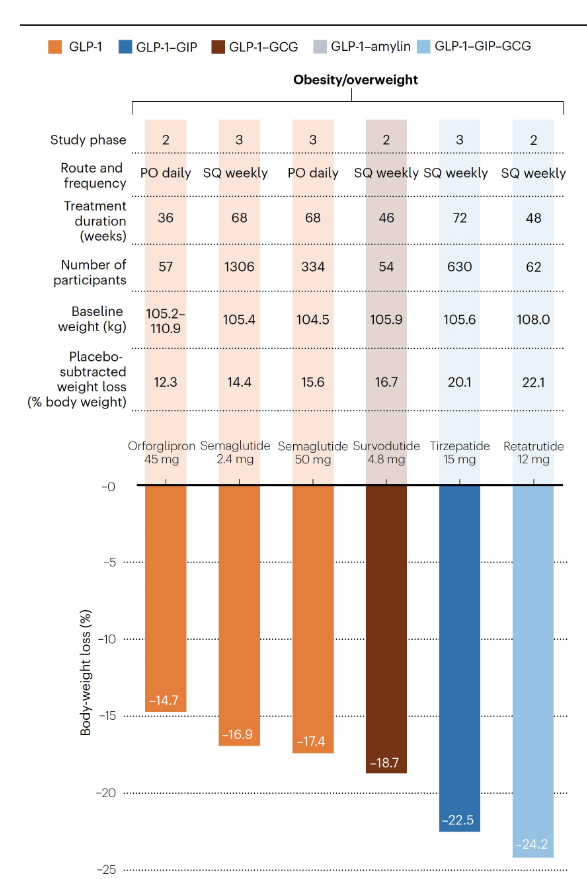
Eric Topol: “The GLP-1 and now triple G-Agonists are exceeding expectations as weight loss drugs. Benefits for cardiovascular outcomes, possibly Type 1 diabetes, addiction, and more are reviewed in the latest Ground Truths.” His newsletter also describes the early results of these medications with MASH/NASH with improvement in ~90%.
To get the full review, go to Ground Truths: http://erictopol.substack.com (can sign up to get regular emails on many current medical topics)
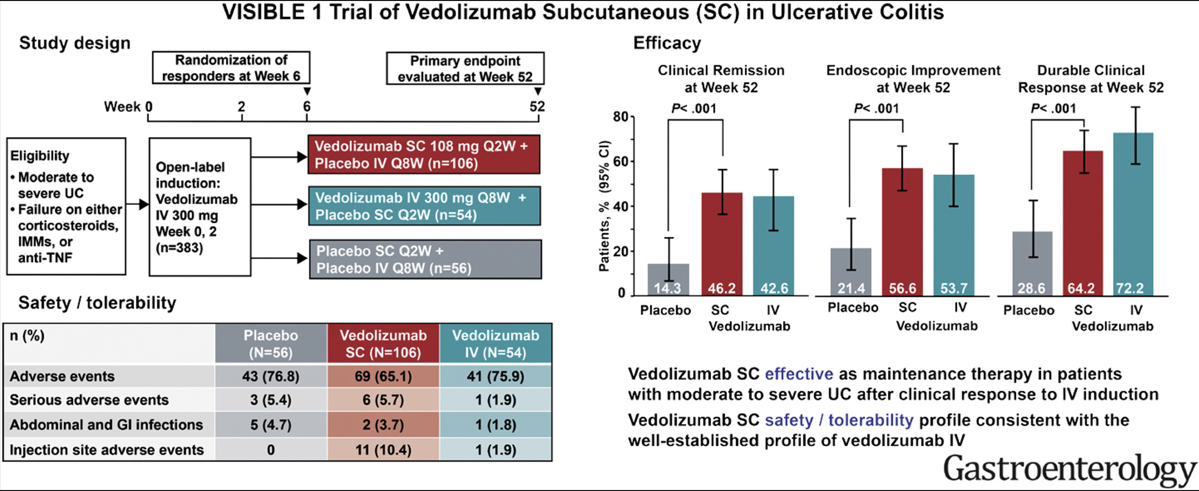
” Takeda (TSE:4502/NYSE:TAK) today announced that the U.S. Food and Drug Administration (FDA) has approved a subcutaneous (SC) administration of ENTYVIO® (vedolizumab) for maintenance therapy in adults with moderately to severely active ulcerative colitis (UC) after induction therapy with ENTYVIO intravenous (IV).1 ENTYVIO SC is expected to be available in the U.S. as a single-dose pre-filled pen (ENTYVIO Pen) by the end of October. Additionally, a Biologics License Application for an investigational SC administration of ENTYVIO for the treatment of adults with moderately to severely active Crohn’s disease is currently under review by the FDA.”
