A group of 23 experts followed a rigorous process over a 1-year period to assess the quality of evidence and develop consensus statements regarding the medical management of ulcerative colitis (UC) in adults (Bressler B, Marshall JK et al. Gastroenterol 2015; 148: 1035-58, editorial 877-80).
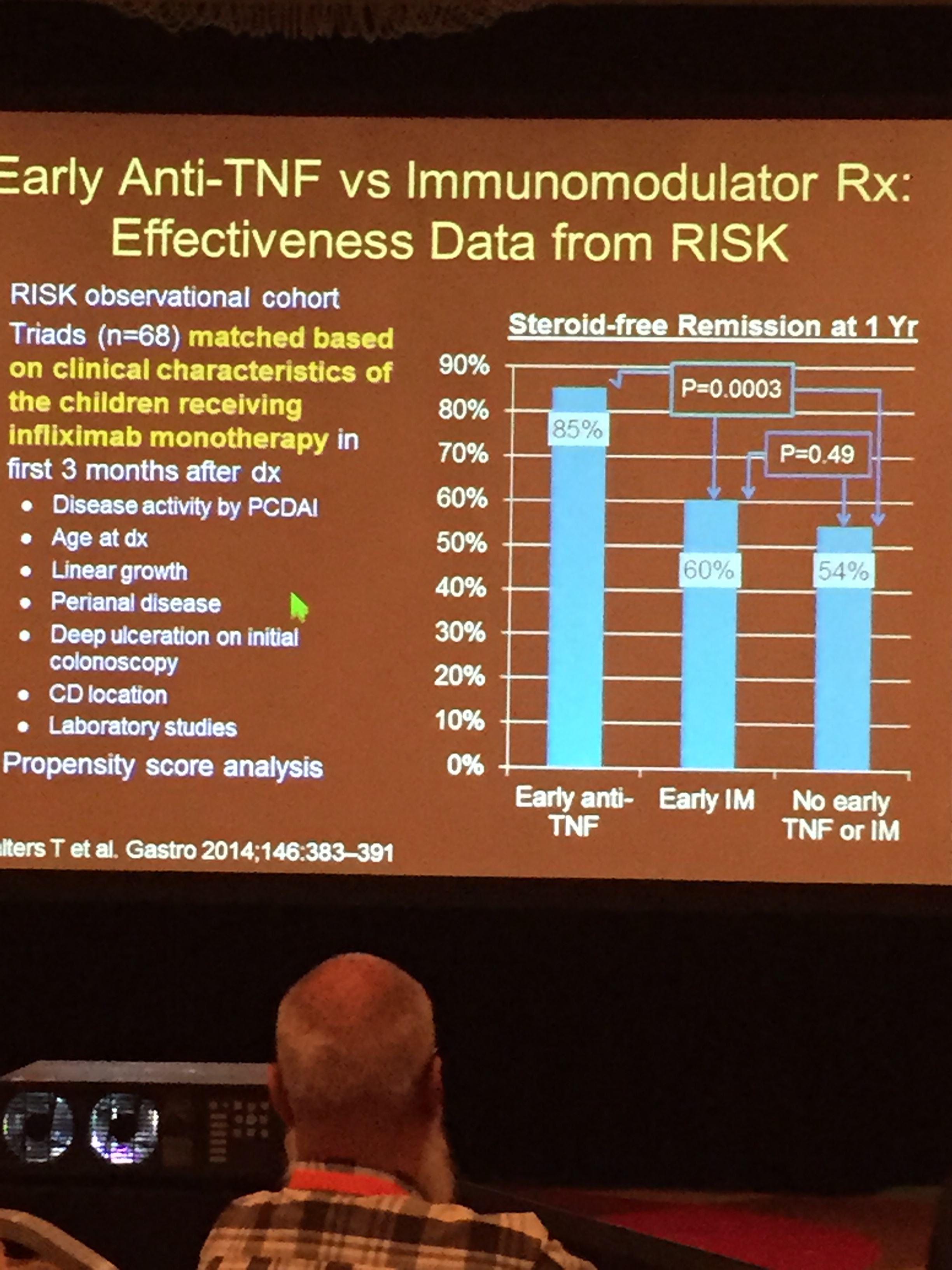
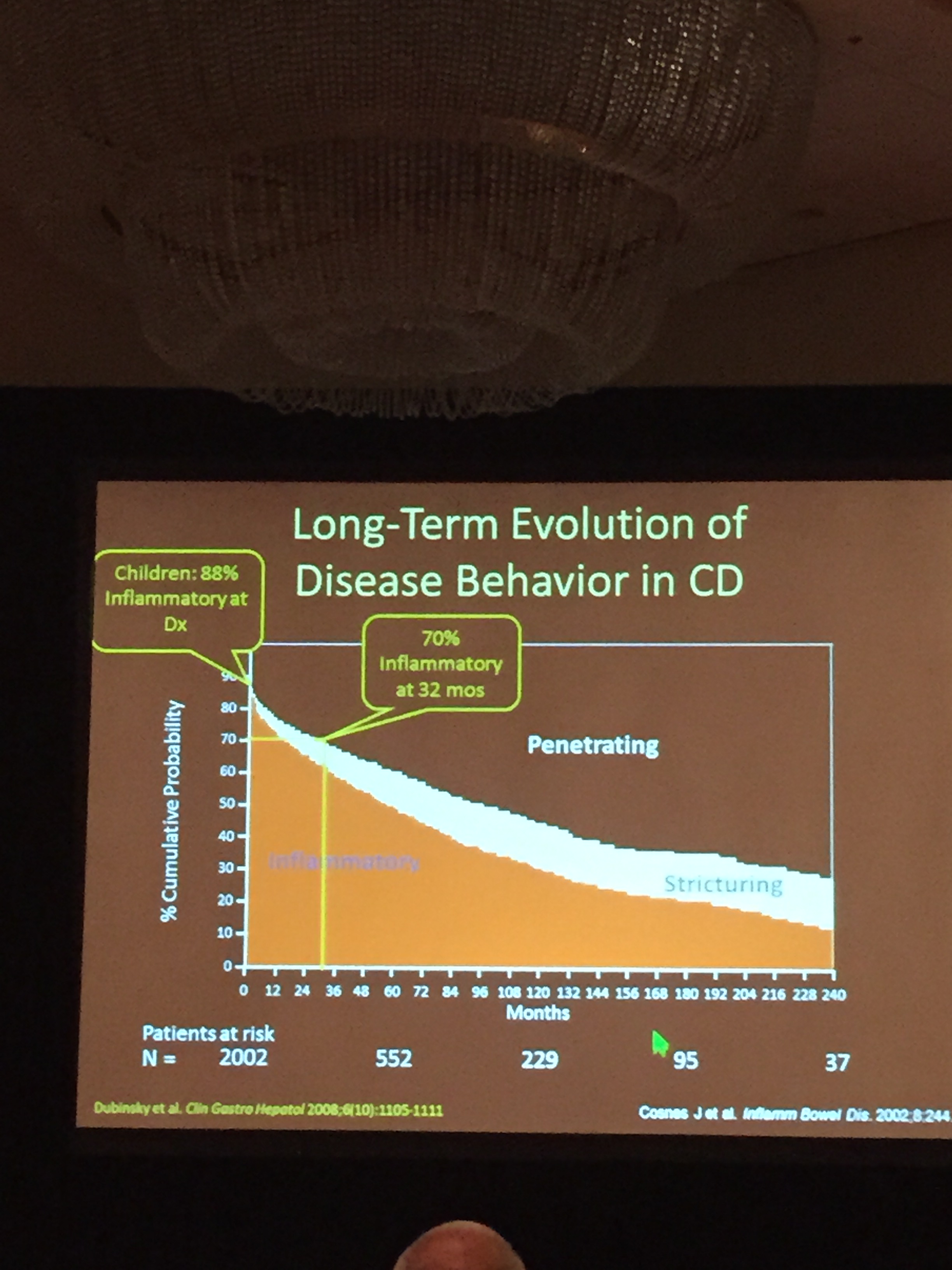
The need for updated guidelines has emerged due to practice variation related in part to a wider availability of treatments and diagnostic tools. It is recognized that early institution of effective therapy is associated with the best outcomes. In addition, due to the chronic nature of ulcerative colitis and the potential for reduced durability of biologic agents, careful decision-making can improve response.
