadic and have no dysplasia, no follow-up is needed. If FGPs are thought to be sporadic, but have dysplasia, “consider diagnostic workup for syndromic FGP.” “Surveillance by EGD of sporadic FGPs with our without low-grade dysplasia is not routinely recommended, as progression to gastric cancer is rare… In patients with multiple FGPs (eg. carpeted polyposis), large (>1 cm) polyps, or the presence of high-grade dysplasia, FAP needs to be ruled via genetic testing and colonoscopy.”
Syndromic: If low risk FGP, then surveillance recommended beginning at 25 years of age. If high risk FGP, surveillance is recommended every 1-2 years. High-risk features include multiple FGPs (eg. carpeted polyposis), large (>1 cm) polyps, or the presence of high-grade dysplasia
In this review, the authors recommend VCE for Peutz-Jeghers syndrome no later than 8 years of age; for constitutional mismatch repair deficiency, the authors recommend “consider VCE surveillance before age 10.”
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
#2: Treatment options for supragastric belching may include brain–gut behavioral therapies, either separately or in combination, such as cognitive behavioral therapy, diaphragmatic breathing, speech therapy, and central neuromodulators.
#6: Abdominal imaging and upper endoscopy should be ordered in patients with alarm features, recent worsening symptoms, or an abnormal physical examination only.
#7: Gastric emptying studies should not be ordered routinely for bloating and distention, but may be considered if nausea and vomiting are present. Whole gut motility and radiopaque transit studies should not be ordered unless other additional and treatment-refractory lower gastrointestinal symptoms exist to warrant testing for neuromyopathic disorders.
#10: Probiotics should not be used to treat abdominal bloating and distention.
#11: Central neuromodulators (eg, antidepressants) are used to treat bloating and abdominal distention by reducing visceral hypersensitivity, raising sensation threshold, and improving psychological comorbidities.
Gastric belching: tracing showing instead a distal to proximal increase in impedance with air clearing from the esophagus. Arrows indicate direction of air flow and high-resolution manometric view of gastric belching is shown with direction of air flow from stomach to upper esophagus seen (orange arrow)
Several points from review:
Belching can be from the esophagus or from the stomach.
Supragastric belching involves air clearing from the esophagus not from stomach and is frequently associated with anxiety.
Gastric belching is frequently associated with reflux and occurs after spontaneous transient relaxation of the lower esophageal sphincter.
Bloating is a subjective sensation of fullness, tightness or trapped gas. Food intolerances, bacterial overgrowth, and celiac disease need to be considered. If constipation is present, this should be treated.
My take: This is a good review with plenty of practical suggestions for management.
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
Lately, I have been struck by the increasing volumes of research on disparities in medicine. A recent issue from the Journal of Pediatrics had at least 4 articles touching on this subject. Most of these articles view these disparities as being due to structural racism.
In this article, the authors show that among 519 children with newly diagnosed IBD, black patients were less likely to achieve CSFR (corticosteroid-free remission) 1-year post diagnosis (OR: 0.52, 95% CI:0.3-0.9) and less likely to achieve sustained CSFR (OR: 0.48, 95% CI: 0.25-0.92). This was despite a similar phenotype. Black patients had much higher rate of public insurance (58% vs 30%) and were less likely to be seen for routine follow-up visits.
While the authors attribute the response to therapy as likely to be related mainly to social determinants of health, there may be biologic factors at work as well. In a recent study (R Greywoode et al. Inflamm Bowel Dis 2023; 29: 843-849. Open Access! Racial Difference in Efficacy of Golimumab in Ulcerative Colitis), there were disparate racial response rate differences among patients receiving the same therapy.
In this retrospective review of 38,334 specialty referrals (2019-2021), of all referrals, 62% were scheduled and 54% were completed. Referral completion rates were lower for patients with Black race (45%), Native Hawaiian/Pacific Islander race (48%), Spanish language (49%), and public insurance (47%). Since the report focused on primary clinics within 5 miles of the hospital, the authors indicate that the lower referral completion is due to nongeographic structural barriers, including problems with arranging visits as some families have less flexible jobs. The authors conclude that the fact that specialty care is inaccessible is due to ” the effects of racism and discrimination on the scheduling process.” The authors recommend that the referral workflows should not “place the administrative onus of scheduling exclusively on families.”
This was a retrospective cohort analysis of linked birth and death certificates from 50 states from 2005 to 2014 to investigate among US infants born at <37 weeks gestation (a) racial and ethnic disparities in sudden unexpected infant death (SUID). Key findings:
Among 4,086,504 preterm infants born during the study period, 8096 infants (0.2% or 2.0 per 1000 live births) experienced SUID. State variation in SUID ranged from the lowest rate of 0.82 per 1000 live births in Vermont to the highest rate of 3.87 per 1000 live births in Mississippi
In the adjusted analysis (for sociodemographic and clinical factors), compared with Non-Hispanic white infants, Non-Hispanic black infants and Alaska Native/American Indian preterm infants had greater odds of SUID (aOR, 1.5)and aOR, 1.44)
The authors attribute the adjusted differences to “structural racism [that] creates and perpetuates health inequities.”