There are a bunch of new videos (one for everyday in September) similar to this on related topics -search 30 Days of US Healthcare. Here’s another one: 30 Days of US Healthcare: Surprise Billing (YouTube)
My take: As usual, Dr. Glaucomflecken humor sheds light on the faults in our nation’s health care insurance coverage.
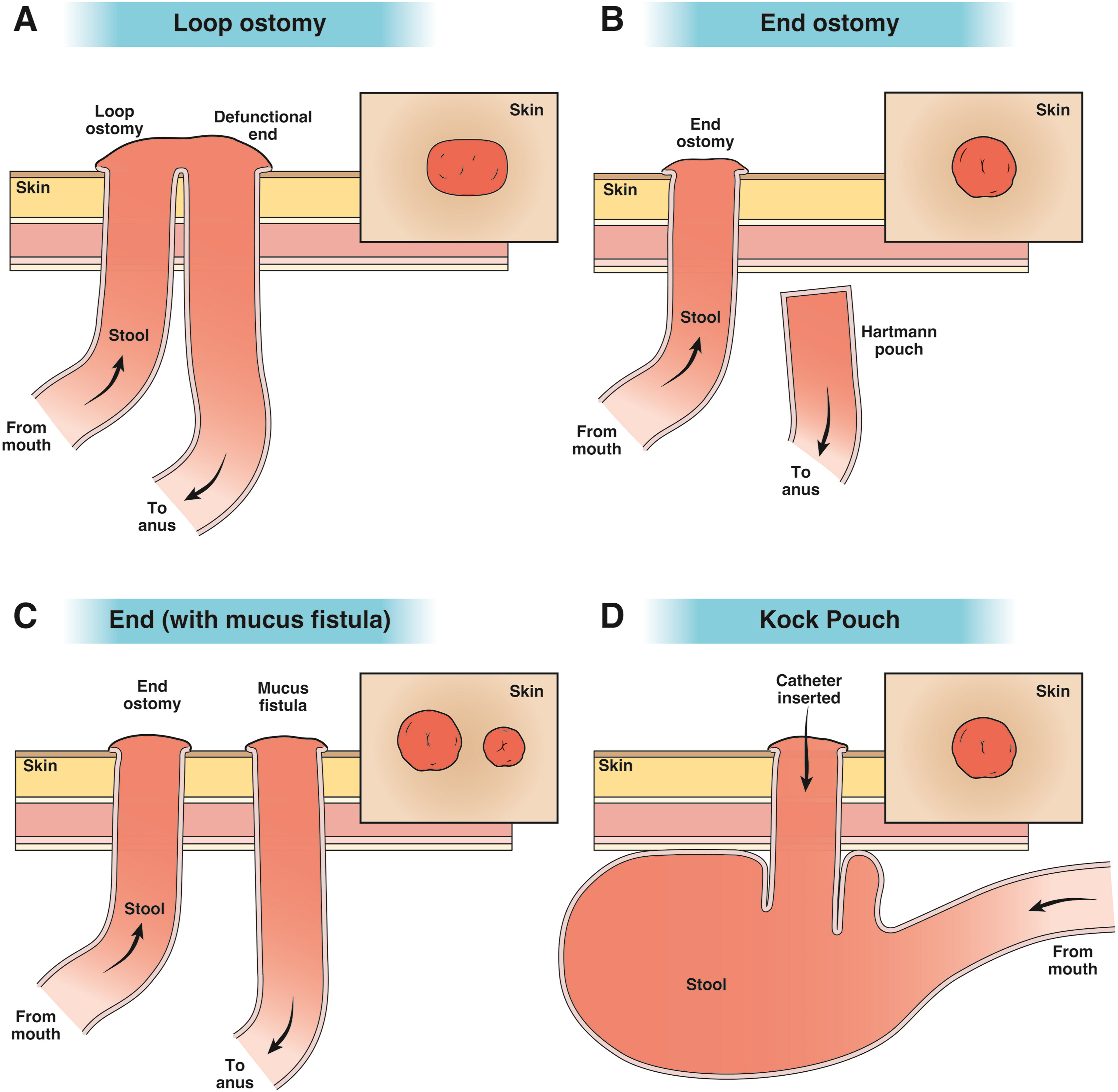
This article is a helpful review on ostomy care. The article reviews approaches to common problems including early high ostomy output, ostomy leakage, stoma retraction, mucocutaneous separation, dermatological problems, chronic high ostomy output, parastomal hernia, and stoma prolapse. A few of their comments:
“An estimated 750,000 Americans live with an ostomy and 130,000 new ostomy surgeries occur in the United States annually.1“
“Reversal [of ostomy] before 6 weeks of the index surgery is associated with an increased risk of complications”
For leakage of ostomy: “Management steps involve thickening the stool with antidiarrheals to facilitate a more solid effluent and pouching techniques to bolster the height of the stoma off the peristomal skin (eg, convex appliance, ostomy belt, paste, or barrier rings). Each of these items is available through the patient’s medical equipment supplier. Additional pearls include heating the appliance with a hair dryer before application, lying flat for several minutes after application, ensuring the peristomal skin is dry before application, and use of a fine dusting of stomal powder followed by skin sealant on the peristomal skin before application.”