Table 4 in the article summarizes the recommendations. I will list a few:
1. Thiopurines:
- “In patients with UC, we recommend against the use of thiopurine monotherapy to induce complete remission.”
- In selected patients, “we suggest thiopurine monotherapy as an option to maintain complete corticosteroid-free remission.”
2. Anti-TNF therapy:
- “In patients with UC who fail to respond to thiopurines or corticosteroids, we recommend anti-TNF therapy to induce complete corticosteroid-free remission.”
- “When starting anti-TNF therapy, we recommend it be combined with a thiopurine or methotrexate rather than used as monotherapy to induce complete remission.”
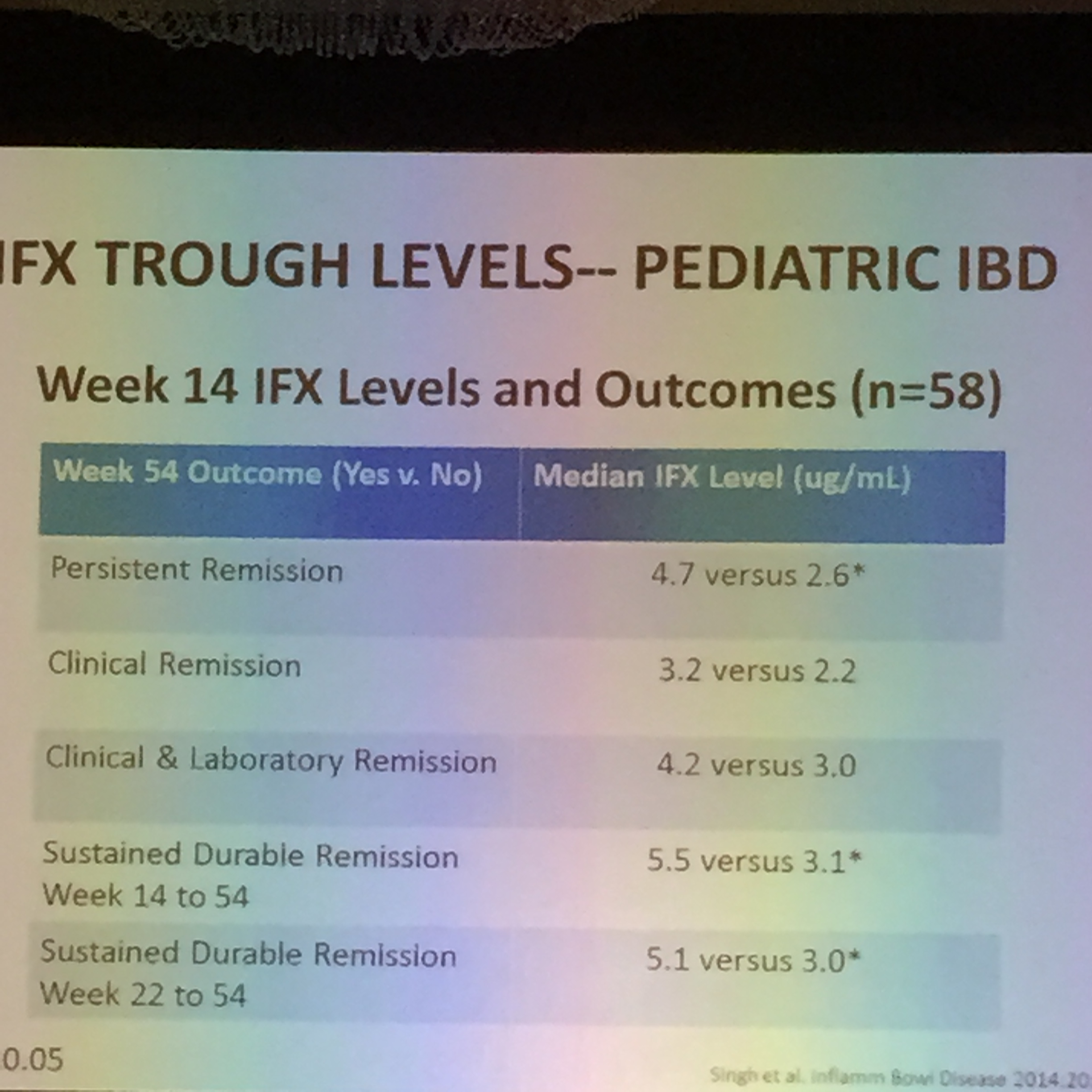
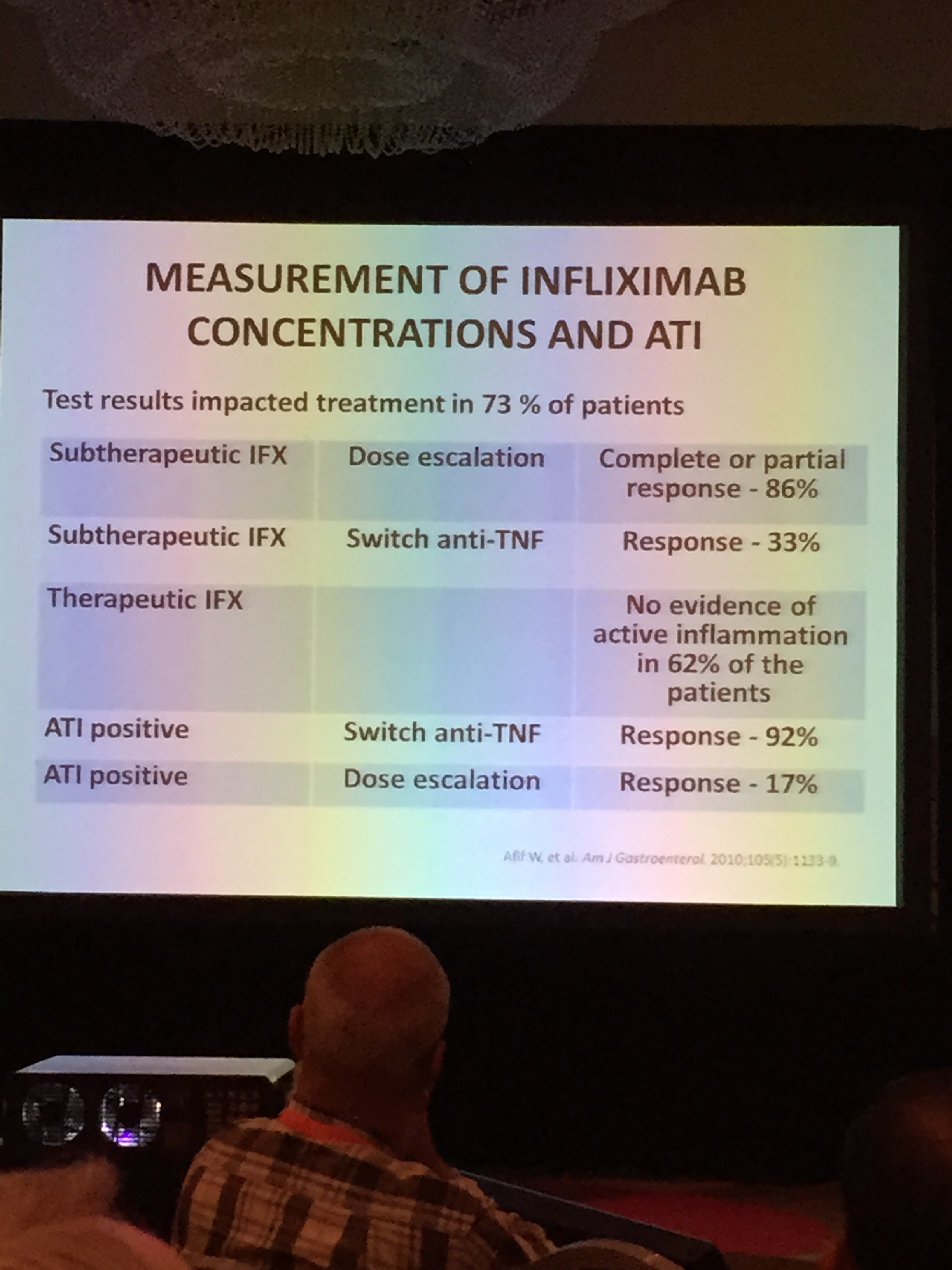
- For UC patients with suboptimal response or for those who lose response to anti-TNF therapy, “we recommend dose intensification.” Dose optimization should be informed by therapeutic drug monitoring.
3. Vedolizumab
- Vedolizumab is recommended with primary anti-TNF failure (rather than switching to an alternative anti-TNF), whereas either a 2nd anti-TNF or vedolizumab is recommended with secondary anti-TNF failure based on therapeutic drug monitoring.
4. Fecal microbial transplant (FMT)
- “We recommend against FMT…outside the setting of a clinical trial.”
