NPR: From Camping To Dining Out: Here’s How Experts Rate The Risks Of 14 Summer Activities
This article describes the potential risks for dining out, staying at hotels, getting a haircut (ask your stylist to focus on cutting and not talking), going to the beach/pool and other activities.
Moving NY Times Graphic on coronavirus toll in U.S. (May 24, 2020): An Incalculable Loss: Remembering the Nearly 100,000 Lives Lost to Coronavirus in America
A recent lecture by Dave Stukus: Deep Down the Rabbit Hole of Biases, Conspiracies, and Echo Chambers (50 minutes). Thanks to Ben Gold for this reference.
This lecture summarizes some of the challenges of misinformation and quackery.
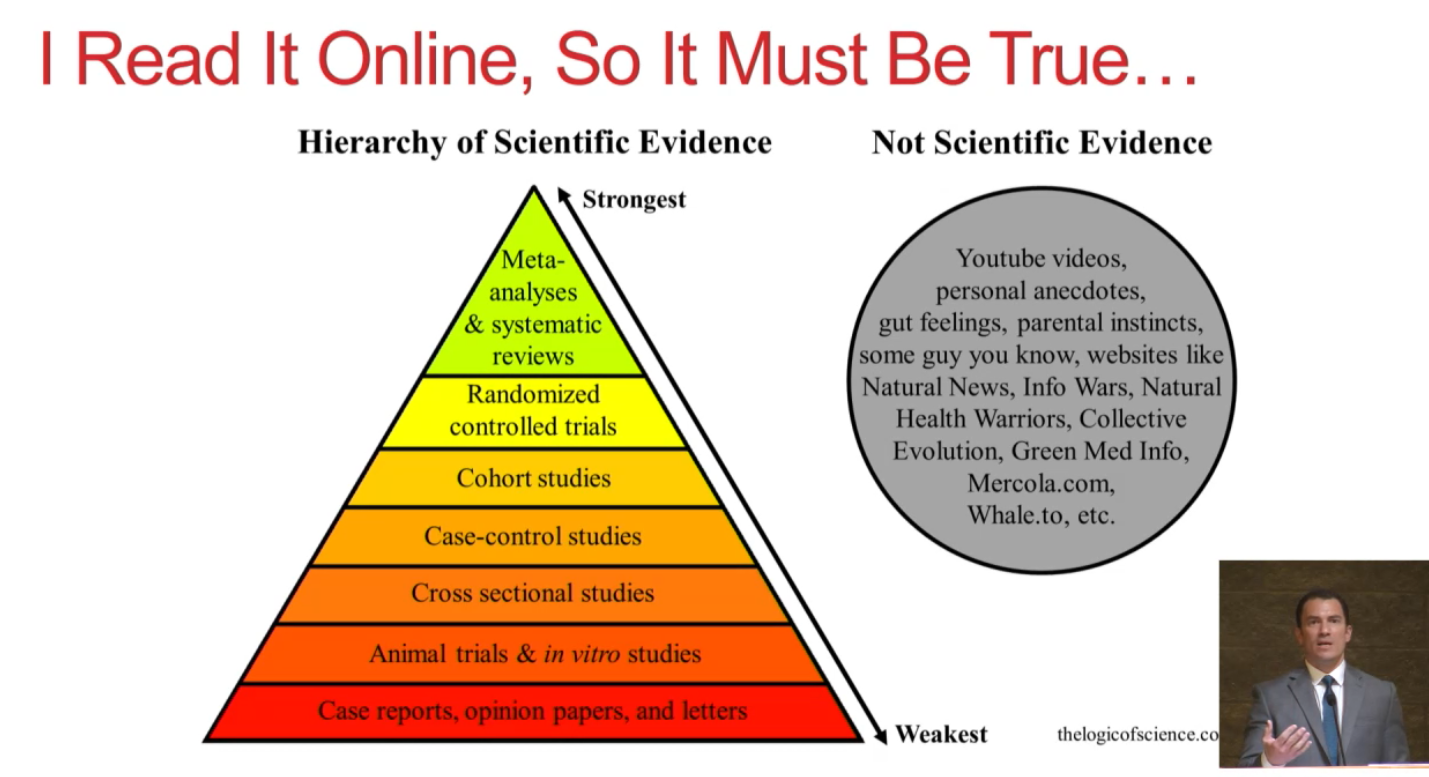
Some interesting points:
- Explains common biases which lead us to faulty conclusions
- Illustrates some far-fetched claims for Himalayan Salt Lamp as a treatment for asthma as well as Dr. Oz’s unproven recommendations for the coronavirus
- Provides several books for those interested in learning a lot more (see last slide)
Some slides:











Related blog posts:
- “The Truth About Allergies and Food Sensitivity Tests”
- War on Science and Genetically-Modified Foods
- Alan Alda (aka Hawkeye Pierce) on Communicating Science …
- NPR: “Should You Trust That New Medical Study?” | gutsandgrowth
- Why I have always liked Arthur Caplan… | gutsandgrowth
- How to Understand Scientific Studies | gutsandgrowth
- Short Take on Understanding Bias | gutsandgrowth