Stoma prolapse: “The rate of stomal prolapse is 5% to 10%.12 Acute prolapse can lead to incarceration and ischemia, which presents as pain, obstipation, and purple/black discoloration of the stoma…In the absence of ischemia, the prolapse may be reduced by laying the patient in a relaxed position and gently squeezing the ostomy back into the abdomen. If the stoma cannot be reduced with pressure alone, a cup of sugar applied directly to the stoma and left in place for 20 minutes can reduce stomal swelling and facilitate reduction of the prolapse. Surgery can be avoided if the prolapse is mild, easily reducible, and does not interfere with pouching.”
Medications for High Ostomy Output include bulking agents (fiber, guar gum, marshmellows), antimotility agents (eg. loperamide, diphenoxylate/atropine), and antisecretory agents (PPIs, Octreotide). Treatment of specific underlying disease may help, such as anti-inflammatory agents for IBD and GLP-2 analogues for short bowel.
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
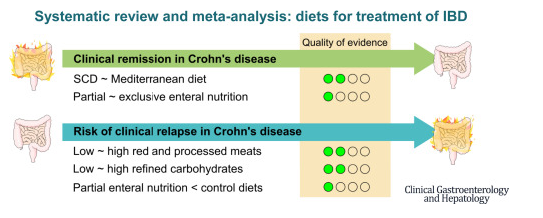
This was a systematic review of prospective controlled trials (n=27) of solid food diets for the induction or maintenance of remission in IBD.
Key findings:
For induction of remission in Crohn’s disease (CD), the Mediterranean diet was similar to the Specific Carbohydrate Diet (low certainty of evidence), and partial enteral nutrition (PEN) was similar to exclusive enteral nutrition (very low certainty of evidence).
PEN reduced risk of relapse (very low certainty of evidence), whereas reduction of red meat or refined carbohydrates did not (low certainty of evidence).
For ulcerative colitis, diets were similar to controls (very low and low certainty of evidence).
My take: Most of the dietary treatments for IBD have low to very low certainty of evidence regarding their effectiveness. Dietary changes are very likely to be helpful but more studies with rigorous endpoints are still needed.
In this retrospective study with adult patients (n=339) referred specifically to a tertiary center for evaluation of gastroparesis (GP) from 2019-2021, the key findings:
Nausea was most common symptom (in 89%), followed by abdominal pain (76%, constipation (71%), vomiting (66%), bloating (38%) and early satiety (35%)
196 (58%) had undergone a prior gastric emptying study; though only 23 (7%) had ingested radiolabeled eggs as the test meal.
66 (19.5%) ultimately received a diagnosis of GP; 80.5% received alterative diagnosis including functional dyspepsia in 44.5%. In those with GP, diabetes was more common (40% vs. 17%, P=.017).
GP patients more often had retained food in the stomach during EGD (23% vs. 11%, P=.013)
My take: In adults (& probably in children), most individuals labelled as having gastroparesis actually have an alternative explanation, usually functional dyspepsia. The symptoms are indistinguishable and improperly performed scintigraphy contributes to confusion.