This was a retrospective cohort study of 3290 infants hospitalized in a single center NICU between 2017 and 2019 in the Racial and Ethnic Justice in Outcomes in Neonatal Intensive Care (REJOICE) study. Key findings:
205 families (6.2%) that experienced an adverse social event. Black families were more likely to have experienced a CPS referral and a urine toxicology screen (OR, 3.6). American Indian and Alaskan Native families were also more likely to experience CPS referrals and urine toxicology screens (OR, 15.8 and OR, 7.6)
Black families were more likely to experience behavioral contracts and security emergency response calls
My take: These articles offer more proof that racial disparities are highly prevalent in healthcare. While we should strive to help improve access/equitable care in medicine, the approach needs to start well before the clinic/hospital. To make the greatest impact, policies are needed to address education outcomes and poverty (eg. expanded child income tax credit) which overall impact health more than anything that happens in our clinics.
Safe Sleep A terrific website that focuses on this crucial issue: Charlieskids.org; it has videos, do’s and don’ts as well as a link to Cribs for Kids (discounted safe crib website). In addition, this website has a book called “Sleep Baby Safe and Snug” which incorporates updated recommendations on safe sleep practices.
The High Toll of Sudden Infant Death From 2013-2015, there was an average of 3523 US infants each year who died from SUID (sudden unexpected infant death), peaking at 1-2 months of life. More black infants died of SUID in the first year than black children who died from firearm homicides in all of childhood through age 19 years. SUID deaths from 2013-2015 (10,568) was similar to the total number of motor vehicle-traffic deaths in all of childhood (10,714) and greater than the total number of any of the other causes.
In this retrospective study with 18 pediatric patients (2019-2021) who presented with pediatric acute liver dysfunction, the authors examined the yield of rapid whole genome sequencing (rWGS). Key findings:
Median turnaround was 8 days. In patients with a diagnostic study, an initial report was received in a median of 4 days compared to 10 days with a non-diagnostic study.
7 patients (39%) had diagnostic results including two with ornithine transcarbamylase deficiency, one with Wilson’s disease, one with PFIC type 1, one with infantile liver failure syndrome 2 (due to NBAS gene), one with GSD type 4, and one with infantile liver failure syndrome 1 (due to LARS gene).
Five of these patients with abnormal rWGS had liver transplantation evaluation/listing after the test results were received
One annoying aspect of the report is the authors’ attempt to suggest that the diagnostic yield should have been higher if they excluded four patients subsequently thought to have liver dysfunction due to environmental exposures. In a retrospective study, it is easy to second-guess and say that the test could have been used more selectively.
My take: This study shows that rapid whole genome sequencing is a very valuable part of the evaluation of children with severe liver dysfunction. Turnaround times have improved considerably.
R Paknikar et al. NEJM 2023; 389: 1321-1326. Digging into the Histology
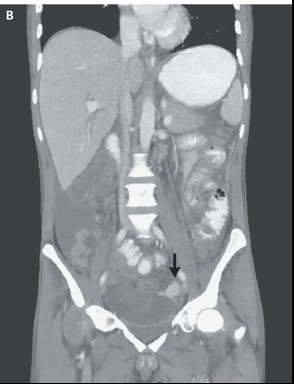
In this case report, a 33-year-old man (from the midwest) with ulcerative colitis (diagnosis seven years prior) who was receiving treatment with tofacitinib (a Janus kinase inhibitor) presented to the hospital with fatigue (x 8 months) and bloody diarrhea. He also had had fevers (x 4 months), 23 lb weight loss, and drenching night sweats. Before tofacitinib, treatment had included adalimumab and azathioprine. He had undergone a sigmoidoscopy two months prior to presentation.
His workup included a CXR showing diffuse reticulonodular opacities, a CT scan showing thickening in the colon and extensive infection workup. On the third hospital day, he had a perforation and resection which led to the diagnosis of invasive histoplasmosis.
My take: This article is useful for understanding how to workup secondary infections in IBD patients on long-term immunosuppressive agents.
One example: “testing for 1,3-β-d-glucan can serve as an adjunctive test for invasive fungal infections caused by fungi expressing 1,3-β-d-glucan in their cell walls, including candida, aspergillus, Pneumocystis jirovecii, Histoplasma capsulatum, and coccidioides; such testing has a high negative predictive value for infection with these organisms. In contrast, cryptococcus and blastomyces produce very low levels of 1,3-β-d-glucan in their cell walls and are therefore not readily detected by serum testing for the cell-wall antigen.”
CT showed shows diffuse wall thickening in the rectosigmoid colon and extravasation of extraluminal contrast material (arrow) into the area adjacent to the sigmoid colon, with layering of the contrast material, findings that are thought to indicate a perforation.
Key finding: This case report documents two cases of medically-treated necrotizing enterocolitis (NEC) that developed shortly after Onasemnogen Abeparvovec which was administered at ~3 weeks of life in two full term infants (born at 40 and 41 weeks).
My take: Consider the diagnosis of NEC in full term infants with SMA who have received gene therapy.
Views from Bike Trail near Ospedaletti, ItalyWhile grabbing a snack & taking a break from our bike ride, we saw all of these wind surfers. The wind on this day was crazy and these surfers looked like they were going 30-40 mph