5. 5-ASA and Corticosteroids
- Rectal 5-ASA is recommended at 1 g daily for mild-to-moderate ulcerative proctitis. 5-ASA enemas are recommended for mild-to-moderate left-sided ulcerative colitis.
- In patients with moderate-to-severe UC, corticosteroids are recommended as 1st line therapy for induction of remission but not for maintaining remission. In addition, corticosteroids are recommended as 2nd-line agents for inducing remission in those with mild-to-moderate disease who do not respond to 5-ASA products.
With all of the treatments, the authors recommend followup to assure response to therapy; this followup ranges from within 2 weeks for steroids, to 4-8 weeks with 5-ASA products, to 8-14 weeks for biologic agents.
Overall, the emphasis of this consensus statement is on maximizing the response to biologic agents. By optimizing dosing and using combination therapy, the treatment guidelines aim to lower rates of antidrug antibody formation. This in turn should improve results and is in agreement with data from both the SONIC study and the UC-SUCCESS study.
The editorial comments that methotrexate “may be an attractive option for young male patients;” however, “the absence of data on risk of malignancy with methotrexate in IBD may reflect lower frequency of use for this indication.”
While these guidelines will be useful, there are many unanswered questions (discussed in editorial).
- In patients on combination therapy, what is the optimal dose of the immunomodulator?
- When or Should the immunomodulator be withdrawn?
- For secondary failure, should a 2nd anti-TNF be used prior to vedolizumab?
- How should these guidelines be tailored for the pediatric population (or the elderly)?
- What is the optimal monitoring for UC patients with regard to biomarkers and endoscopy?
- What is the appropriate role of therapeutic drug monitoring?
Bottomline: These guidelines are likely to promote the use of more combination therapy and help define the current role of vedolizumab.
Related blog posts:
- UC SUCCESS | gutsandgrowth
- Source Article: Methotrexate Safety | gutsandgrowth
- Digging into the COMMIT Study | gutsandgrowth
- Enthusiasm for Vedolizumab | gutsandgrowth
- Vedolizumab -another new IBD treatment | gutsandgrowth
- More NASPGHAN Meeting Notes: IBD Hot Topics – gutsandgrowth
- What you might not know about anti-TNF monitoring …
Disclaimer: These blog posts are for educational purposes only. Specific dosing of medications/diets (along with potential adverse effects) should be confirmed by prescribing physician/nutritionist. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.