Until a few years ago, I had controlled my depression and anxiety through decades of counseling. I was reluctant to try medications because the medical understanding of them seemed vague…We also can’t explain why some people benefit from S.S.R.I.s and others do not. Because of this, many people still believe those who take them don’t really need them. I also believed that, if I was strong enough, I didn’t need medication…
I was wrong to doubt. It’s had a remarkable effect on my mood, and almost everyone around me noticed the difference. I was more optimistic, friendlier and more engaging. I was forced to reconsider why I had avoided taking the medication for so long. I think it’s because — even though I realize this isn’t true — taking it felt like an admission of failure…
I’ve recently faced a similar scenario with new drugs for obesity. I’ve struggled with my weight for most of my life. I’ve always been overweight, and in the last few years, I’ve slipped into obesity, according to my body mass index. I exercise regularly and carry the weight well, but it bothers me immensely. It especially troubles me because I have a fair amount of self-discipline and eat quite healthfully…
Despite all the advances in science, we don’t know why some people, even when they try desperately, can’t seem to lose weight. Because of that, we often assume it must be a lack of willpower…
These drugs are expensive, but I was determined to see what would happen if I took one. It is hard to explain what life is like on this medication to people who don’t have trouble controlling their weight. I’m not hungry all the time. I’m not thinking about food incessantly. I’m not obsessing about what I wish I could eat and what I can’t. My mental health, and even my temperament, improved so much that my whole family rejoiced…
Before writing this essay, I had told just a few people I’m on the drug. I think it’s because, on some level, I still feel shame. I felt the same when I finally started taking an antidepressant…
Medical treatments should not be dismissed just because we don’t fully grasp their mechanisms; people who use them are not cheating.
C Gamble et al. NEJM 2023; 389:795-807. Timing of Primary Surgery for Cleft Palate
Conclusion from study authors: Medically fit infants who underwent primary surgery for isolated cleft palate in adequately resourced settings at 6 months of age were less likely to have velopharyngeal insufficiency at the age of 5 years than those who had surgery at 12 months of age.
The associated editorial (R Tse, O Jackson, N Engl J Med 2023; 389:857-858. Mind the Gap) notes that “over two thirds of infants who were screened were excluded because their cleft was part of a syndrome, they were deemed to be medically unfit for early surgery, or they had a cleft that was too wide.” Also, “the incidence of additional surgery to treat velopharyngeal insufficiency was greater in the 6-month group than in the 12-month group (30 procedures in 27 children vs. 17 procedures in 16 children), and speech assessments performed after the secondary procedures were used in the analysis. Thus, the trial evaluated the mixed effects of primary surgery and secondary surgery in some patients.” Finally, “the considerations with regard to early surgery include the greater technical complexity of the procedure and the greater risks associated with anesthesia (airway complications and potential neurodevelopmental sequelae). Early surgery may also contribute to midfacial growth restriction, which becomes apparent only later, in adolescence, and may require complex corrective jaw surgery.”
My take: Early cleft palate surgery is not best for all infants with this defect.
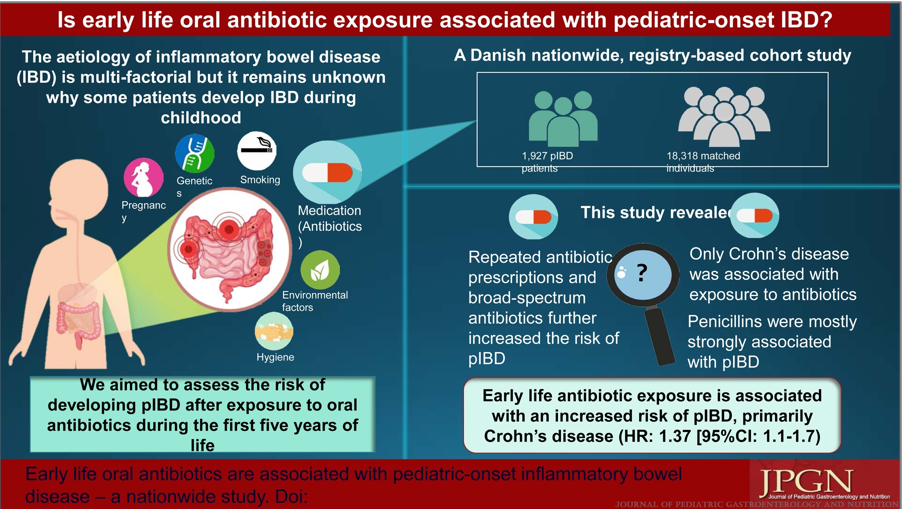
Oral antibiotic exposure during the first 5 years of life was associated with a higher risk of developing pIBD (HR = 1.33, P <0.0001). The risk was also increased if patients had ≥4 antibiotic prescriptions compared to no antibiotics (HR = 1.33, P <0.0001).
Broad-spectrum antibiotics increased the risk of pIBD compared to narrow-spectrum antibiotics (HR = 1.29, P < 0.0001).
When stratified by IBD subtypes, only Crohn disease was significantly associated with exposure to antibiotics (HR = 1.37, P = 0.002).
My take: This study indicates that antibiotics (and/or serious infections) are associated with an increased the risk of pediatric Crohn’s disease but the absolute risk is very low. We still have a lot to learn about how environmental exposures, including diet, infections, antibiotics, and pollution, contribute to the increasing prevalence of inflammatory bowel disease.
Related blog posts:
Early Antibiotics -Minimal Risk for Crohn’s Disease The cumulative risk of CD at the 11th birthday for children exposed to antibiotics in their first year of life was 0.16% compared to 0.11% for children unexposed to antibiotics in their first year of life.
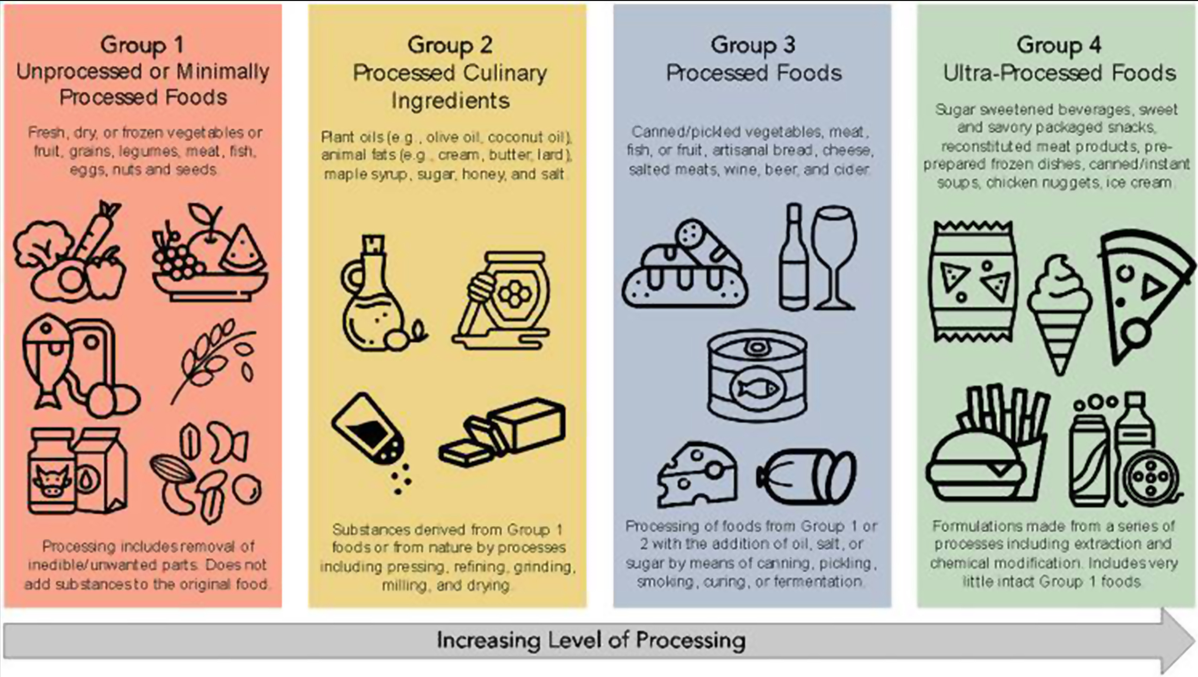
Figure 1 from editorial: The NOVA classification of food
A total of 1,068,425 participants were included (13,594,422 person-years) among 5 cohort studies published between 2020 and 2022. The average age of participants ranged from 43 to 56 years. Key findings:
Crohn’s disease: During follow-up, 916 participants developed CD, and 1934 developed UC. There was an increased risk for development of CD for participants with higher consumption of ultra-processed foods compared with those with lower consumption (HR, 1.71; 95% CI, 1.37–2.14; I2 = 0%) and a lower risk of CD for participants with higher consumption of unprocessed/minimally processed foods compared with those with lower consumption (HR, 0.71; 95% CI, 0.53–0.94; I2 = 11%).
Ulcerative colitis: There was no significant association between risk of UC and ultra-processed foods (HR, 1.17; 95% CI, 0.86–1.61; I2 = 74%) or unprocessed/minimally processed foods (HR, 0.84; 95% CI, 0.68–1.02; I2 = 0%).
The associated editorial by Fitzpatrick et al, notes that “there are plausible mechanisms that explain the associations of higher UPFs and development of CD, such as: (1) displacing the intake of minimally processed foods and subsequently reducing exposure to beneficial micronutrients, antioxidants, and phytochemicals; (2) driving overconsumption of total calories7; and (3) increasing exposure to non-nutritive food substances that have been implicated in the development of CD in pre-clinical studies…The notion is that a lower UPF intake is better, but a cutoff value remains elusive.”8
My take (borrowed from editorial): “the population studies have indicated that the extremes of UPF intake are related to risk of CD and that such associations are underpinned by plausible biological mechanisms, suggesting causality.”